
Abstract
Purpose:
To compare the clinical efficacy and safety of selective vs hilar clamping during minimally invasive partial nephrectomy (PN).
Methods:
Studies comparing the effect and safety of selective versus hilar clamping during PN were identified by a systematic search using MEDLINE and EMBASE from January 2000 to November 2014. Quality of the selected studies was assessed according to the Newcastle-Ottawa Scale (NOS).
Results:
A total of seven retrospective studies were included. No significant differences were observed between the two groups in age, body mass index, tumor size, pre-estimated glomerular filtration rate (eGFR), operative time, and length of stay. The selective clamping group had greater estimated blood loss (P<0.01) but similar blood transfusion rate (P=0.78) compared with the hilar clamping group. There were no significant differences between the two groups in terms of urinary leaks, overall complication rate, and positive margin rate. Patients who underwent selective clamping had a lower change in eGFR (mean difference [MD]: 13.95; 95% CI 8.85 to 19.05; P<0.01) and a lower percent change in eGFR (MD: 18.51; 95% CI 14.18 to 22.84; P<0.01) at 1 week. Combined results from two studies showed a trend toward a lower percent change in eGFR at 3 months (MD: 5.47; 95% CI −0.28 to 11.22; P=0.06). At 6 months, two studies showed no significant differences in percent change of renal function between the two groups (MD: 16.85; 95% CI −10.47 to 44.16; P=0.23).
Conclusions:
Although selective clamping resulted in greater estimated blood loss, it provided comparable perioperative safety and superior short-term renal function preservation. The advantage of selective clamping in preservation of intermediate-term renal function remains to be evaluated in the future, however. There is a need for properly designed studies to confirm our founding.
Introduction
P
Generally, blood flow control is often necessary to provide relatively bloodless visualization for tumor excision and renal reconstruction during traditional PN. Main renal artery clamping may lead to a decline of renal function, however. 6,7 For these reasons, ongoing efforts have been made to minimize the WIT during minimally invasive PN. 6 Among them, nonclamping was proposed as an alternative to hilar clamping in terms of a lower percent change in the nadir estimated glomerular filtration rate (eGFR) whereas it carried a similar percent change in eGFR to hilar clamping at 1 year. 8 Furthermore, concerns were raised about intraoperative bleeding and higher transfusion rate. 9 To solve these problems, some researchers have focused on the development of selective renal ischemia.
Nohara and associates 10 first introduced a method called “modified anatrophic partial nephrectomy” for open PN in which only the segmental artery feeding the renal tumor was clamped. Later, Gill and colleagues 11 described a new technique of “zero ischemia” in which only peritumoral blood flow is eliminated by anatomic vascular microdissection and tumor-specific devascularization during PN. Recently, selective arterial clamping with fluorescence imaging was found to preserve renal function after robot-assisted PN (RAPN). 12
Although some studies showed that selective artery clamping PN provided comparable perioperative outcomes and the advantage of significantly superior short-term renal function compared with hilar clamping PN, the true benefit of the selective artery clamping technique remains debatable. 12 –18 Moreover, one of the concerns is whether it increases the risk of greater blood loss because of the uninterrupted main renal artery. Consequently, we performed a systematic review and meta-analysis of the available literature to compare the safety and efficacy of selective artery versus hilar clamping during PN.
Methods
Study identification
We performed this meta-analysis by following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. First, we searched MEDLINE and EMBASE for data published from January 2000 to November 2014. The key words of the search strategy include “nephrectomy,” “clamp,” and “selective” (and multiple synonyms for each term). Two authors (LZ, XW) independently screened all citations and abstracts to determine potentially eligible studies. Abstracts presented but not published were included if useful information could be extracted. English language restriction was applied.
Inclusion/exclusion criteria
Studies comparing selective artery clamping with hilar clamping during minimally invasive PN were included. Eligible trials that measured operative time, estimated blood loss, length of stay, transfusion rate, complication, positive margin rate, and reduction of eGFR were used for quantitative analysis. Data on perioperative variables, complications, or renal function should be available in selected articles. Only studies on humans were included. Studies were excluded based on any of the following criteria: (1) review, letter, and case report; (2) descriptive study without comparison; (3) insufficient original data. If two studies were published by the same group with overlapping patient populations, we chose the most recent one. Disagreements on study eligibility were resolved by consensus.
Data extraction and outcome measures
The following information was extracted from each study: First author, year of publication, number of patients, means of group allocation, selective clamp technique, surgical approach, age, body mass index (BMI), tumor size, preoperative eGFR, estimated blood loss, operative time, length of hospital stay, overall complications, transfusion rate, positive surgical margins, and renal function outcomes. The primary outcome measures were operative time, estimated blood loss, length of stay, transfusion, complication, and change or percent change of eGFR. The change or percent change of eGFR was analyzed at 1 week, 3 months, and 6 months, respectively. Heterogeneity of outcomes was assessed to confirm the appropriateness of combining individual studies.
Methodologic quality
Methodologic quality of included studies was evaluated by two reviewers. The Newcastle-Ottawa Scale (NOS) was used to evaluate methodologic quality of retrospective observational studies. 19 NOS scores of ≥6 were assigned as high-quality studies.
Data synthesis and analysis
A meta-analysis comparing selective versus hilar clamping during PN was undertaken. Weighted mean difference was used for continuous variables and the risk ratio (RR) for binary outcomes. RR >1 indicates greater risk in the selective clamp group, and RR <1 indicates greater risk in the hilar clamp group. Mean difference (MD) was calculated as selective clamp minus hilar clamp. The I2 was used to quantify statistical heterogeneity. Heterogeneity was defined as P<0.10 or I2>50%; then a random effects model was used. Otherwise, a fixed effects model was applied. If continuous variables were stated as medians and range, we calculated the mean and standard deviation with the methods described by Hozo and associates. 20 Meta-analysis was performed with the Review manager 5.0 (The Cochrane Collaboration, Oxford, UK).
Results
Study selection
Figure 1 showed the process of study selection. A total of 206 reports were identified from the database searching, and relevant references and 95 articles were excluded due to duplication. After carefully reviewing the titles and abstracts, 12 relevant articles were identified. Two independent investigators reviewed the studies and determined whether they met the eligible criteria for inclusion. Then five articles were excluded based on the full text. As a result, a total of seven studies including 541 patients were identified for quantitative analysis. 12 –18
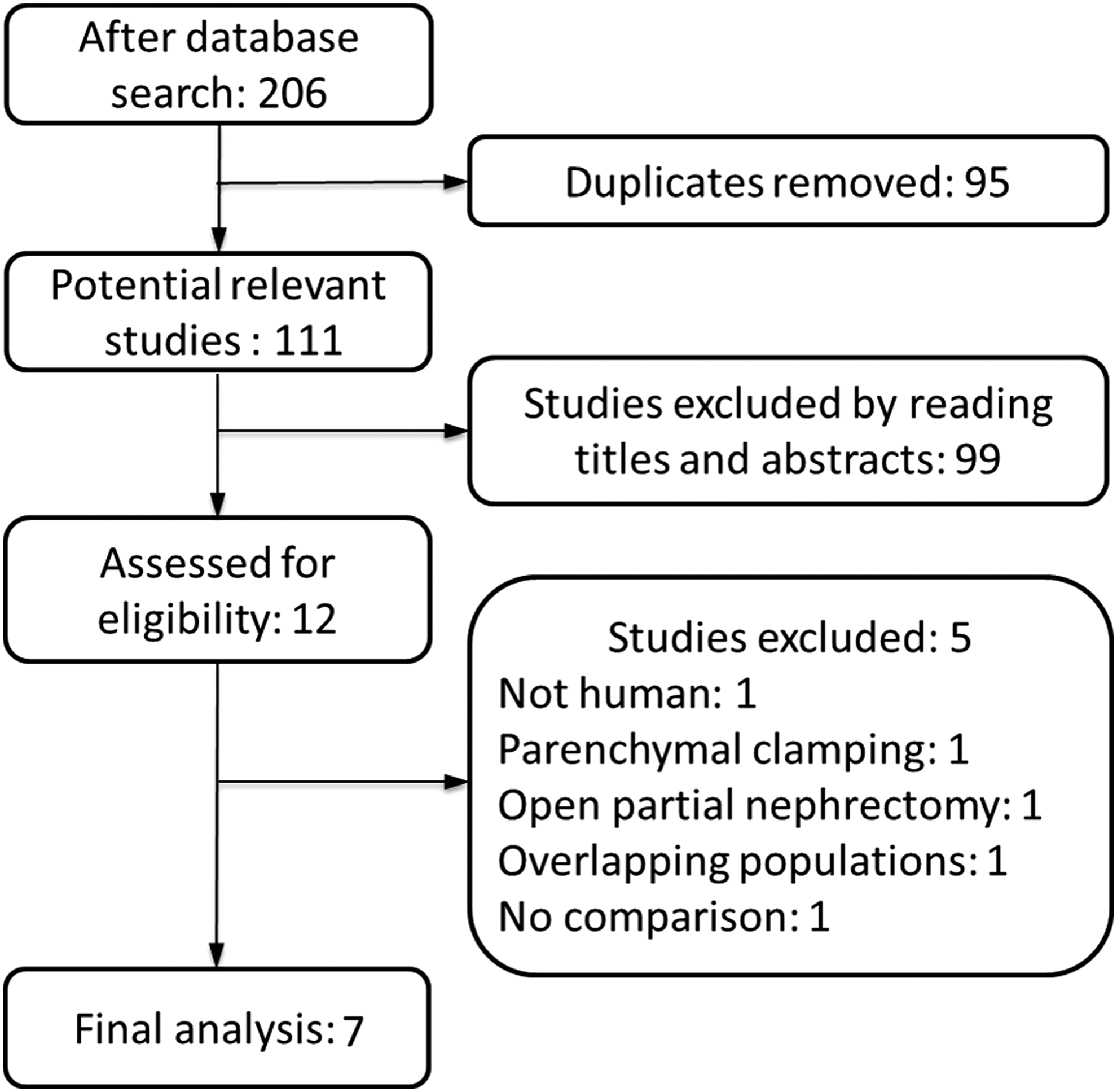
Flowchart of study selection for the meta-analysis.
Study characteristics
The characteristics of the included studies are shown in Table 1. All studies were retrospective cohort studies with no randomization. Among these studies, three studies compared functional outcomes after PN with selective artery clamping guided by near-infrared fluorescence (NIRF) imaging to a matched cohort of patients who underwent PN with hilar clamping. 12,13,15 Four other studies evaluated the clinical efficacy and safety of selective artery clamping without NIRF imaging in comparison with hilar clamping. 14,16 –18 As for surgical approaches, five studies were on RAPN. 12 –16 One study was on laparoscopy-assisted PN (LAPN). 18 One study was on LAPN or RAPN. 17 The NOS scores of all studies were more than 6.
NOS=Newcastle-Ottawa Scale for methodological quality of the included studies; NIRF=near-infraredfluorescence; eGFR=estimated glomerular filtration rate.
Preoperative variables
Supplementary Figure 1 (supplementary data are available online at
WMD/OR=weighted mean difference/odds ratio; CI=confidence interval; BMI=body mass index; EBL=estimated blood loss; LOS=length of stay.
Peri- and postoperative variables
In terms of peri- and postoperative variables (Fig. 2), there were no differences between the two groups in operative time (MD: −1.51; 95% CI −25.17 to 22.14; P=0.90) and length of stay (MD: −0.22; 95% CI −1.13 to 0.69; P=0.63). The selective clamping group had significantly greater estimated blood loss (MD: 55.16; 95% CI −20.71 to 89.61; P<0.01), however.

Forest plot of peri- and postoperative variables: (
Surgical complications and oncologic variables
As Figure 3 showed, there were no significant differences between the two groups in transfusion rate (RR: 0.77; 95% CI 0.12 to 4.78; P=0.78), urinary leak (RR: 2.48; 95% CI 0.64 to 9.70; P=0.19) as well as overall complication rate (RR: 1.11; 95% CI 0.65 to 1.90; P=0.71). Five studies described the complications in detail. Only one patient with acute renal failure was reported in the hilar clamping group. No open conversion was reported in either group. Negative surgical margins were obtained for all cases in five studies. The pool analysis of two other studies showed that there was no significant difference in the incidence of positive surgical margins in two groups (RR: 1.33; 95% CI 0.30 to 5.83; P=0.71) (Fig. 3D).

Forest plot of surgical complications and oncologic variables: (
Renal outcome
In terms of renal outcomes, compared with the hilar clamping group, the selective clamping group was associated with superior kidney function at 1 week, as shown through absolute change in eGFR (MD: 11.34; 95% CI 5.58 to 17.11; P<0.01) and percent change in eGFR (MD: 18.51; 95% CI 14.18 to 22.84; P<0.01) (Fig. 4). At 3 months, the difference in percent change of eGFR between the two groups persisted, but there was no statistical significance (MD: 5.47; 95% CI −0.28 to 11.22; P=0.06) (Fig. 5A). A similar result was obtained through the analysis of change in eGFR. At 6 months, no significant difference was observed in renal function between the two groups (change: MD: 0.20; 95% CI −8.26 to 8.66; P=0.96; percent change: MD: 16.85; 95% CI −10.47 to 44.16; P=0.23) (Fig. 5B).

Forest plot of renal outcomes in 1 week postoperatively.
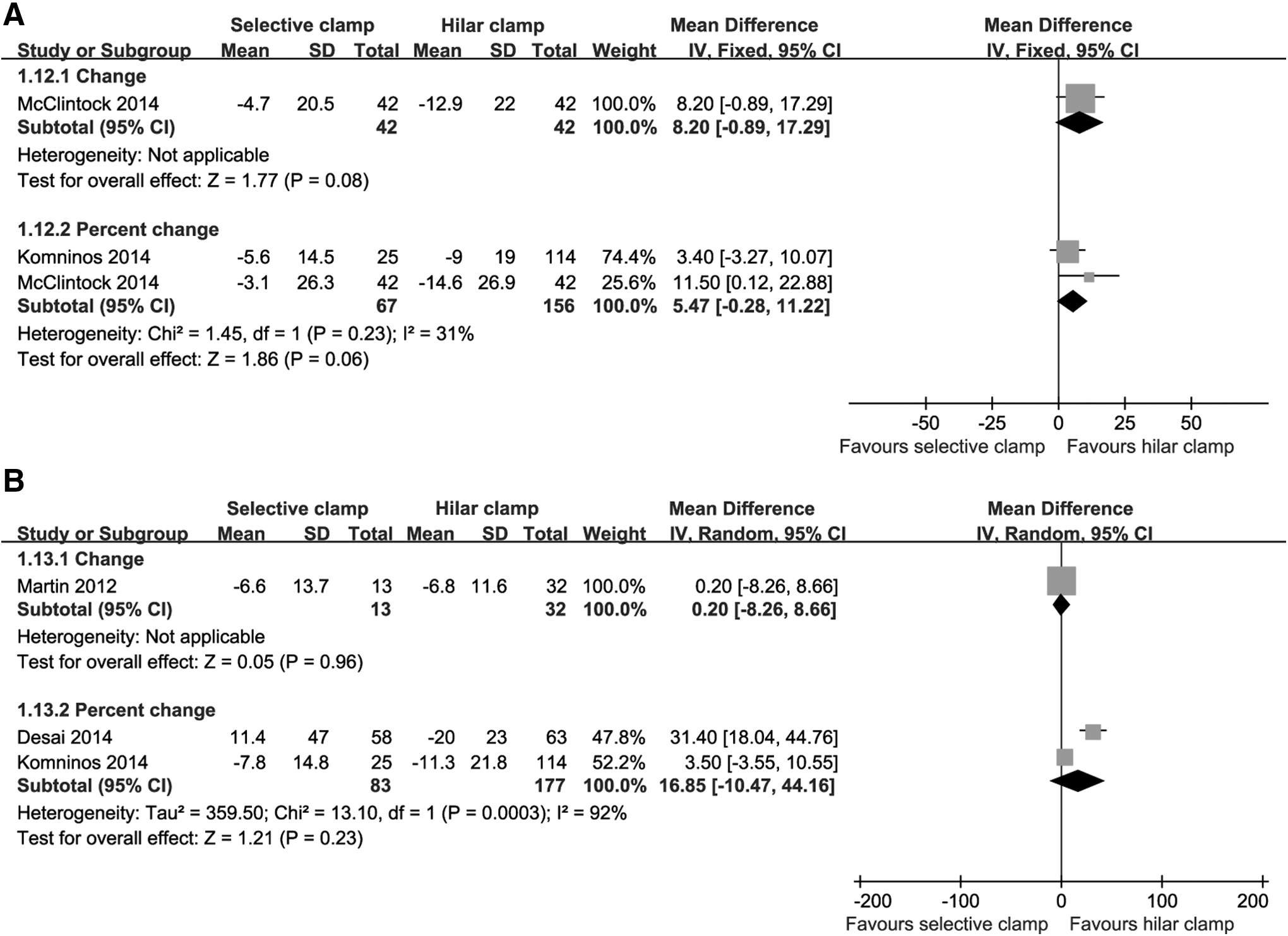
Forest plot of renal outcomes at 3-month (
Discussion
Accumulating evidence supports that WIT is a factor influencing postoperative renal function during PN with hilar clamping. 21 Then, various techniques and approaches aimed at minimizing the extent and duration of WIT were developed. Among them, a regional ischemia technique was regarded as a research “hot.” Renal vascular segmentation creates a theoretical condition for regional ischemia so that selective artery clamping could be adopted to achieve regional ischemia. 22,23 Although recent studies demonstrated the advantage of selective artery clamping over hilar clamping in preserving short-term renal function, there is controversy regarding the clinical efficacy and safety of this technique.
We included seven articles and 541 patients to address this problem. To our knowledge, there has been no systematic review or meta-analysis to date that aims to evaluate the potential benefit of selective artery clamping over hilar clamping for minimally invasive PN. Our results suggested that selective clamping had greater estimated blood loss and less change in short-term renal function when compared with hilar clamping. No significant differences in other outcomes were found between the two groups. In terms of baseline variables, the two groups were relatively comparable in age, BMI, tumor size, and baseline renal function.
One of the potential disadvantages is the risk of an increase in blood loss and transfusion rate because selective clamping does not occlude the main renal artery. In reality, the meta-analysis confirmed the concern about intraoperative bleeding, but combined results from three studies demonstrated that there were no significant differences in blood transfusion rate. The result of blood transfusion rate was limited to the small number of included articles and high heterogeneity, so it remains to be evaluated in the future.
Intraoperative bleeding may result in impaired visualization. We found, however, that the increase in blood loss in the selective clamping group had no impact on positive margins. In addition, patients who underwent the selective clamping PN had a similar overall complication rate to those who underwent hilar clamping PN. Hence, compared with hilar clamping, selective artery clamping was a relatively safe means of vascular control during PN.
In the present study, selective clamping was associated with preservation of short-term renal function. A similar trend was found at 3 months, but the difference did not reach statistical significance. There were no differences in percent change of eGFR at 6 months between the two groups. One possible explanation is that the difference at 6 months should have been statistically significant. The false negative result may be attributed to the small number of articles included in the quantitative analysis. Further, other factors such as variability in surgical techniques and unbalanced patient characteristics may lead to the negative results.
Actually, some patient characteristics such as sex, race, tumor location, and parenchymal volume loss, which may be associated with renal function after PN, were not assessed in our meta-analysis. 24 In a recent review, Mir and coworkers 25 summarized that almost all the variables influencing renal function during PN played their roles by impacting the number of preserved nephrons and recovery from any ischemia associated with the procedure. Therefore, neglect of parenchymal volume loss in study design should arouse our attention.
A second possibility is that there is truly no difference in renal function at 6 months between the two groups. In brief, the selective clamping technique may provide superior renal function after PN at short-term follow-up, but the advantage in preservation of renal functions would disappear over time. A similar phenomenon was shown in a study comparing different methods of hilar clamping during PN. The study suggested that the nonclamping group had a lower percent change in nadir eGFR but was similar in 1-year eGFR when compared with cold ischemia and warm ischemia groups. 8 We could not rule out the possibility of a similar underlying mechanism. In our opinion, it was possible that recovery from ischemia injury caused a similar change in renal function at 6 months.
Previous studies suggested that warm ischemia was one of the primary surgically modifiable factors and led to the functional decline after PN. 6 Then, the selective clamping technique was developed to preserve renal function by minimizing or even eliminating the WIT during PN. There was research to show that ischemic injury could be avoided when WIT was less than 20 minutes. When WIT was 20 to 25 minutes, renal function recovered to normal level in 6 months after surgery. 26 We found WIT in most studies in our review was less than 25 minutes. Thus, there was a chance that the lower-discharge eGFR of patients who underwent hilar clamping had gradually risen because of the recovery of the preserved nephrons related to the ischemic insult. 13,25
Consistent with the hypothesis, a study from Komninos and colleagues 14 found that renal function in the main artery clamp group began to improve from the first postoperative day and continued to improve until 1 year after surgery. More recent research emphasized that renal parenchyma sparing was the primary driver of ultimate renal function after PN with ischemia playing a secondary role. 21,27 –29 In our pool analysis, only a study from Desai and associates 16 took the amount of preserved parenchyma into account, and they found that renal functional outcomes were superior in the superselective cohort at last follow-up (11% vs 17%, P=0.03). 16 Interestingly, greater kidney volume was preserved in the superselective cohort (95% vs 90%, P=0.07).
A study from Simmons and colleagues 30 also suggested that unclamped PN was associated with significantly less parenchymal loss when compared with clamped PN. 30 There is likely a complicated dynamic interaction between parenchymal and ischemia time. 31 Combined with the aforementioned hypothesis, selective clamping may influence the renal function after PN through increasing the number of preserved nephrons, in addition to reducing the WIT. Further investigation is needed, however, to confirm this viewpoint.
The present review had several limitations. First, all studies were retrospective studies without randomization. Group allocation was often based on surgeon preference and even three studies did not provide the means of group allocation. Those may cause significant selection bias. For example, patients in the hilar clamp group were older, although the difference did n0t reach significance. Second, there was insufficient evidence to assess the intermediate-term or long-term renal function outcomes, and more high-quality clinical trials should be conducted. Third, as described previously, parenchymal volume loss is a very important factor influencing postoperative renal function. Only one study took it into account, however. We expect that volume preservation gains more attention. Fourth, some studies failed to provide means and standard deviations for continuous variables. We had to estimate these data with statistical methods.
Conclusions
The present meta-analysis indicated that selective clamping PN was a relatively safe method of vascular control during PN and was associated with improved short-term renal function when compared with hilar clamping PN. Selective clamping, however, may cause greater estimated blood loss, and the benefit in intermediate-term renal function is still controversial. Our review is limited by the small number of selected studies and impact of selection bias. More well-designed studies are needed to investigate this issue in the future.
Footnotes
Acknowledgments
This work was supported by the National Natural Science Foundation of China (Grant No. 31370951 and 31170907), the National Science Foundation for Young Scholars of China (Grant No. 81300579 and 81100494), and the PhD Programs Foundation of Ministry of Education of China (Grant No. 20110181110028).
Disclosure Statement
No competing financial interests exist
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.