
Abstract
Background and Purpose:
The optimal treatment of patients with lower pole renal stones continues to be a dilemma for urologists. Retrograde intrarenal surgery (RIRS), percutaneous nephrolithotomy (PCNL), and extracorporeal shockwave lithotripsy (SWL) all constitute viable therapeutic options in selected patients. The aim of this study was to assess the efficacy and safety of RIRS, PCNL, and SWL in management of lower pole renal stones.
Methods:
A literature search was performed in July 2014 using PubMed, Embase, and Web of Science databases. Literature reviewed included meta-analysis and randomized and nonrandomized controlled studies to identify relevant studies for the meta-analysis.
Results:
Six randomized and eight nonrandomized studies were identified for analysis. PCNL provided a significantly higher stone-free rate (SFR) compared with RIRS and SWL. Furthermore, no statistical significant difference was found when PCNL was compared with RIRS and SWL for complication rate. Compared with the other two treatments, RIRS had a longer operative time and PCNL had a longer hospital stay. SWL was associated with significantly higher re-treatment rate compared with RIRS and PCNL, whereas there were no significant differences in auxiliary procedure rates among the three treatment techniques.
Conclusion:
RIRS offers a relative higher SFR while it has a longer operative time. PCNL is associated with the highest SFR at the expense of the longest hospital stay. SWL is performed as an outpatient procedure with a relative shorter operative time; however, it has lower a SFR and higher re-treatment rate. The categories of complications vary while the overall complication rates are comparable among the three treatment techniques.
Introduction
W
SWL is a low morbidity outpatient procedure that is preferred by many urologists and accepted by many patients. The 2013 European Association of Urology (EAU) guidelines recommend SWL as the first management option for lower pole renal stones smaller than 1 cm. 3 SWL, however, may be associated with poor clearance of fragments from the lower pole, because its stone-free rate (SFR) is dependent on anatomic features. 4
At present, PCNL is the standard option for the management of large stones (>2 cm) and is also preferred for the management of multiple renal stones or stones in dependent areas of the kidney, such as the lower pole, by many urologists, because of its constant high success rates independent of stone size. 5 Nevertheless, its high SFR is counterbalanced by the risk of a high morbidity rate. 6 Recently, efforts have been made to decrease the morbidity associated with PCNL. With the emergence of the minimally invasive PCNL applying miniaturized instruments and tubeless technique that reduce the invasiveness of conventional PCNL, a great decreased rate of complications has been achieved without affecting its excellent result. 7,8
A potential less invasive alternative to the percutaneous approaches is provided by flexible ureteroscopy, also referred to as RIRS, which was originally applied in the management of lower pole stones resistant to SWL. 9 RIRS is increasingly used as a primary modality to manage lower pole stones, and it may potentially achieve higher SFR than SWL with lower morbidity than PCNL for patients with low volume stone disease. The drawbacks of retrograde access, however, include the limited visualization, reduced size of fragment removal, and the requirement of stone lithotrites and baskets. 10 What is more, high cost is a major obstacle to the wide application of RIRS, especially in developing countries. 10
Regardless of their limitations, PCNL and RIRS are recommended as first-line treatments of patients with lower pole stones on the occasion that anatomic factors make SWL unfavorable in the 2013 EAU guidelines for urolithiasis. 3
We aim to perform a meta-analysis of available high-level studies to evaluate the efficacy and safety of RIRS, PCNL, and SWL in the management of lower pole renal stones. The main crucial parameters under evaluation included the efficacy of each method, as described by the SFR, the complication rate, the operative time, the hospital stay, the auxiliary procedure rate, and the recurrence rate.
Methods
Literature search and article selection
A literature search was performed on July 22, 2014, using PubMed, Embase, and Web of Science databases to identify relevant studies. The following search terms were used for the search: Retrograde intrarenal surgery/flexible ureterorenoscopy/flexible ureteroscopy/RIRS OR percutaneous nephrolithotomy/percutaneous lithotripsy/PCNL OR extracorporeal shock wave lithotripsy/SWL) AND lower/inferior AND calyceal/calices/calyx. Search restrictions were set for the English language and human species. The retrieved articles were gathered and viewed by WZ and TZ independently, and all disagreements were resolved by their consensus. Reference lists of the selected articles retrieved in the search as well as relevant review articles were also studied (Fig. 1).

PRISMA flow diagram of search strategy.
Evaluation of study quality
The levels of evidence (LE) were estimated for all included studies using the criteria provided by the Oxford Centre for Evidence Based Medicine. 11 The methodologic quality of the studies was evaluated according to the Jadad Scale for randomized controlled trials (RCTs) 12 and the Newcastle-Ottawa Scale (NOS) for nonrandomized controlled trials. 13 The assessments were processed independently by two reviewers, and the final decision was determined by a discussion between them.
Statistical analysis
After the studies were reviewed, a meta-analysis was performed to assess the efficacy and safety of RIRS, PCNL, and SWL in management of lower pole renal stones by the pairwise comparisons among the three treatment techniques. Extracted data for the analysis included SFR, postoperative complication rate, operative time, length of hospital stay, need for auxiliary procedures, and re-treatments. The odds ratio (OR) and mean difference were calculated for the binary and continuous variables, respectively. To perform a meta-analysis of continuous parameters, the mean values and standard deviations are needed to pool data. Nevertheless, sometimes, the published literature only presents continuous data as means and range. For those studies, standard deviations were calculated according to the methodology described by Hozo and associates. 14
The Q and I 2 statistics were used to evaluate the heterogeneity among studies: Homogeneity was rejected when the Q statistic P value was<0.10 or the I 2 value was >30%. Depending on whether homogeneity was accepted or rejected, we applied the fixed effect model or the random effect model to estimate the combined ORs (or weighted mean differences) and the 95% confidence intervals (CIs). The pooled effects were computed by the z test, and statistical significance was set at P<0.05. The statistical analysis was conducted using Stata v.12.0 statistical software (StataCorp, College Station, TX).
Results
Study characteristics
Fourteen studies have been finally included for the analysis, composed of 6 RCTs 15 –20 (LE: 2b) including four multi-institutional trials and 8 retrospective case control studies 21 –28 (LE: 3b) (Table 1). The methodologic quality of included studies was relatively high for three of the nonrandomized studies (NOS: 7 of 9 points and 6 of 9 points) and medium for five (NOS: 5 of 9 points and 4 of 9 points), whereas the five RCTs were medium quality (Jadad Scale: 3 of 5 points) and relatively low for only one (Jadad Scale: 2 of 5 points), which was mainly attributed to the no blind methods.
Using Newcastle-Ottawa scale (score from 0 to 9)
Jadad scale (score from 0 to 5)
LE=level of evidence; RIRS=retrograde intrarenal surgery; PCNL=percutaneous nephrolithotomy; SWL=extracorporeal shockwave lithotripsy; RCT=randomized controlled trial.
A total of 328 RIRS cases (15.3%), 476 PCNL cases (22.2%), and 1338 SWL cases (62.5%) were compared in our meta-analysis. There were two studies comparing all three treatment techniques, 21,22 whereas there were two comparing RIRS and PCNL, 23,24 five comparing RIRS and SWL 15 –17,25,26 ; the remaining five compared PCNL and SWL 18 –20,27,28 In addition, only two studies mentioned their portion of patients with multiple stones. 23,24 Still and all, the preoperative demographic characteristics such as mean age (45.9 vs 44.1 vs 46.7 y), sex ratio (male/female: 1.5 vs 1.6 vs 1.4), stone locatiozn (left/right: 1.0 vs 1.1 vs 1.3), and stone size (1.2 vs 1.6 vs 1.4 cm) were comparable among RIRS, PCNL, and SWL study populations (Table 2).
cm2; all other units are in centimeters.
Meta-analysis outcomes
SFR and complication rate
PCNL provided a significantly higher SFR compared with RIRS (OR, 0.41; 95% CI, 0.21–0.82; P=0.012) and SWL (OR, 8.75; 95% CI, 3.29–23.26; P<0.001), whereas no statistical significant difference of SFR was found between RIRS and SWL (OR, 1.97; 95% CI, 0.98–3.95; P=0.057) (Fig. 2). In terms of complication rate, there was no significant difference between PCNL and RIRS (OR, 0.81; 95% CI, 0.42–1.57; P=0.541), PCNL and SWL (OR, 3; 95% CI, 0.92–9.74; P=0.068), RIRS and SWL (OR, 0.99; 95% CI, 0.61–1.62; P=0.974) (Fig. 3).

Forest plot comparing stone-free rates between
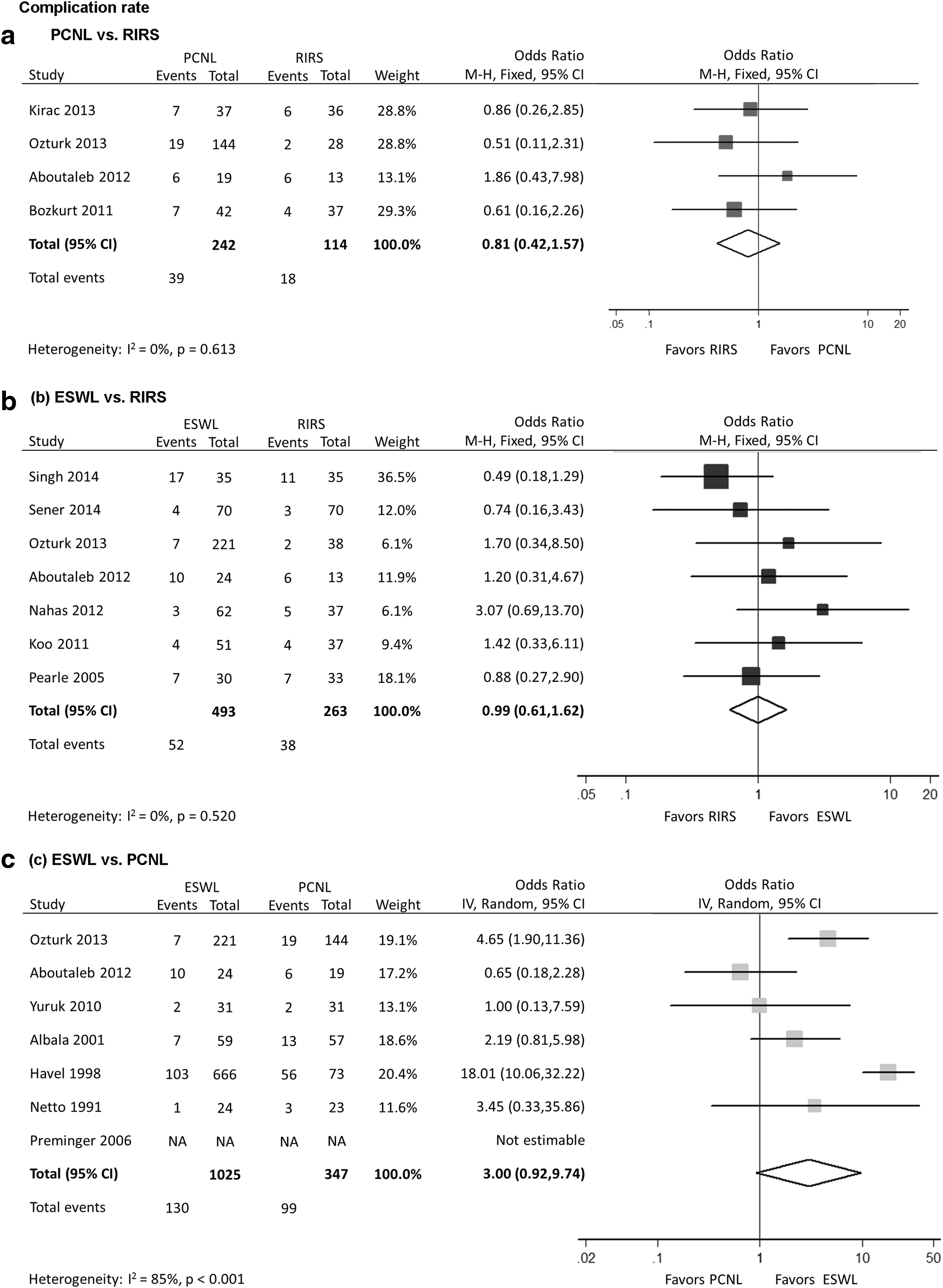
Forest plot comparing complication rates between
Operative time and hospital stay
PCNL had significantly shorter operative time than RIRS (weighted mean difference [WMD], 15.56; 95% CI, 10.04–21.08; P<0.001); however, no statistically significant difference was found when SWL was compared with PCNL (WMD, 14.70; 95% CI, −1.16–30.56; P=0.069) and RIRS (WMD, 20.77; 95% CI, −0.29–41.83; P=0.053) for operative time (Fig. 4). Compared with the other two treatment techniques, PCNL led to a longer hospital stay than RIRS (WMD, −0.85; 95% CI, −1.03– −0.67; P<0.001) and SWL (WMD, 2.63; 95% CI, 0.62–4.65; P=0.010). Furthermore, RIRS patients also had a longer hospital stay compared with SWL patients (WMD, 1.24; 95% CI, 0.68–1.80; P<0.001) (Fig. 5).
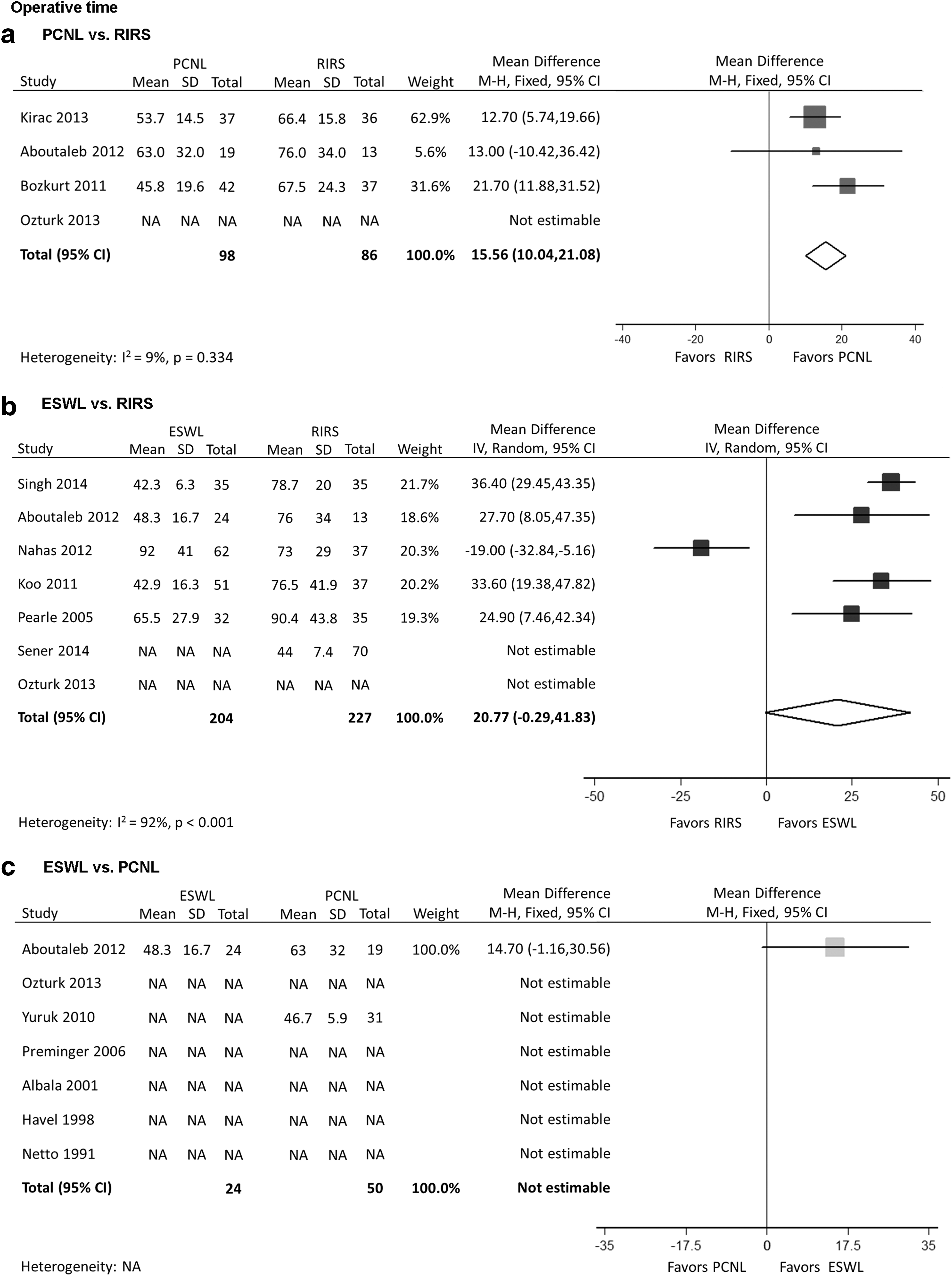
Forest plot comparing operative time between
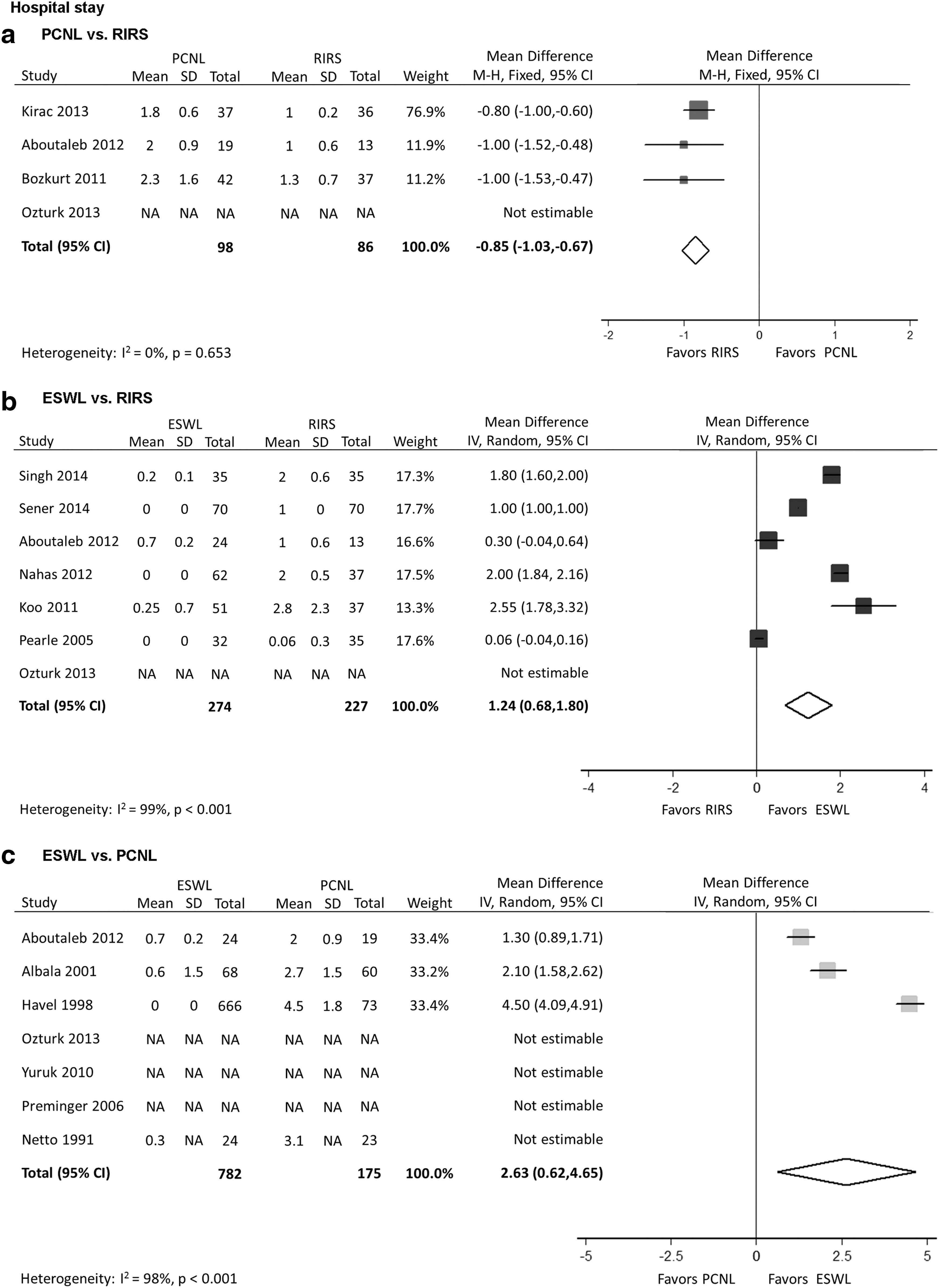
Forest plot comparing hospital stay between
Auxiliary procedure and re-treatment rate
There was no difference in the rate of auxiliary procedures between SWL and PCNL (OR, 0.43; 95% CI, 0.01–14.54; P=0.637), SWL and RIRS (OR, 0.43; 95% CI, 0.08–2.34; P=0.327), PCNL and RIRS (OR, 0.81; 95% CI, 0.18–3.73; P=0.785) (Fig. 6). Nevertheless, SWL was associated with a significantly higher re-treatment rate compared with RIRS (OR, 0.15; 95% CI, 0.03–0.67; P=0.013) and PCNL (OR, 0.12; 95% CI, 0.02–0.61; P=0.011) while the re-treatment rates of RIRS and PCNL did not show a statistically significant difference (OR, 3.49; 95% CI, 0.14–88.40; P=0.448) (Fig. 7).
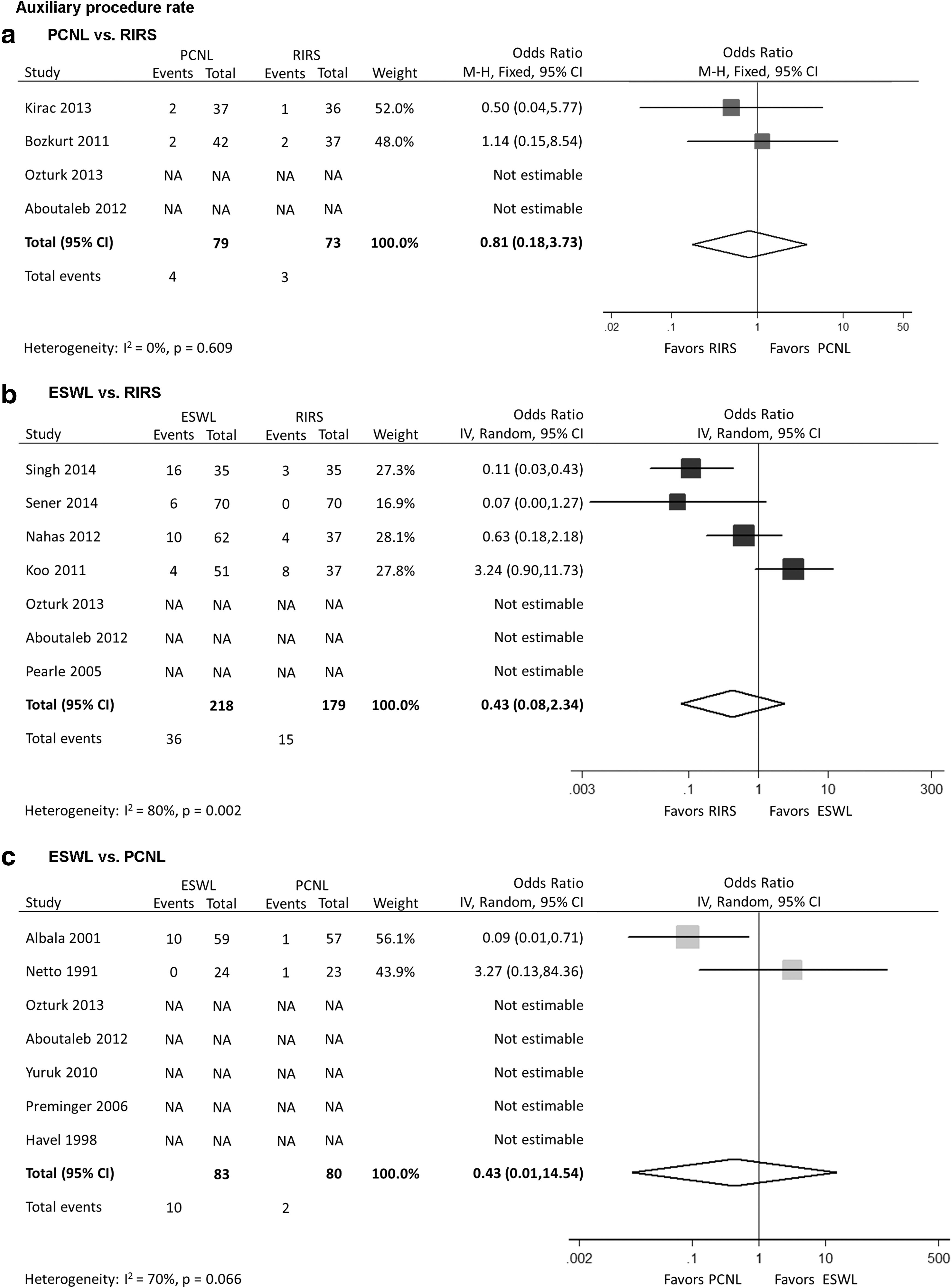
Forest plot comparing auxiliary procedure rate between
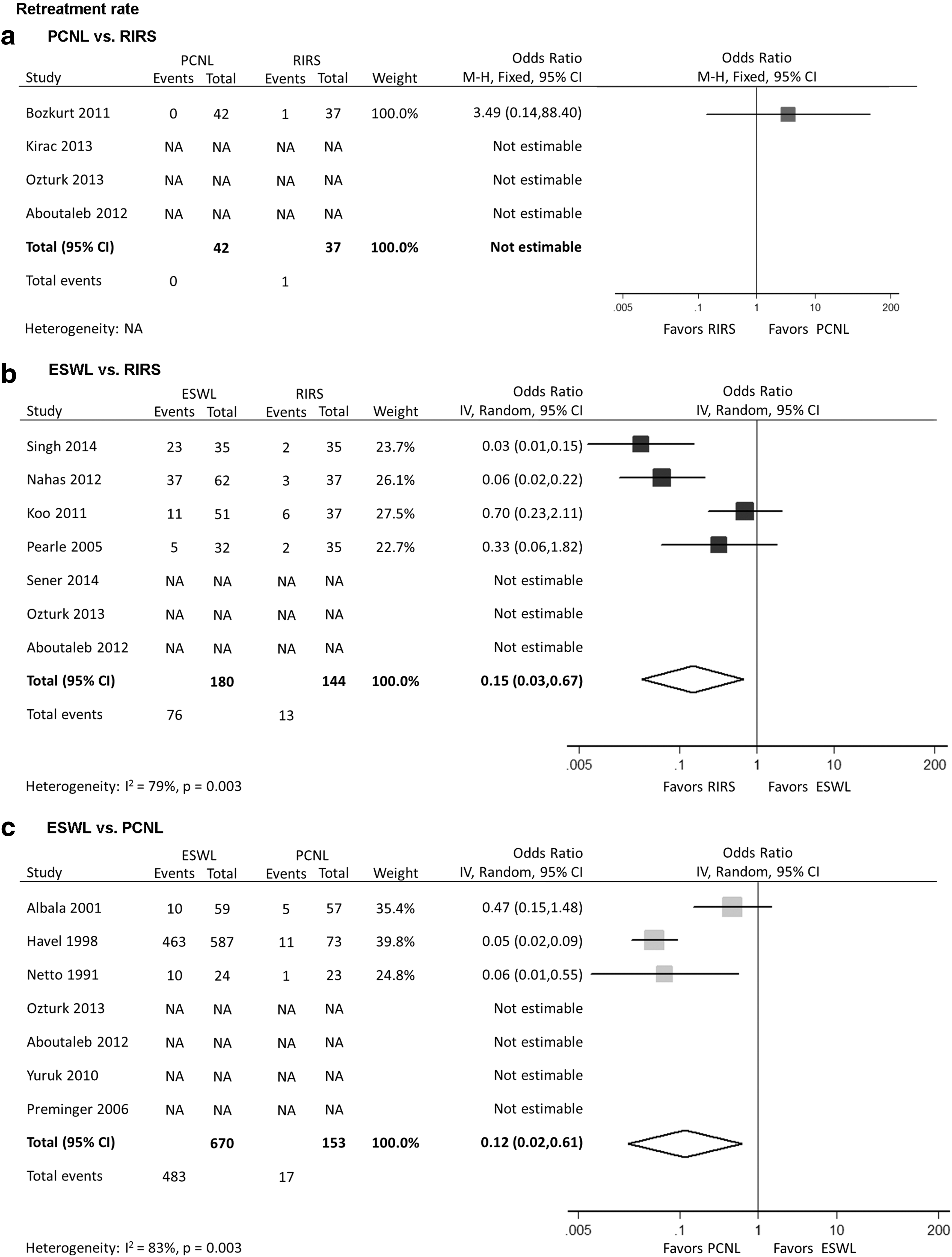
Forest plot comparing re-treatment rate between
SFR changing with time
Figure 8 shows the results of the SFR meta-analysis with time among PCNL, RIRS, and SWL. On postoperative several days, the SFRs for patients treated with PCNL and RIRS (80% vs 85%) were similar, whereas the data for SWL were not available. Furthermore, SFRs of both PCNL and RIRS had improved over weeks and that of PCNL increased significantly to nearly 95%. The SFR of SWL with time, however, did not show significant changes and was always fluctuating around 65%.

Meta-analysis of stone-free rate among PCNL, RIRS, and SWL at all time points.
Detailed complication categories
As a subjective parameter, pain (PCNL: 0%–53.4%; RIRS: 0%–18.2%; SWL: 0.9%–37.5%) was the most common and varied. Infection-related complications including fever (PCNL: 2.1%–30.0%; RIRS: 0%–10.8%; SWL: 0%–1.6%), urinary infection (PCNL: 0%–11.0%; RIRS: 0%–8.3%; SWL: 0%–1.7%), and sepsis (PCNL: 1.8–4.1%; RIRS: 2.9–8.1%; SWL: 0%–5.7%) could be seen in all three techniques, but were not included in every study.
For complications of hematuria (PCNL: 0%–21.1%; RIRS: 0%–30.8%; SWL: 1.8%–11.4%), the average reported cases were relatively less. Except for the study of Albala and colleagues, 20 which described two in the PCNL group, all the other cases of perirenal hematoma (PCNL: 0%–3.5%; RIRS: 0%; SWL: 0.9%–3.2%) happened after receiving SWL. Likewise, only one patient had steinstrasse (PCNL: 0%; RIRS: 0%–2.6%; SWL: 0%–5.7%) after RIRS in the study by Ozturk and coworkers, 21 and the remaining cases were all in the SWL group.
In addition, obstruction (PCNL: 0%–1.8%; RIRS: 0%; SWL: 0%–4.2%) just occurred in the PCNL and SWL groups. Based on all included studies, only a few patients after PCNL needed blood transfusion (PCNL: 2.7%–7.6%; RIRS: 0%; SWL: 0%). Perforation (PCNL: 0%; RIRS: 2.7%–6.1%; SWL: 0%) was unique to RIRS because it was a retrograde surgical procedure. Other reported complications included ileus, arteriovenous fistula, lumber ecchymosis, and prolonged urine discharge (Table 3).
Discussion
SFR represents a key parameter when evaluating the efficacy of a stone surgical procedure. 10 Our analysis illustrated that PCNL provided a significantly higher SFR compared with RIRS (OR, 0.41; 95% CI, 0.21–0.82; P<0.012) and SWL (OR, 8.75; 95% CI, 3.29–23.26; P<0.001). The lower pole is the ideal indication for PCNL, because percutaneous access can be achieved directly in line with the stone burden, guaranteeing the removal of stone fragments. Nevertheless, the retrograde approach has to face the technical challenge of performing extensive lithotripsies at maximal ureteroscopic deflection. 5
In the initial RCT report of the Lower Pole Study Group, 20 PCNL was associated with superior SFR compared with SWL (95% vs 37%) at a 3-month follow-up. Furthermore, when stratified by stone size, the SFR for stones <1, 1 to 2, and 2 to 3 cm was 100%, 93%, and 86%, respectively. By contrast, SFRs of 63%, 21% and 14% were reported after SWL for stones <1, 1–2, and 2–3 cm. This study revealed that the treatment efficacy for PCNL was significantly better than SWL for all stone sizes. In the following prospective study by the same group, patients with stones 1 to 2.5 cm were randomized to PCNL or RIRS. 29 The primary outcome measure was SFR that strongly favored PCNL over RIRS (71% vs 37%). Both randomized trials, however, reported a longer hospital stay and higher complication rates for PCNL compared with either RIRS or SWL, because of the greater invasiveness of the PCNL technique. 20,29
The identical conclusion was confirmed by the study of Preminger, 19 who also compared PCNL and SWL for lower pole stones. He demonstrated that for stones <1 cm, PCNL provided a 100% SFR compared with 67% for SWL. The disparity was even more apparent for stones 1 to 2 cm, for which the SFR of PCNL was 92%, whereas only 21% of cases in the SWL group reached the stone-free status. It was also claimed that RIRS was a feasible alternative to PCNL and SWL approaches, especially for patients with high surgical risks or challenges, such as bleeding diatheses, renal anomalies, solitary kidneys, and morbid obesity.
Certainly, SWL is a first-line option for the management of intrarenal stones <1 cm, and many patients will opt for this treatment technique in that it does offer several potential advantages over RIRS. After comparing 37 RIRS cases and 51 SWL cases for lower pole stones <2 cm with a mean stone size of <1 cm, Koo and associates 26 found SWL to be more efficacious and cost-effective than RIRS. In a RCT study, Pearle and colleagues 17 compared RIRS with SWL for the management of small size (<1 cm) lower pole stones and found no statistically significant difference of SFRs between RIRS (50%) and SWL group (35%), but patients had greater acceptance and higher satisfaction of SWL. This is likely the result of shorter recovery time and minimal anesthesia during the procedure.
For medium size stones, however, there is a decline in the use of SWL with a parallel rising application of RIRS because it is associated with better SFR. 30 A study with lower pole stones 1 to 2 cm was conducted by El-Nahas and coworkers. 25 They obtained a significantly higher SFR in RIRS (86.5%) compared with SWL (67.7%), whereas the complication rates were 13.5% for RIRS and 4.8% for the SWL group. Furthermore, the study by Sener and associates 16 reported an even higher SFR and lower complication rate for the RIRS group, which may be because of the different stone sizes and consideration of a lower pole infundibulopelvic angle.
In a recent study by Bozkurt and colleagues, 24 they showed similar SFRs of RIRS and PCNL (89.2% vs 92.8%) for lower pole stones 1.5 to 2 cm. As for complications, there were minimal differences in both procedures except for three cases of hemorrhage (necessitated transfusion) in the PCNL group. They finally concluded that RIRS had acceptable efficacy for medium size stones in the lower pole with lower morbidity.
An important technique in managing lower pole stones by RIRS is displacement of the stones to a midpolar area or upper pole to facilitate stone removal. It appeared that the SFR could be greater with displacement methods than with in situ attempts to fragment the stones. 31 Portis and coworkers, 32 however, noted a SFR of only 59% after RIRS despite displacing all lower pole stones to an upper pole and manually retrieving fragments. These data suggest that the SFR relying on gravity clearance or manual retrieval of fragments will always be inferior to percutaneous stone removal.
Even so, gravity still plays a major role in clearing stone fragments. Thus, patients with lower pole stones have residual fragments significantly more often than those with stones in other positions. 33,34 Recently, with an increased reliance on laser dusting without stone extraction in mini-PCNL and RIRS procedures, challenges to fragment clearance are similar to those faced in SWL, such as infundibulopelvic angle, infundibular width and length, and urine output. Accordingly, SFRs would improve over weeks as fragments are cleared with the urine flow, 10 which was partially proved by our results of the SFR meta-analysis with time.
Although the overall complication rates were not significantly different comparing PCNL with RIRS, the greater invasiveness of the procedure leads to a more frequent use of transfusions in patients undergoing PCNL; in our meta-analysis, blood transfusion was unique to PCNL. After reviewing 5750 patients undergoing PCNL over 6 years, the UK Health Episode Statistics database identified complication rates for hemorrhage (1.4%), fever (1.7%), urinary tract infection (3.8%), and sepsis (0.7%), and concluded that hemorrhage and infection represented relatively common and potentially severe complications of PCNL. 35 Because PCNL and RIRS techniques share overlapping indications, the potential serious morbidity of PCNL needs to be considered when comparing it with less invasive RIRS.
Although the threshold of stone size >2 cm is a commonly cited standard for choosing PCNL over RIRS, technology and technique advancements have dramatically increased the therapeutic potential of RIRS. Recent studies have reported that RIRS can offer an acceptable efficacy with low morbidity in selected patients with large intrarenal stones. 36,37 Retrograde endoscopic management of lower pole stones, however, can be technically demanding and may cause unexpected complications, particularly for urologists who infrequently perform flexible ureteroscopy. As one of the most serious complications, ureteral perforation was unique to RIRS in our meta-analysis. On the other hand, with the development of the miniature nephroscope and miniperc technique, PCNL has been innovatively used for midsized lower pole stones, 23 diverging from the EAU recommendation for PCNL to be used in stones >2 cm.
Our analysis showed that although SWL carries a relatively lower complication rate compared with PCNL, the total complication rates of SWL and RIRS were almost identical, which meant that SWL was not the so-called noninvasive procedure. D'Addessi and coworkers 38 implied that SWL was a serious procedure and its complications should be considered before being applied on patients. Complications of SWL were mainly connected to the stone passage, infections, and renal or adjacent tissue injury. The study of Bierkens and colleagues 39 indicated that steinstrasse might occur at a 40% rate if a Double-J stent was not placed after SWL for stones >2 cm. Hemorrhage caused by direct tissue damage of SWL might be perirenal, intrarenal, or subcapsular, and it developed for an overall incidence of 4.1% if the asymptomatic hematomas were counted in. 40 In addition to those mentioned, more serious complications such as ruptured spleen and acute pancreatitis have been reported. 41,42
Operative time was found to be significantly shorter for PCNL compared with RIRS. Among the included studies, two favored PCNL, 23,24 whereas one did not show significant difference. 22 This difference may translate into potential significant clinical benefit to patients in that the longer duration of the ureteroscopic procedure was strongly related to postoperative complications, especially ureteral perforation. 43 Therefore, it is necessary to strictly limit the operative time of RIRS. In addition, operative time is absolutely associated with nuances in the surgical techniques, and many technical differences deserve to be noted in this regard. 10
Although practices for hospital admission vary globally, patients are routinely admitted after PCNL, whereas patients undergoing RIRS can be discharged the same day. Furthermore, just like SWL, RIRS is increasingly performed as an outpatient procedure in many countries. So that, not surprisingly, RIRS showed a significantly shorter length of hospital stay than PCNL in our analysis, which could be regarded as an important feature in terms of cost reduction. Recently, de la Rosette and associates 6 have demonstrated that the Clavien score was strongly associated with duration of hospital stay. The study of Ozturk and colleagues 21 showed that grades II and III complications were more common in the PCNL group, while grade I accounted for the most complications in RIRS group. This may explain why length of hospital stay was shorter for RIRS, even though the overall complication rates did not show significant disparity between RIRS and PCNL.
There was no difference in the rate of auxiliary procedures among the three treatment techniques, but SWL was associated with a significantly higher re-treatment rate compared with RIRS and PCNL in our meta-analysis. In the study of Aboutaleb and coworkers, 22 SWL failed in more than one-third (37.5%) of the patients, and they had the possibility of repeating the session or shifting to PCNL or RIRS for removal of the significant fragments, resulting in more sessions and follow-up visits. Even if SWL has advantages of minimal invasiveness, outpatient mode, and better subjective acceptance, its high re-treatment rate is still a problem that has long bedeviled urologists and urged wide concerns.
Our meta-analysis was conducted using the currently available comparative studies. More than half of the studies, however, were nonrandomized retrospective comparisons, and only six RCTs were available for inclusion. Among all the included RCTs, five studies described their methods of randomization in detail while one did not. Unavoidably, patients and investigators could not be blinded to the interventions, and blinding of the outcome and data assessors was also not described in these studies. Furthermore, some articles reported missing patients during the follow-up, but the reasons were not described clearly.
Heterogeneity among studies was found to be high for several parameters, and the reasons causing it could be complex. The sources of heterogeneity could be explained by the difference in patient inclusion criteria, surgical practices, outcome definitions and standards, or follow-up imaging and duration. To illustrate the difference in SFRs and complication rates among the three techniques more accurately, we further displayed the results of the SFR meta-analysis with time and made a summary of the detailed complications among RIRS, PCNL, and SWL in the literature.
Although the above limitations might influence the interpretation of our findings, as the first meta-analysis that typically focused on the management of lower pole renal stones and included RIRS, PCNL, and SWL simultaneously, our study provided the most up-to-date information in this area.
Conclusion
Meta-analysis of available comparative studies suggests that RIRS offers a relatively higher SFR while it has a longer operative time. PCNL is associated with the highest SFR at the expense of the longest hospital stay. SWL is mostly performed as an outpatient procedure with a relatively shorter operative time; however, it is associated with a lower SFR and higher re-treatment rate. The categories of complications vary while the overall complication rates are comparable among the three treatment techniques, and most of them are minor complications that can be managed conservatively.
The aim of lower pole stone management is to achieve maximal stone clearance with minimal morbidity. No single technique is suitable for the removal of all lower pole stones. Urologists need to address lower pole stones individually, and all pros and cons should be considered when determining the optimal treatment technique for lower pole renal stones.
Footnotes
Acknowledgments
We thank Dr. Huijun Li for his valuable proposals to our manuscript. The study received funding from the 1255 Fund (CH125520302) of Changhai Hospital, Second Military Medical University, Shanghai, China. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.