
Abstract
Objective:
The aim of the present study is to elucidate factors contributing to early recovery of urinary continence after robot-assisted laparoscopic radical prostatectomy (RARP) from the perspective of urethral and vesical anatomical features after RARP.
Patients and Methods:
Sixty consecutive patients undergoing RARP also underwent pre- and postoperative urethrovesicography (UVG). Both pre- and postoperative UVG evaluated the posterior-urethral vesical angle and position of the urethrovesical junction. Postoperative UVG was performed 7 days after RARP and also evaluated postoperative membranous urethral length (MUL) and the postoperative degree of atony of the external urethral sphincter. Associations were analyzed between pre- or postoperative UVG variables and urinary incontinence as well as between UVG variables significantly correlating with urinary incontinence and neurovascular bundle-preservation procedures.
Results:
Postoperative MUL was the only factor significantly associated with the state of continence in the early postoperative period according to multivariate logistic regression analysis (odds ratio, 1.94; 95% confidence interval, 1.22–3.12; p<0.005). A cutoff value of 17 mm offered the best accuracy in receiver operating characteristics analysis. Postoperative MUL was significantly increased in the group with preservation of the neurovascular bundle (p=0.01).
Conclusions:
Postoperative MUL is the most important factor for recovery of urinary continence in the early postoperative period after RARP. Postoperative MUL >17 mm as measured on UVG can be expected to predict early recovery of urinary continence. Postoperative MUL was greater with preservation of the neurovascular bundle, thus allowing early recovery of urinary continence.
Introduction
R
Radical prostatectomy, including RARP, induces anatomical changes to the lower urinary tract caused by removal of the prostate and subsequent reanastomosis of the urethra and bladder neck. Although a small number of studies have specifically addressed relationships between morphology of the lower urinary tract after radical prostatectomy and urinary incontinence, 4 –6 no studies specific to RARP have been described, especially for the early postoperative period.
Several surgeons have demonstrated that modified surgical procedures for RARP aimed at achieving early recovery of urinary continence and can offer good outcomes. 7 –9 In addition, neurovascular bundle- or plate-preservation procedures have an increased likelihood of allowing an early return of urinary continence. 10,11 The basic concept underlying intraoperative techniques to improve early return of urinary continence after radical prostatectomy is to maintain normal anatomical and functional structures in the pelvis as much as possible. 12 However, the reasons why those procedures allow early acquisition of urinary continence have not been adequately revealed from the perspective of urethral and vesical anatomical features after RARP.
The aim of the present study was to investigate correlations between pre- and postoperative morphology of the bladder and urethra and urinary incontinence after RARP to elucidate factors contributing to early acquisition of urinary continence. In addition, we investigated correlations between aspects of the morphology of the bladder and urethra showing statistical correlations to urinary incontinence in the early postoperative period and neurovascular bundle-preservation procedures, to elucidate the mechanisms underlying early acquisition of urinary continence following surgical procedures.
Patients and Methods
Patients
Participants in this prospective clinical cohort observational study comprised 60 consecutive patients who underwent RARP at our institution between February 2013 and August 2013. All patients underwent pre- and postoperative cystourethrography to evaluate features of the urethral and vesical anatomy after RARP.
No patients had baseline lower urinary tract abnormalities, such as a neurogenic bladder, bladder outlet obstruction, or overactive bladder. No patients underwent salvage radiotherapy, took medications that affect the lower urinary tract function, such as alpha blockers or antimuscarinics, or underwent bladder neck contracture or urethral stricture surgeries and injectable treatments, such as collagen, into the membranous urethra until the date of postoperative evaluation for urinary incontinence.
All patients have conducted pelvic floor exercises for acquiring the urinary continence from the preoperative period. Informed consent was obtained from all patients before the study, after explaining the purpose and methods. The study protocols were approved by the ethics committee at our institution.
Operative technique
All cases underwent surgery using the 3-arm Da Vinci Si surgical system (Intuitive Surgical, Sunnyvale, CA) with combined posterior and anterior intraperitoneal approaches and early exposure of the seminal vesicles and vasa deferentia. Neurovascular bundle preservation was performed in patients who were potent (5-item International Index of Erectile Function score ≥14) 13 and desired preservation of potency. 3
In all cases, anastomosis between the urethra and bladder started with the Rocco technique for posterior reconstruction of Denonvilliers' fascia, 7,14 followed by Van Velthoven's stitch 15 using a running, double-armed barbed 3–0 polyglyconate suture (V-LOC®; Covidien, Mansfield, MA). Integrity of the urethrovesical anastomosis was confirmed intraoperatively with intravesical instillation of 150 mL of sterile saline.
Neurovascular bundle preservation was performed using a similar manner in accordance with the four grades of posterolateral resection of the prostate: Grade 1, intrafascial dissection; Grade 2, interfascial dissection; Grade 3, extrafascial dissection (partial nerve sparing), and Grade 4, wide dissection. 16,17 However, due to the limited numbers of patients, the patients who were performed any nerve-sparing procedures, including Grade 1–3, are added in the nerve-sparing group and patients who were performed wide dissection (Grade 4) are added in the non nerve-sparing group. RARP was performed or supervised by a single surgeon (Y.K.).
Cystourethrography
Cystourethrography before RARP
The bladder was filled with 100 to 150 mL of mixture (saline 110 mL, iodinated contrast media [iopamidol, Iopamiron 300; GE Bayer, Osaka, Japan] 40 mL) through an 8F Nelaton catheter (flexible catheter). Images were obtained for anteroposterior and lateral projections with the patient standing without the Nelaton catheter withdrawal.
Cystourethrography after RARP
First, 7 days after RARP, urethrography was performed to confirm the absence of urinary leakage from the vesicourethral anastomosis as well as the urethral anatomical features before cystourethrography. Contrast media were infused through the indwelling catheter. Next, after removal of the indwelling catheter, cystourethrography was performed in a manner similar to that used before RARP.
Cystourethrography parameters assessed
Cystourethrography was reviewed by two reviewers to assess the anatomical parameters outlined in Table 1 (Fig. 1). Two board-certified radiologists (O.H. and K.K., with 17 and 6 years of experience in pelvic imaging, respectively) made all evaluations by consensus decision. These radiologists were aware that patients had prostate cancer and were undergoing RARP, but did not know any other clinical and pathological findings. The pre- and postoperative urethrocystography variables evaluated were the posterior-urethral vesical angle 18,19 and position of the urethrovesical junction. 20 The postoperative urethrography and cystourethrography valuables evaluated were postoperative membranous urethral length (MUL) 21,22 and degree of atony of the external urethral sphincter (EUS). In the pilot study, cystourethrography performed due to the catheter withdrawal demonstrated the existence or not of atony of the EUS (Fig. 2B, C). We assessed whether or not that is related to the early acquisition of urinary continence.

Representative cystourethrography imaging. Pre-
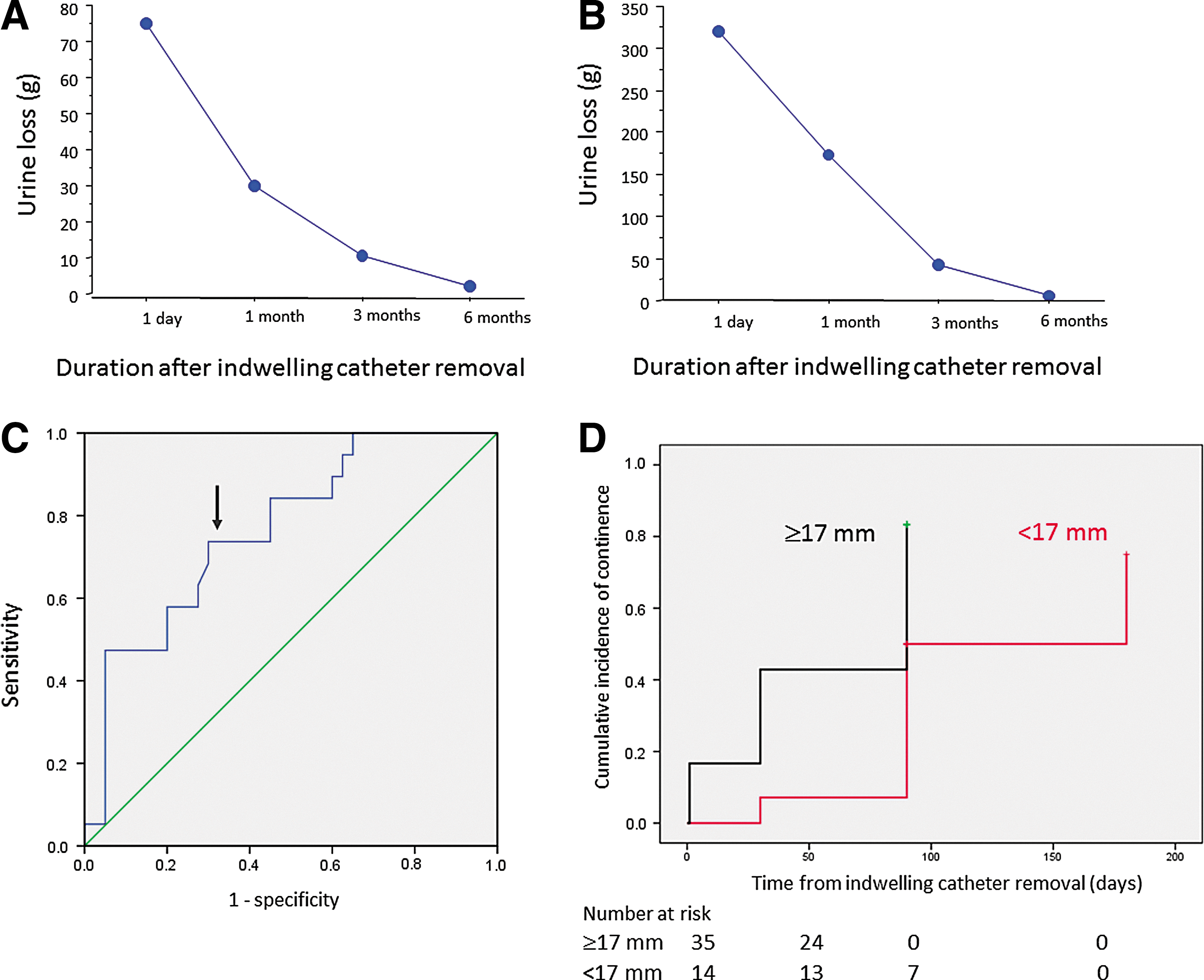
Mean urine loss in pad test, Cutoff values for membranous urethral length and cumulative incidence of urinary continence Mean urine loss in 1- and 24-hour pad tests after robot-assisted laparoscopic radical prostatectomy
EUS=external urethral sphincter; MUL=membranous urethral length; post=postoperative; pre=preoperative.
Urinary continence definition
The three methods for assessing urinary incontinence mentioned below were applied. The continence status of the patient was assessed on the day after catheter withdrawal and then at 1-, 3-, and 6-month intervals after RARP. Early acquisition of urinary continence was defined as recovery of urinary continence within 3 months after RARP. 4 The number of pad exchange is an objective measure of severity of urinary incontinence in many studies. 23 –26 On the other hand, several studies reported that pad count is a poor measure of severity of urinary incontinence. 27 –29 Thus, urinary continence was judged as present if all three of the following requirements were met. First, subjective evaluation of urinary continence was that the patient was using either no pads or only one security liner during stressful activities. 30 The second item was a 1-hour pad test. 31 This 1-hour pad test was performed according to the International Continence Society recommendations, with a bladder volume >200 mL, as evaluated by ultrasound. This bladder volume was achieved by natural diuresis following ingestion of 500 mL of water. The patient performed maneuvers and exercises during the 1-hour period while wearing a preweighed absorbent pad, which was again weighed at the completion of provocation exercises to calculate urine loss. Urinary continence on the 1-hour pad test was defined as <2 mL. 31 The third item was a 24-hour pad test. 27 Patients were reminded to use the same brand and type of pad throughout the 24-hour period. They were told to change pads as they regularly would and upon each pad change to place the used pad in a separate sealed plastic bag to minimize evaporative loss. All the patients were asked to bring all the used pads along with one unused pad on the day of the scheduled follow-up appointment, except during the hospital stay. All pads were weighed. Total urine loss was calculated by subtracting the dry pad weight from the wet pad weight, assuming that each gram of difference in weight was equivalent to 1 mL of urine loss. Urinary continence on the 24-hour pad test was defined as <8 mL. 32
Statistical analysis
All values are presented as mean±standard deviation or median. Correlations between parameters of urethral and vesical anatomical features and volume of urinary continence were investigated by simple regression analysis using the Spearman's rank correlation coefficient. Univariate logistic regression analysis was carried out to determine factors predicting the early recovery of urinary continence. Next, independent predictive factors were confirmed using multivariate logistic regression analysis. Cutoff values for independent predictive factors of urinary continence were determined using receiver operating characteristics (ROC) analysis. Time to urinary continence among two groups divided by a cutoff value was compared using log-rank statistics. Two-sided Mann–Whitney U testing was used to determine significant differences in parameters of surgical procedures using binary variables. Values of p<0.05 were considered significant. ROC analysis was undertaken using SPSS version 21 software (Statistical Package for Social Sciences, Chicago, IL). All data analyses besides ROC analysis were performed using StatView version 5.0 software (Abacus Concepts, Berkeley, CA).
Results
Baseline characteristics of patients, operative procedures, and outcomes are shown in Table 2. Mean volume of urinary incontinence from both 1- and 24-hour pad tests decreased with time (Fig. 2A, B). Association between patients' characteristics, surgical parameters, and urinary incontinence is presented in Table 3. Age was associated with 24-hour pad test results.
BMI=body–mass index; EBL=estimated blood loss; NVB=neurovascular bundle; operative duration=duration of operation, including docking/undocking the robot; SD=standard deviation.
p<0.05.
Association between urethral and vesical anatomical features and urinary incontinence
Table 4 shows correlations between the urethral and vesical anatomical features and urinary incontinence at 1 day after catheter withdrawal. Preoperative vesical and urethral anatomical features showed no significant correlations with urinary incontinence. The postoperative position of the bladder neck was significantly associated with 24-hour pad test results at 1 day after catheter withdrawal. Postoperative MUL was significantly associated with 24-hour pad test result at 1 day after catheter withdrawal. Postoperative degree of atony of the EUS was significantly associated with 1 hour pad test result at 1 day after catheter withdrawal. These three parameters that correlated significantly with urinary incontinence after catheter withdrawal were analyzed using logistic regression analysis to confirm factors contributing to early acquisition of urinary continence. Early acquisition of urinary continence was defined as present if all three of the following requirements were met within 3 months after RARP: subjective evaluation that the patient was using either no pads or only one security liner; and objective evaluations of a 1-hour pad test result less than 2 mL and a 24-hour pad test result less than 8 mL. Postoperative MUL was the only factor significantly associated with the state of continence in the early postoperative period according to both uni- and multivariate analyses (Table 5).
p<0.05.
BN=bladder neck; post=postoperative; pre=preoperative; PUVA=posterior urethrovesical angle.
Early acquisition of urinary continence was defined as present if all three of the following requirements were met within 3 months after robot-assisted laparoscopic radical prostatectomy: subjective evaluation that the patient was using either no pads or only one security liner; and objective evaluations that 1-hour pad test result was less than 2 mL; and 24-hour pad test result was less than 8 mL.
p<0.05.
CI=confidence interval; OR=odds ratio; post=postoperative.
We performed ROC analysis to elucidate the optimal cutoff value for postoperative MUL. A cutoff value of 17 mm yielded the best accuracy in ROC analysis. Area under the ROC curve, sensitivity, and specificity were 0.76, 0.76, and 0.4, respectively (Fig. 2C). Postoperative MUL >17 mm was significantly associated with early acquisition of urinary continence (Fig. 2D) (p=0.006, log-rank test).
Association between urethral and vesical anatomical features and operative procedures
Postoperative MUL was significantly associated with the nerve-sparing procedure in univariate analysis (p=0.04, Mann–Whitney U test) (Table 6). In addition, multivariate analysis was performed using multiple linear regression to investigate the contributing factors, including the nerve-sparing procedure, in relation to postoperative MUL (Table 7). The nerve-sparing procedure was the most important factor significantly associated with postoperative MUL (Table 7).
p<0.05.
post=postoperative.
p<0.05.
In the nerve-sparing group, the number of pad exchanges per day was significantly reduced at 1 month after RARP compared with the non-nerve-sparing group (nerve-sparing group, 1±1 pad/day; non-nerve-sparing, 2±3 pads/day; p=0.02, Mann–Whitney U test). Moreover, the nerve-sparing group showed a tendency toward reduced pad weight in both 1- and 24-hour pad tests compared with the non-nerve-sparing group, but differences did not reach the level of statistical significance (data not shown).
Discussion
To date, a small number of reports have demonstrated associations between imaging assessment of urethral and vesical anatomical features and urinary incontinence after radical prostatectomy. 4 –6 However, studies specific to RARP in the early postoperative period have not been reported. Nishida et al. demonstrated that urethral mobility at catheter removal predicts early recovery of urinary continence after retropubic and laparoscopic radical prostatectomy. 5 Because RARP has a tendency to allow early acquisition of urinary continence compared with retropubic and laparoscopic radical prostatectomies, data on associations between urethral and vesical anatomical features and urinary continence, particularly in RARP, are needed. Jeong et al. demonstrated in a retrospective study that the location of vesicourethral anastomosis in the pelvic cavity evaluated by postoperative cystography represents an independent predictor of early recovery of urinary continence after radical prostatectomy, which includes retropubic, laparoscopic radical prostatectomy, and RARP. 4 They showed that the higher location of vesicourethral anastomosis in the pelvic cavity achieved by preservation of surrounding structures and membranous urethra during apical dissection is associated with a higher rate of early recovery of urinary continence. In their postoperative cystography, higher location of the bladder neck indicated a longer postoperative membranous urethra. In the present study, postoperative MUL, chosen by the association between 1- and 24-hour pad test results and urethral and vesical anatomical features, was the most important factor for recovery of urinary continence in the early postoperative period after RARP. Paparel et al. demonstrated in a retrospective study that postoperative MUL, as evaluated by endorectal magnetic resonance imaging, is associated with recovery time and the level of urinary continence after retropubic and laparoscopic radical prostatectomy. 6 These observations are consistent with our prospective clinical cohort observational study, especially in RARP, in the early postoperative period to investigate the relationship between urethral and vesical anatomical features, as evaluated by pre- and postoperative urethrovesicography and urinary incontinence, as assessed by both subjective and objective data.
Several studies have demonstrated that preservation of the neurovascular bundle was significantly associated with recovery of urinary continence. 13,33 However, the reasons why preservation of the neurovascular bundle affects the recovery of urinary continence have not yet been completely elucidated. In the present study, neurovascular bundle-preservation procedures resulted in long postoperative MUL. One possible explanation for the early recovery of urinary continence with neurovascular bundle preservation is that MUL is retained after RARP. Potential reasons for the preservation of MUL using neurovascular preservation are as follows. First, defense against direct damage to the membranous urethra was achieved by retaining tissue surrounding the urethra and prostatic apex by performing neurovascular bundle preservation. Second, retention of MUL by prevention of urethral denervation was accomplished by guarding against damage to the involved nerves, such as the cavernous, 34 pelvic, and pudendal nerves. 35 During neurovascular bundle-preservation procedures, involving dissecting the neurovascular bundles laterally from the prostate, the pudendal or pelvic nerves were indirectly preserved because these ran more lateral to the neurovascular bundles. 35
In the present study, the tonicity of EUS was significantly retained in the nerve-sparing procedures. Although a functional study was not performed and multivariate analysis did not demonstrate statistical significance in the present study, nerve-sparing procedures also have a possibility of early acquisition of urinary continence by retaining the tonicity of EUS.
Several methodological limitations must be considered when interpreting the results of the present study. First, the sample size was small because the current study was performed at only a single institution. Sufficient statistical power to identify associations between morphology of the bladder and urethra and urinary continence may, thus, have been lacking. Second, although we performed cystourethrography according to the methods reported by Jeong et al., 4 a standard international protocol for the cystourethrography assessment method has yet to be defined. However, the two radiologists carried out the pre- and postoperative cystourethrography following the same protocol at our institution; thus, consistency of the methods used for cystourethrography was maintained. Third, we did not perform the urodynamic assessment; therefore, the association between morphology and the function of lower urinary tract could not be evaluated. However, the operation of the urodynamic study at the same time as catheter withdrawal might be difficult because there was a possibility of damage of the anastomotic site between the bladder and urethra. Fourth, our study might not provide any preoperative parameters of urethral and vesical anatomical features for clinicians to be able to predict early recovery of urinary incontinence before RARP, however, patients with postprostatectomy incontinence worried about how long they will have to cope with incontinence after radical prostatectomy, as the length of the period during which incontinence will continue can vary a great deal even if the skilled hands have performed RARP. 5,36 The present study demonstrated that postoperative MUL >17 mm was significantly associated with early acquisition of urinary continence. This information is a helpful guideline for patients and physician to estimate the duration of incontinence and would decrease patient emotional stress for the uncertain duration of postprostatectomy incontinence.
Conclusion
Postoperative MUL represents the most important factor for recovery of urinary continence after RARP in the early postoperative period. Postoperative MUL >17 mm could be expected to predict early recovery of urinary continence. Preservation of the neurovascular bundle might thus achieve early recovery of urinary continence by preserving the MUL.
Footnotes
Acknowledgment
The authors acknowledge that this study was previously published as the conference proceeding at the World Congress of Endourology and SWL in Taipei 2014.
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.