
Abstract

VIDEO PRESENTATIONS
VIDEO SESSION 1: LOWER URINARY TRACT OBSTRUCTION – BPH AND URETHRAL STRICTURES
A Novel surgical procedure for fibrotic anterior – Posterior urethral stricture
Procedure: Under general anesthesia anterior urethroplasty procedure was initiated. However, the guide wire passing through the penile mea could proceed only for 3–4 centimeters. Upon that, a penile dissection beginning from the sulcus coronarius until perinea was made. Due to severe anterior urethral stricture, the fibrotic penile -bulbous urethra was completely excised until stricture. The stricture in the posterior urethra was excised until prostate. Interestingly, the prostate was not affected by the stricture. The prostate tissue was dissected all around with scissor and blunt dissection until bladder neck. Even, the bladder neck and tissue surrounding the bladder were dissected bluntly. In order to anastomosis of the prostate urethra to the perineal skin, subcutaneous tissues were excised. Thus, the prostatic tissue is pulled with a babcock clamp to the perinea. 22 ch Foley Catheter was placed through the prostate into the bladder. The perineal skin with excised subcutaneous tissue is anastomised end to end with the prostate tissue by means of the catheter.
Transurethral enucleation of prostate using button electrode (TUEP-B) for the treatment of clinical obstructing benign prostate hyperplasia
We performed a Transurethral Enucleation of Prostate with Button electrode (TUEP-B) following by the resection of “peduncolated adenoma with a
The procedure was completed using Olympus
We performed a Transurethral Enucleation of Prostate with Button electrode (TUEP-B) following by the resection of “peduncolated adenoma with a
The procedure was completed using Olympus
Single-port transvesical enucleation of the prostate for the patients with large prostatic adenoma
VHS Medical Center, Seoul, Korea Republic

Hallym University Dongtan Sacred Heart Hospital, Hwaseong-si, Korea Republic
The Smith Institue for Urology, New Hyde Park, USA
Asklepios Hospital Barmbek, Department of Urology, Hamburg, Germany
HoLEP is an endoscopic challenging procedure first introduced in 1998, now many investigators consider HoLEP the new gold standard.
Surgeon search for the capsular plane by making two incisions at the 5 and 7 o'clock positions beginning at the bladder neck, until the circular neck's fibers are exposed, and proceed till the verumontanum deepening and widening the incision separating the lateral lobes from the median portion.
In the apex region, push laterally with the instrument detaching the adenoma from the capsule, with the laser turned off, producing detachment of the lateral lobe.
The transversal incision in front of the verum allows to detect the cleavage plane at the level of the lateral incisions and to free the median lobe in retrograde fashion.
Lift and push the median lobe distally detaching it along the groove plane until the circular neck's fibers are visualized.
The incision of the anterior commissure should begin, at the apex, at the 12 o'clock position and proceeding in retrograde fashion until the neck is reached.
Extend the central incision, at the level of the neck, from the 11 to 1 o'clock positions, creating a space to insert the instrument allowing to push the lobe in a posterior direction uncovering the cleavage plane which is opened by the laser's action.
Enucleate the lateral lobe beginning at the cleavage plane at the 6 o'clock position until detachment is achieved at the level of the neck.
During the hemostasis, use warm irrigation fluid, inspect for small arteries to coagulate using a high energy for 2–3 seconds defocusing the laser to 2–3 mm.
Use warm irrigation liquid to the distended bladder during morcellation; after engaging the specimen bring it to the center of the bladder, morcellation could be expedited by moving in and out the instrument and sometimes by slowing the blades' velocity.
Laparoscopic simple prostatectomy: 8 years experience
Bipolar Plasma Enucleation of the Prostate (BPEP). Alternative approach for oversized adenomas
Bioclinic Hospital, Athens, Greece
Recently the TURIS-plasma vaporization (TURIS-V) technique, which uses the Gyrus PK plasma vaporization generator and ‘button’ vaporization electrode, was introduced in clinical practice. We evaluated our results with Transurethral in saline Vaporization with Button electrode (TUVP-B) for the treatment of bladder outlet obstruction (BOO) due to benign prostatic hyperplasia (BPH).
Following surgery, we evaluated Hb's dosage, bladder irrigation's time, catheterization time, RUA post B-TUVP, hospital stay and <30 days hospital patient readmissions.
Patients were assessed after 30 days from the surgical procedure and then every 3 months, using PSA and HB dosage, IPSS, IEFF-5, QOL, Uroflowmetry with PVR. Postoperatively, TRUS was performed 6 months.
All the patients showing during follow-up a reduction of Qmax (<15 ml/sec) or an increasing of IPPS or RPM (>50 ml), underwent an endoscopic second look.
Randomized comparison study on clinical outcomes in the treatment of benign obstructing prostate with Gyrus PK Resection using 120 watt power versus standard 180 watt. Preliminar results
The average age of the patients was 71,5 yrs (range 54–89 yrs) and medium follow-up 13 months (range 19–7 mo.). The preoperative investigation protocol included : digital rectal examination (DRE), Prostatic Specific Antigen (PSA), International Prostate symptom Score (IPSS), Quality of Life (QOL), urinalysis with urine culture, uroflowmetry with post-voiding residual urinary volume (PVR) and transrectal ultrasonography assessing prostate volume. During surgery, intraoperatively, we evaluated total Bipolar TURP time, including total resection's time and prostate's and adenoma's weight. Before surgery, perioperatively we evaluated Hb dosage, bladder irrigation's time, catheterization's time, RUA post B-TUEP, hospital's stay and <30 days in hospital patient readmissions. Patients were assessed after 30 days from the surgical procedure and then every 3 months, using PSA and HB dosage, IPSS, IEFF-5, QOL, Uroflowmetry with PVR. The patients were evaluated after 6 and 12 months using TRUS (to evaluate residual prostate volume).
No death after operation in both groups.
Six months after no patients of 120 watt group but two patients of 180 watt group have had re-endoscopic operation for bladder outlet obstruction.
Combined laparoscopic treatment of benign prostatic hyperplasia complicated with large bladder stone
Urological Center of Russian Railways Hospital, Nizhny Novgorod, Russia
Civil Aviation Central Clinical Hospital, Moscow, Russia
1 patient underwent robot-assisted laparoscopic retropubic prostatectomy, 2 – transvesical laparoscopic simple prostatectomy and for other 38 patients extraperitoneal retropubic simple prostatectomies were performed. BPH enucleation was performed using an ultrasonic dissector “Harmonic” Hemostasis was achieved with bipolar coagulation or radiofrequency coagulation by “LigaSure” and with suturing the prostate capsule. 26 patients underwent trigonisation of bladder neck with “Polysorb” No 4.0 together with excision of the prostatic urethra. In the remaining 15 cases, “urethral area” has been saved. Prostate capsule was sutured using intracorporeal continuous or nodal joints “Polysorb” No 2.0.
VIDEO SESSION 2: UROTHELIAL CANCER
Department of Urology, Department of Pathology, National Oncology Hospital Sofia, Bulgaria
EARLY EXPERIENCE OF TRANSURETHRAL BIPOLAR PLASMA VAPORIZATION FOR THE TREATMENT OF NON-MUSCLE INVASIVE BLADDER TUMOR
VHS Medical Center, Seoul, Korea Republic
Urinary diversion was reconstructed as intracorporal ureterocutaneostomy in six and as extracorporal ileum conduit in one patient.
Surgery lasted 296,85 min, thereof 199,71 min console time on average. There was no need of a conversion to open surgery. The mean blood loss was 238 ml and none of the patients required blood transfusions. Resection margins were tumor-free in six cases. In the patient with positive resection margins the tumor stage was pT4a.
Postoperative complications occurred in two of the patients: paralytic Ileus (Clavien-Dindo class 1 (CDC 1) in one patient and port hernia (CDC 3b) in the other patient.
ROBOT-ASSISTED RADICAL CYSTECTOMY, LYMPH NODE DISSECTION, AND FULLY INTRACORPORAL ILEAL CONDUIT RECONSTRUCTION DIVERSION BY PATIENTS WITH MUSCLE-INVASIVE UROTHELIAL BLADDER CANCER
Alfried Krupp Krankenhaus, Essen, Germany
LAPAROSCOPIC PARTIAL CYSTECTOMY IN URACHAL DISEASES
LAPAROSCOPIC PROSTATE-SPARING RADICAL CYSTECTOMY; CASE REPORT
APPROACH TO THE BLADDER TUMORS WHICH HAS UNUSUAL AND INACCESSIBLE LOCALIZATION FOR CONVENTIONAL TECHNIQUES: LASER VAPORIZATION TREATMENT FOR BLADDER TUMORS: DIFFICULT CASE
LAPAROSCOPIC RADICAL CYSTECTOMY: ULUDAG UNIVERSITY EXPERIENCE
ROBOTIC RADICAL CYSTECTOMY WITH INTRACORPOREAL ORTHOTOPIC ILEAL NEOBLADDER. ORIGINAL TECHNIQUE
TURB EN BLOC WITH PLASMAKINETIC BUTTON TURIS: IS A BETTER TREATMENT?
THULIUM:YAG LASER EN BLOC RESECTION OF BLADDER TUMORS (TmLRBT) FOR TREATMENT AND PATHOHISTOLOGICAL STAGING
Hannover Medical School, Hannover, Germany
Surgical Procedure: An incision into the circumference of the tumor with a safety margin of 2 mm to the tumor was performed with a 550 nm laser fibre that was advanced through a 26 F continuous-flow resectoscope. The 2013 μm Tm:YAG laser was used at the power level of 10–15 Watts. After incicion, the mucosa was bluntly dissected from the deeper layers leaving the bladder facing part of the specimen intact. The tumor was extracted endoscopically in one piece with a grasper. Two cold-cut biopsies were taken from the tumor ground.
ILEAL CONDUIT ENDOSCOPY – SURGICAL VIDEO
To our knowledge this is the first time a looposcopy video with LASER resection is showed.
VIDEO SESSION 3: RENAL - URETERAL SURGERY I
TOTALLY INTRACORPOREAL LAPAROSCOPIC RADICAL CYSTECTOMY WITH ORTHOTOPIC “U” SHAPED ILEAL NEOBLADDER: TECHNIQUE DESCRIPTION, ONCOLOGIC AND FUNCTIONAL OUTCOMES OF THE FIRST THIRTY PATIENTS
Sapienza Università di Roma, Facoltà di Farmacia e Medicina, Dipartimento di Scienze e Biotecnologie Medico-Chirurgiche, UOC Urologia, ICOT
The demographic data were: 30 male patients, median age 67 years (range: 62–79), BMI 22.3; (16–26.1), mean ASA score 2,2 (1–3); clinical stage (cT1 12 pts; cT2 15 pts; cT3 2 pts; cT4 1 pt, concomitavt CIS 7 pts).
A 40 cm. segment of ileum 20 cm. from the ileocecal junction was isolated, and ileo-ileal continuity was restored using Endo-GIA staplers (U.S. Surgical, Norwalk, Connecticut). The isolated ileal segment were detubularized and a globular U shaped ileal neobladder was constructed and anastomosed to the urethra with a 3-0 barbed suture, using the Van Velthoven technique. Bilateral stented ureteroileal anastomoses were individually performed to the proximal ileal segment of the neobladder. The entire procedure was completed intracorporeally.
We present our data on our experience with LRC with pure intracorporeal neobladder diversion all performed by a single laparoscopic skilled surgeon. Our data suggests that localized muscle invasive bladder cancer can be successfully treated by LRC. We achieve operating times, intra-operative blood loss, and length of hospital stays comparable with the largest published series. We reported an overall complication rate similar to the data reported in literature. Moreover most of the complications, about 70% (12/17) were treated conservatively with no further surgical intervention required and were classified as low grade Clavien complications (1 and 2). The remaining five patients required re-operations (four minimally invasive endoscopic procedures, and only one major open surgery due to an ileal pouch fistula occurred 56 days after LRC). The major complication rate reported in our study is comparable to previous studies and remains less than ORC procedures. Haber et al. compared 25 consecutive LRCs with a contemporary cohort of 25 ORCs with urinary diversion (14 ileal conduits, 11 orthotopic neobladders). Operative time, blood loss, transfusion rate and ileus were lower in the LRC group (P<0.05). There were no significant differences between the groups as regards oral intake, time to ambulation, postoperative complications and hospital stay [17].
Huang et al. reported the largest series to date, where 171 patients underwent LRC [18]. Their median operative time was 325 minutes with a median blood loss of 270 mL. They reported a total complication rate of 39.2% (67/171), with 6.4% (11/171) CC I complications, 19.3% (33/171) CC II complications, and 13.5% (23/171) CC III complications. All studies reported more complications in patients who had orthotopic neobladder substitution, as compared to ileal conduits. This would explain why Huang et al. have a higher complication rate than other studies, as they only performed neobladder procedures.
It is evident that there is a significant variability in results reported regarding operative data, as well as complication rates. These data reflects the surgeon expertise and the volume of different centres, and highlights that there is not still an accordance in literature over operative procedure and urinary diversion technique in laparoscopic surgery.
Aboumarzouk et al. in a retrospective study compared 155 patients who underwent LRC or ORC with a mean follow-up of 53 months. The authors reported that ORC group had shorter operative times (p<0.0001), more blood loss with more transfusion requirement (p<0.00001), and a longer hospitalization. No difference was found regarding lymph node yield, positive margins, pathologic results and positive lymph nodes. The ORC group had less intraoperative complications (p=0.03). No significant difference was found between the two groups regarding 5-year overall survival, cancer-specific survival, and recurrence-free survival. They concluded that LRC may be considered as an alternative to ORC with good operative results in addition to comparable oncologic outcomes [19]. In two recent published systematic reviews, which evaluated 19 studies comparing ORC to LRC as well as robot-assisted radical cystectomy (RARC), was not able to show superiority of one modality to the other [20,21]. The authors conclude that despite the select cohort of patients included in the LRC and RRC groups compared to the non-selective ORC group, they were unable to highlight a clear impact regarding oncological outcomes. The two reviews agree that the LRC and RARC results are encouraging thus to support the diffusion of these mininvasive techniques. What seems to become an upcoming evidence is that improved skills and experience of surgeons, LRC might replace ORC. Ass well known, robotics is rapidly replacing laparoscopy due to its shorter learning curve and at least similar if not better operative and post-operative results. In a prospective comparative analysis between LRC and RARC with ileal conduit urinary diversion, Abraham et al. reported that both laparoscopic and robot-assisted radical cystectomies can be performed safely without compromising oncologic standards for surgical margins and extent of lymphadenectomy. In this experience, the robotic approach appears to have a shorter learning curve, and it is associated with less blood loss, fewer complications, and earlier return of bowel function than LRC [22]. Furthermore, two prospective controlled randomised trials comparing robotic radical cystectomy to open radical cystectomy noted that RARC significantly decreased estimated blood loss with a reduced transfusion rate, operative time and analgesic use. No significant difference were observed regarding complications, length of hospital stay or pathological outcomes [23,24]. In our experience pure LRC with orthotopic neobladder in male patients with invasive bladder carcinoma results safe, feasible as radical tumor resection, and offers less invasiveness with a quicker associated recovery. With the improvement of laparoscopic techniques and renovation of equipments[5], pure LRC with an orthotopic neobladder is maturing. Compared to open procedure, LRC with an orthotopic neobladder has 3 principal advantages. First, clearer operative view facilitates meticulous dissection and less injury of the pelvic floor structure improves the early postoperative continence recovery. Second, each dissection is performed with good haemostasis, and the pneumo-peritoneal pressure could also decrease the venous hemorrhage. Third, the last but not the least, the bowel is never exposed extracorporeally. Less invasive manipulation of the bowel was associated, in our case series, with quicker functional recovery of the intestinal tract and lower the incidence of related postoperative complications. The main limit of this study could be represented by the sample size and by the mean range of follow-up; however, the aim of this study is to report our experience of LRC with total intracorporeal orthotopic neobladder diversion performed by the same surgeon with the same reconstructive technique.
A larger multi-institutional analysis with a long term follow-up comparing laparoscopic, open, and robotic radical cystectomy is needed to finally establish the superiority of one procedure over the others.
LAPAROSCOPIC MASS ENUCLEATION WITHOUT ISCHEMIA IN SMALL RENAL MASSES
TRANSVAGINALLY ASSISTED MINI-LAPAROSCOPIC RADICAL NEPHRECTOMY
POTPOURRI OF ROBOTIC PARTIAL NEPHRECTOMY: EGE UNIVERSITY EXPERIENCE
Third patient was a 32 year old male with a 2×2.5 cm left lateral solid renal mass. All three patients underwent transperitoneal robotic partial nephrectomy with 3-arm approach utilizing 5 ports. Only the renal artery was clamped for the first patient, both the renal artery and renal vein were clamped for the second patient and the third patient underwent unclamped technique. The first two masses were excised with cold scissors while the last one was excised hot. Renal reconstruction was performed with horizontal mattress suturing technique using 0 vicryl with the aid of sliding Weck clips.
INTERDISCIPLINARY SURGICAL MANAGEMENT OF A CASE OF RENAL TUMOR WITH MASSIVE VENOUS THROMBUS EXTENDING INTO INFERIOR VENA CAVA (T3b)
Municipal Clinical Hospital Cluj-Napoca, Romania
A 56-year-old male presented to our service complaining of right sided lumbago and gross hematuria during the recent one month. Complete physical examination revealed Grade 2 hypertension. Laboratory tests showed secondary anemia. Contrast-enhanced computed tomography showed a tumor in the upper half of the right kidney 8.5 cm in diameter. Doppler abdominal ultrasonography demonstrated a massive tumor thrombus extending to the Inferior Vena Cava with a distal apex 8 cm from the right atrium. No distant metastasis was recognized in the preoperative radiological studies.
Right radical nephrectomy with tumor thrombectomy was succesfully performed. After adequate vascular control of the Inferior Vena Cava and bilateral renal veins, the radical nephrectomy was performed followed by disection of the inferior vena cava wall and removal of the thrombus. The urological surgical team was asisted by a general surgeon for the isolation of the main billiary duct and by a vascular surgeon for the thrombectomy. As a final operating stage a retroperitoneal lymphadenectomy was performed. Total operating time was 2 hours 20 minutes with a blood loss of 1200 ml. Postoperative evolution was favorable. Pathological analysis of the surgical specimen revealed a Fuhrman 4 renal cell carcinoma with extracapsular invasion and no lymph node metastasis (pT3bNoMoV1Lo).
3-months and 6-months follow-up consisted of clinical examination, laboratory tests and contrast enhanced computed tomography with no evidence of disease.
LAPAROSCOPIC PARTIAL NEPHRECTOMY: ULUDAG UNIVERSITY EXPERIENCE
STEP BY STEP ROBOTIC ASSISTED LAPAROSCOPIC TRANSPERITONEAL RADICAL NEPHRECTOMY: 8 CM LEFT KIDNEY MASS
Department of Urology, Gulhane Military Medical Academy, Ankara, Turkey
The retroperitoneal space is prepared. The Psoas muscle is identified and the kidney is lifted up. The azigo-lumbar vein is identified, clipped and transected. The left renal artery is dissected. A vessel loop is passed around it and exteriorized through the trocar site. The tumor is exposed. The fatty tissue overlaying it is dissected and sent for histological examination. The healthy tissue around the tumour is incised in order to find the correct cleavage plane between the mass and the kidney. This plane is developed with blunt and sharp dissection. A small vessels going to the tumor is clipped and cut. The vessel loop is released. At the end of this step a running suture using a 0 vicryl 36 needle is performed to obtain good haemostasis. A hem-o-lok is placed at each passage in order to apply enough tension to the suture. Finally Floseal gel is placed over the resected area.
IPSILATERAL COMBINATION OF KIDNEY CANCER & STAGHORN NEPHROLITHIASIS. WHAT TO DO?
Urological Center of Russian Railways Hospital, Nizhny Novgorod, Russia
TRANSMESOCOLIC LAPAROSCOPIC RADICAL NEPHRECTOMY
Urological Center of Russian Railways Hospital, Nizhny Novgorod, Russia
St. Luca's Clinical Hospital, St. Petersburg, Russia
St. Luca's Clinical Hospital, St. Petersburg, Russia
LAPAROSCOPIC TREATMENT OF RENAL HYDATID CYST
FIRST EXPERIENCE LAPAROSCOPIC PYELOPLASTY FOR URETEROPELVIC JUNCTION OBSTRUCTION IN MALANG, INDONESIA: A CASE REPORT
Resident – Departement of Urology Saiful Anwar General Hospital, Malang, Indonesia
Istanbul Medeniyet University Goztepe Training Hospital, Turkey
Istanbul Medeniyet University Goztepe Training Hospital Department of Urology, Turkey
VIDEO SESSION 4: PROSTATE CANCER
SOC Urologia, Ospedale “San Lazzaro” di Alba, CN
The aim of this study was to evaluate the versatility (hemostasis, sealing, cutting, dissection capability and tissue manipulation) of THUNDERBEAT in laparoscopic non nerve sparing radical prostatectomy.
ROBOTIC RADICAL PROSTATECTOMY FOR VARIOUS CLINICAL SCENARIOS: EGE UNIVERSITY EXPERIENCE
VESICOURETHRAL ANASTOMOSIS DURING ROBOT-ASSISTED LAPAROSCOPIC PROSTATECTOMY USING A UNIQUE BIDIRECTIONAL BARBED SUTURE
LAPAROSCOPIC RADICAL PROSTATECTOMY: 10 YEARS EXPERIENCE
MANAGEMENT OF LARGE MEDIAN LOBE DURING ROBOT ASSISTED LAPAROSCOPIC RADICAL PROSTATECTOMY
STEP BY STEP ROBOTIC ASSISTED LAPAROSCOPIC RADICAL PROSTATECTOMY: RESIDENT TRAINING
Department of Urology, Gulhane Military Medical Academy, Ankara, Turkey
POSTERIOR RECONSTRUCTION AND VESICOURETHRAL ANASTOMOSIS IN EXTRAPERITONEAL LAPAROSCOPIC RADICAL PROSTATECTOMY USING NEW GENERATION BARBED POLYGLICONATE SUTUR (V-LOC)
VIDEO SESSION 5: LYMPH NODE DISSECTION, SACROPEXY AND INCONTINENCE, VESECTOMY REVERSAL
LAPAROSCOPIC RETROPERITONEAL LYMPHADENECTOMY IN TECHNICAL ASPECTS
Moscow Oncourological Hospital No 62, Moscow, Russia
Urology Clinic, Military Medical Academy, Belgrade, Serbia,
Department of Urology, VKF American Hospital, Istanbul, Turkey
School of Medicine, Koc University, Istanbul, Turkey
SURGICAL TECHNIQUE, SURGICAL BENCHMARKS AND IMPACT OF TEAM CONSTANCY ON SURGICAL DURATION IN ROBOT-ASSISTED ISOLATED SACROUTEROPEXY/SACROCOLPOPEXY AND SACROUTEROPEXY/SACROCOLPOPEXY COMBINED WITH MODIFIED BURCH COLPOSUSPENSION PROCEDURE
LAPAROSCOPIC BILATERAL CERVICOSACROPEXY (CESA) IN TUNNELING TECHNIQUE
Department of Urology, Charité University, Berlin, Germany
Operative technique: local anesthesia (LA) was performed by using a topical application of eutectic mixture of local anaesthetic cream (EMLA®) on vaginal mucosa 20 minutes before the procedure and then by local injection of lidocaine 2% (10 cc) and ropivacaine 7,5% (10 cc) in the transobturator site of needle passage. The Monarc® procedure was performed following strict guidelines of the manufacturer (American Medical System). All patients were discharged from operative room without catheter.
Intra and postoperative pain (Visual Analogue Scale, VAS), rate of complications, operative times, patient satisfaction through VAS Satisfaction scale, and Post-Anaesthesia Discharge Scoring System (PADSS) at one and four hour (patient were dischargeable with a PADSS ≥9) were recorded.
No cases of postoperative urinary retention were recorded. The time to first urination was 2.6 hours. Mean post-voiding residual at first micturition was 40 ml.
This study suggests that Monarc® procedure in LA is safe and feasible.
ADVANCE MALE SLING FOR RECURRENT URINARY INCONTINENCE AFTER INVANCE SLING PLACEMENT IN PATIENT WITH INFLATABLE PENILE PROSTHESIS
Since 2012 the patient presented recurrent moderate SUI. Mobility and residual function of the sphincter are tested by cystoscopy repositioning test and urodinamic evaluation.
After antibiotics prophylaxis (Ceftriaxone and Amikacina) a 14 French Foley catheter is inserted and 4-cm midline perineal incision is made. Identification of the Invance® sling, which is then completed removed. Bulbospongiosus muscle was identified and split, the central tendon is detached partially exposing the underlying urethra. The transobturator fossa is accessed with the helical trocar via an outside-in approach. After each steps IPP was tested to confirm its functionality. The sling was then placed following strict guidelines of the manufacturer; tension is applied to the sling to elevate and repositioning the proximal urethra.
SELF CREATED TRANSOBTURATOR TAPE FOR STRESS URINARY INCONTINENCE
ROBOT ASSISTED LAPAROSCOPIC COLPOSACROPEXY: OUR TECHNIQUE STEP BY STEP
INTRACORPOREAL ROBOT-ASSISTED BILATERAL VASOVASOSTOMY, AFTER BILATERAL VASECTOMY
VIDEO SESSION 6: RENAL - URETERAL SURGERY II
URGENT KIDNEY DESOBSTRUCTION – A ROUTINE EVERYDAY PRACTICE OR A CHALLENGE
Department of Urology, University Hospital for Urgent Medicine “Pirogov”, Sofia, Bulgaria
Thanks to the immediate desobstruction we achieve pain relief, normalization of the creatinine and urea and time to consider the cardiovascular, neurological, coagulation and other issues of the general condition before undertaking the major surgery for solving the entire health problem. Minor perioperative complications linked to the procedure were observed such as fever (4 cases), gross haematuria lasting more than 2 days (3 cases), dysuria (6 cases), frequency- (2 cases), transurethral protrusion of the stent in female patients- (3 cases). For this period open surgery was necessary in 3 cases despite kidney desobsruction with PNS because persistent fever and presence of sepsis, where nephrectomy was done.
4, th Department of Urolgoy, Iaso General Hospital, Athens, Greece
Hannover Medical School (MHH), Hannover, Germany
ENDOSCOPIC REMOVAL OF A LARGE URETERAL POLYP
The operation was performed in the standard endoscopic operation theatre with the possibility of intraoperative x-ray control. On the first step the patient underwent rigid cystoscopy, according to which a large floating ureteral polyp, coming up from the right orifice was determined. The distal pole of the polyp captured and then pulled by endoscopic forceps with the purpose of subsequent ureteroscopy possibility according to the huge polyp size. A rigid videoyreteropyeloscope Olympus EndoEye was held in the right ureter beside the polyp. Instrument was delivered to the proximal end of the polyp in the upper third of the ureter. Precious holmium laser resection of the proximal polyp part was performed. The emergence of active bleeding was not observed. After the polyp mass extraction, the “cold” biopsy of the polyp base was performed. As a final step, we made laser ablation of the base of the polyp to prevent the possible disease recurrence. The right kidney was drained by double-J stent. The procedure duration limited up to 30 minutes. The total length of the removed polyp was about 17 cm.
ROBOTIC PYELOPLASTY FOR SECONDARY URETEROPELVIC JUNCTION OBSTRUCTION OBSTRUCTION: 3-ARM APPROACH
ROBOTIC URETERONEOCISTOSTOMY FOR SEVERE URETERAL ENDOMETRIOSIS - SURGICAL TECHNIQUE AND RESULTS OF AN INITIAL EXPERIENCE
The robotic system DaVinci®, can hugely ease the surgical maneuvers during reconstructive procedures and so can find an optimal field of application in the multidisciplinary management of DIE.
The video presents our experience with 3 consecutive cases submitted to robotic ureteroneocystostomy for endometriosis.
Preparation for robotic ureteroneocystostomy resembled radical prostatectomy, with the patient in Trendelemburg position with divaricated legs and a W-shaped port placement for 3 robotic arms and 1 or 2 assistant's ports; 0° optic was used; an uterine manipulator was inserted through the vagina.
The first step was the resection of all the pelvic sites involved by DIE, including a large partial cystectomy for the patients with the bladder involvement.
Then the ureter of the affected side was isolated, cranially up to an healthy segment, caudally to the intravesical tract. Once the ureter was completely freed from the adherences due to DIE, it was evaluated in terms of vitality and patency, irrigating the nephrostomy: in all the cases the obstruction was not relieved by the ureterolysis. So, the pelvic ureter was resected, the bladder extensively mobilized and an ureteroneocystostomy according to a modified Lich-Gregoir technique performed, with a 4-0 monofilament suture.
LAPAROSCOPIC ADRENALECTOMY: ULUDAG UNIVERSITY EXPERIENCE
LAPAROSCOPIC TRANSPERITONEAL HEMINEPHRECTOMY IN ADULTS WITH DUPLICATED RENAL COLLECTING SYSTEMS
ROBOT ASSISTED URETERAL RECONSTRUCTION IN 3 PATIENTS
PURE LAPAROSCOPIC VENA CAVA BLEEDING MANAGEMENT AND CONTROL DURING RIGHT LIVE DONOR NEPHRECTOMY
1) Pure laparoscopic right donor nephrectomy: step-by-step approach. Abrahams J Endourol. 2004 Apr;18(3):221–5; discussion 225. Department of Urology, University of California School of Medicine, San Francisco, California 94143-0738, USA.
2) The Hem-o-lok clip is safe for laparoscopic nephrectomy: a multi-institutional review. Ponsky, Cherullo E, Moinzadeh A, Desai M, Kaouk J, Finelli A, Frank I, Matin S. Center for Urologic Oncology and Minimally Invasive Therapies, Case Western Reserve University, University Hospitals, Cleveland, Ohio 44106, USA.
3) Vascular clips are safe and a great cost-effective technique for arterial and venous control in laparoscopic nephrectomy: single-center experience with 1834 laparoscopic nephrectomies.Simforoosh
4) J Endourol. 2006 Jul;20(7):467–9; discussion 469–70. Methods of vascular control during laparoscopic donor nephrectomy. Sundaram Department of Urology, Indiana University School of Medicine, Indianapolis, Indiana 46202-5289, USA.
5) Ann Surg. 2006 Jan;243(1):126–30. Fatal and nonfatal hemorrhagic complications of living kidney donation. Friedman AL1, Meng MV, Freise CE, Stoller ML., Sarhangnejad R, Basiri A Nouralizadeh A, Kashi AH, Moosanejad N., Bargman V, Bernie JE., Peters TG, Jones KW, Boulware LE, Ratner LE. never use Hemolock clips at least for Right sided Live donor Nephrectomies.
LAPAROSCOPIC ILEAL URETER
City Clinical Hospital Nr. 40, Yekaterinburg, Russia
Individual attention iatrogenic ureteral injury when endourological interventions on the upper urinary tract urolithiasis. The frequency of intraoperative complications of traumatic and mechanical character is in contact stone removal method is quite high. The total percentage of such complications as high as 10%. These include - ureteral wall contusion (3%), hematoma formation (3%), ureteral perforation (1%), rupture of the walls and a complete separation of the ureter (1%) (Marberger M., Fitzpatrick JM, Jenkins AD, et al., 1998, 2004).
Ureter injury scale (American Association for the Surgery of Trauma-Organ Injury Scale, AAST-OIS (2002)
Grade* Type of injury Description of injury
I Hematoma Contusion or hematoma without devascularization
II Laceration<50% transection
III Laceration≥50% transection
IV Laceration Complete transection with <2 cm devascularization
V Laceration Avulsion with >2 cm of devascularization
*Advance one grade for bilateral up to grade III.
May 2010, during ureterolithotripsy occurred avulsion (complete detachment) right ureter - V grade AAST-OIS. July 2010, underwent surgery - laparoscopic Ileal ureteral substitution,
The patient was discharged home healthy. The patient returned to his usual activities. Biochemical markers (serum creatinine, electrolytes), ultrasonography within the normal range. Chest x
X-rays and CT scans after 1.5 and 7 months (Fig. 3,4.)


Civil Aviation Central Clinical Hospital, Moscow, Russia
Position the patient - Trendelenburg (10*) turned left (30*). Were used 5 trocars (3 – robot, 2 - assistant), three of which were set through the hernia after mobilization of fixed seals, bowel. Docking DaVinci Si. After mobilization in middle part, extended to 1 cm right ureter had been cut over the dense scar on the alleged infiltration level crossing over the iliac vessels with no possibility of identifying the latter. Previously installed JJ- stent removed. Flap is cut from the bladder's wall. Ureterocystoanastomosis interrupted sutures (Vicryl 4.0) was performed. The ureter in the pelvis held drainage - intubator; the distal end of it antegradely withdrawn through the urethra. On the intubator was done tubularization of the flap with interrupted sutures (Vicryl 4.0). Bladder's incision was sealed with a continuous suture. Filled through a urethral catheter to150 ml bladder demonstrated no leaks. Area of operation drained.
At follow-up in a month: an adequate amount of urination, dysuria absence, further regression of right hydronephrosis, no vesico-ureteral reflux.
PRONE POSITION RETROPERITONEAL APPROACH LESS ADRENALECTOMY
APPENDOPLASTY FOR EXTENDED URETERIC STRICTURES
Civil Aviation Central Clinical Hospital, Moscow, Russia
At the initial stage we identified appendix and appreciated its length. Then typical appendectomy was done with preservation vascular pedicle – very important for following success of operation. Following stage was transformation blind cavity of appendix in through tube. For this sake the apex of appendix was cut off, and its cavity was irrigated to remove intestine contents. Then we cut the ureter upper the stricture within intact tissues for future appendo-ureteral anastomosis: bleeding of its margins confirmed its vitality. Also important was to prepare the place for appendo-vesical anastomosis in bladder.
To avoid tension of this anastomosis we brought down to the bladder the appendix with its vascular pedicle and fixed it with some stitches. Opening the bladder cavity in the previously prepared area and end-to-end appendo-vesical anastomosis. For this we used interrupted sutures an three zero vycril. As soon as we completed posterior wall of anastomosis we introduced guide through appendix into the bladder and via this guide we brought down to it the J-J stent. After finishing lower anastomosis we were prepared to undergo upper one which was uretero-appendicular. We cut off the damaged tissue of ureter and spatulated its ends. Firstly guide and then J-J stent were introduced from appendix up to the pelvis of the right kidney. And at this stage we performed anastomosis between appendix and upper third of ureter around the stent with interrupted three zero vycril sutures. Passage of right upper urinary tract was restored. Drainages to small pelvis and upper anastomosis.
J-J stent was removed in 1 month and pyeloureterography was performed: passage was sufficient, nephrostome was removed. In 6 month ureteroscopy revealed no strictures or any other obstruction. No acute pyelonephritis occurred with the patient for 1 year of surviliance.
Central City Hospital No. 3, Ekaterinburg, Russia
In 7 months CT and intravenous urography demonstrated no signs of stricture and reflux, sufficient function of the kidney.
Transpertioneally we placed 3 ports at the left lateral position. After mobilisation of the ascending colon medially, the ureter was identified and dissected from IVC upwards. The excessive retrocaval ureteral segment was excised and a single stone of 2 cm located at the dilated proximal ureter was extracted with the aid of flexible nephroscope. A double-j stent was placed and after spatulating the end of distal segment, ureteral anastomosis was performed with no tension. No complication was observed during or after surgery. The drain was removed at postoperative day 3 and the patient was discharged uneventfully.
VIDEO SESSION 7: UROLITHIASIS
PCNL IN GALDAKAO-VALDIVIA SUPINE POSITION
Zvezdara University Medical Center, Belgrade, Serbia
ENDOSCOPIC EXTRACTION OF A SEVERELY ENCRUSTED LONG FORGOTTEN INDWELLING URETERIC STENT
Urology Clinic, Military Medical Academy, Belgrade, Serbia,
ROBOTIC ASSISTED LAPAROSCOPIC AND ENDOSCOPIC FLEXIBLE PYELOSCOPIC MANAGMENT OF PYELOURETERAL JUNCTION STENOSIS AND NEPHROLITHIASIS
Iaso General, Athens, Greece
Robotic Pyelolithotomy is considered one of the options for management of renal stones. Currently there are supporting data for use in patients with certain anatomical variations and in whom approach with URS or PCNL is difficult.
We present a 23 year old female known to have cerebral palsy with severe scoliosis, upper and lower limb contractures presenting with recurrent UTI and left radio-opaque renal stone measuring 1.8 cm, attempt of ESWL was unsuccessful to fragment the stone
Due to difficult positioning for URS/PCNL, and making her stone free would be unlikely, we attempted Robotic left Pyelolithotomy, with a total OR time of 245 minutes and blood loss of 50 ml, she was discharged on day three stone free.
We conclude that robotic/laparoscopic Pyelolithotomy is a valid option for patients with anatomical variations and in who are approach with URS or PCNL would be unfeasible.
CYSTOLITHOTRIPSY FOR LARGE AND/OR MULTIPLE BLADDER STONES: OUR TECHNIQUE
National Police Hospital, Korea Republic
University Hospital, Sofia, Bulgaria
-How to use laser beam and energy in the most effective way?
-How to decrease procedure and anesthesia time?
-How to disintegrate the stone into the smallest possible fragments allowing easy and full evacuation?
Using this technique the disintegration starts with making horizontal and vertical (if needed) channels into the stone. The channels are increased in width and depth using the maximum effectiveness of laser beam as it always in contact with the stone matrix.
ENDOSCOPIC COMBINED INTRA-RENAL SURGERY FOR STONES IN CHILDHOOD
BIOCLINIC Hospital, Athens, Greece
Percutaneus access is preferably done into the lower calyx. Track dilatation is carried out until placement of a 18Fr Amplatz sheath. A flexible 16Fr cysto-Nephroscope or a 17Fr rigid Nephroscope can by used to access and disintegrate stones with the aid of Holmium Laser.
Retrograde access is achieved by catheterizing the ureteric orifice with 0,035 nitinol hydrophilic wire via a pediatric cystoscope. A 7,5Fr flexible ureteroscope is passively advanced over the wire without light or irrigation attachments. This “cordless” advancement without use of ureteric access sheath minimizes the risk of ureteric injury.
This method allows us to exploit the full potential of the endourological armamentarium accessing and delivering treatment in the most remote intra-renal locations. It harvests the advantages of the percutaneous and ureteronephroscopic approaches without stretching either to their limit. This means no need for multiple percutaneous tracks and smaller caliber sheaths for PCNL. It also means no need for long procedures under high intrarenal pressures during lengthy RIRS. The bulk of the stone is ferried through the percutaneous sheath. The latter is usually parked in the renal pelvis via the posterior lower calyx. The flexible ureteroscope deals with inapproachable stones. There is no need to take the extra time to pulverize the stones, just brake in large pieces and present them to the nephroscope (passing the ball technique).
ECIRS is the method of choice for such complex cases when patients are in absolute need of becoming stone free with the less possible number of interventions. To our knowledge it has not been used in children although it maximizes safety and effectiveness and this is very important for the young patient.
REMOVAL OF STONE ENCRUSTATED DOUBLE J STENT IN A SOLITARY KIDNEY WITH THE HELP OF URETERORENOSCOPY AND FLUOROSCOPIC GUIDANCE
MANAGEMENT OF URETEROPELVIC JUNCTION OBSTRUCTION ASSOCIATED WITH A RENAL STONE
RETROGRADE INTRARENAL LITHOTRIPSY (RIRS) FOR STONES >2.5 CM. OUR EXPERIENCE AND TECHNIQUE
Blue Cross Hospital, Athens, Greece
BIOCLINIC Hospital, Athens, Greece
VIDEO SESSION 8: RARE UROLOGICAL CONDITIONS
LAPAROSCOPIC APPROACH IN RARE UROLOGIC DISEASES
Tamega e Sousa Hospital, Penafiel, Portugal
ENDOSCOPIC MANAGEMENT OF KERATINIZING SQUAMOUS METAPLASIA OF THE BLADDER WITH URETERAL OBSTRUCTION
CYSTOSCPIC EXTRACTION OF A WHOLE PEN FROM THE BLADDER. A CASE REPORT
1) Source of work is Urology department at Tanta University Hospital.
2) No conflict of interest.
3) Author disclosure: No competing financial interests exist
(N.B) The video music was obtained from the website:
Song name: Dream Culture
ROBOTIC EXICION OF URACHAL REMNANTS AND UMBILLICOPLASTY; PRESENTATION OF OPERATIVE TECHNIQUE
THE RESECTION OF FIBROEPITHELIAL POLYP WITH HO:YAG LASER
Aksaray State Hospital, Aksaray, Ankara, Turkey
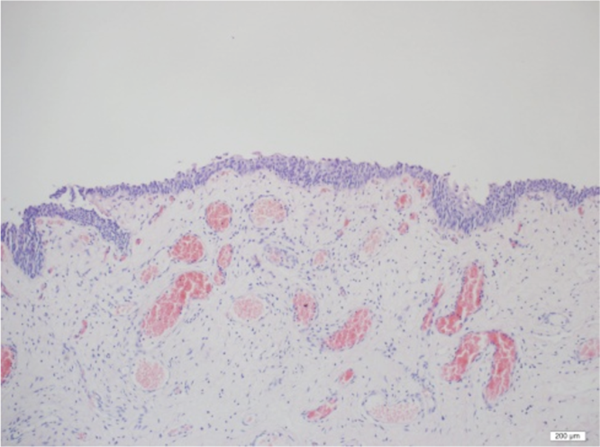
Fibroepithelial polyps of the urinary tract are rare, benign, non-epithelial tumors. They may involve the renal pelvis, ureter, bladder or urethra. They are composed of a stroma derived from mesoderm and covered by a layer of normal transitional epithelial cells. In contrast to tumors of epithelial origin, malignant degeneration of fibroepithelial polyps has not been reported. Fibroepithelial polyps can cause urinary obstruction with the most common presenting symptom.
We report a 30-year-old woman who presented to our clinic with left flank pain and urgency symptoms. Further examination included MRI urography and cystoscopy. Interestingly there was no filling defect and hydronephrosis at the MRI urography but there was a mass filling the ureteral orifice at the cystoscopy. After the cystoscopy ureteroscopy revealed a polypoid mass, which was floating up and down in the lumen of the ureter. The polyp was resected by Ho: Yag laser and extracted from the ureter. A double J stent was inserted and left for three weeks.
Histology verified a polyp containing a loose fibrous tissue with the presence of vessels. Ureteroscopy was performed following removal of the stent with findings of clear urothelium of ureter without any scaring. Her follow up is 6 months without any clinical symptoms.


Acibadem University, Urology Department, Istanbul, Turkey
EPISPADIAS REPAIR USING A TECHNIQUE OF MINIMAL MOBILIZATION AND CORPORAL ROTATION
POSTER PRESENTATIONS
POSTER SESSION 1: LOWER URINARY TRACT OBSTRUCTION - BPH AND URETHRAL STRICTURES, USE OF SMARTPHONES IN ENDOSCOPIC PROCEDURES
PRELIMINARY EXPERIENCE WITH A NEW TECHNIQUE FOR THE TREATMENT OF BENIGN PROSTATE HYPERPLASIA. TRANSURETHRAL ADENOMA ENUCLEATION IN SALINE BUTTON ELECTRODE (B-TUEP) WITH GYRUS PK SYSTEM
We evaluated our results with Transurethral Adenoma Enucleation with Button electrode (TUEP-B) in saline for the treatment of bladder outlet obstruction (BOO) due to benign prostatic hyperplasia (BPH).
Following surgery, we evaluated bladder irrigation's time, catheterization's time, RUA post B-TUEP, hospital's stay and any emergency after the surgery within 30 days.
The follow up was performed after one month from the surgical procedure and then at 3–6 and 12 months, with PSA and HB dosage, IPSS, IEFF-5, QOL, Uroflowmetry with PVR. TRUS was performed 6 months after surgery.
The bladder irrigation time was between 24 h and 36 h in about 80% (55 pts). No important change in pre and post operative Haemoglobin (p<0,1), no patient needed hemo transfusion.
In 5 pts we had haematuria and clot retention after catheter removal and only one pts was necessary a second look endoscopy. The hospitalization time was less than 48 hour in 22%, less than 72 hours in 70% and more in 18%.
In 6% of pts we had a new readmission in hospital for
We had no urinary incontinence. In the first 30 days we had 1 new admit to hospital for heamaturia. After six months we had 2 pts with urinary obstruction and in second time we permed a TUIP.
PLASMAKINETIC™ VAPORIZATION VS PLASMAKINETIC™ RESECTION FOR TREATMENT OF BENIGN PROSTATIC HYPERPLASIA: A PROSPECTIVE RANDOMIZED TRIAL WITH 1 YEAR FOLLOW UP
TRANSURETHRAL THULIUM LASER VAPO-ENUCLEATION VERSUS TRANSVESICAL OPEN ENUCLEATION FOR PROSTATE ADENOMA GREATER THAN 80 G: A STUDY OF 78 PATIENTS
Academic Dep. of Urology, University of Milan, Policlinico San Donato Milanese, Milan, Italy
Academic Dep. of Urology, University of Milan, Policlinico San Donato Milanese, Milan, Italy
Academic Dep. of Urology, University of Milan, Policlinico San Donato Milanese, Milan, Italy
Academic Dep. of Urology, University of Milan, Policlinico San Donato Milanese, Milan, Italy
Academic Dep. of Urology, University of Milan, Policlinico San Donato Milanese, Milan, Italy
THE MANAGEMENT OF THE URETHRAL STRICTURE - OUR EXPERIENCE
UCCK, Clinic of Urology, Prishtina, Kosovo
UMHAT “Alexandrovska”, Department of Urology, Sofia, Bulgaria
VIDEO ENDOSCOPIC TELECONFERENCING OF PHOTOGRAPHS TAKEN BY SMARTPHONES DURING INTRAOPERATIVE REFERRALS
POSTER SESSION 2: PROSTATE CANCER
PREDICTOR FACTORS OF SURVIVAL IN HORMONE-REFRACTORY PROSTATE CANCER PATIENTS
FIRST RESULTS COMPARING BETWEEN HAND-HELD ROBOTIC ASSISTED PROSTATECTOMY AN CONVENTIONAL RADICAL ENDOSCOPIC EXTRAPERITONEAL PROSTATECTOMY (KYMERAX, TERUMO)
Patients with PSA level >10 ng/ml underwent preoperative skeletal scintigraphy (bone-scan), abdominal computed tomography and Intraoperative express histology of pelvic lymphatic nodes. A nerve sparing procedure was carried out on patients with a Gleason score <7 and PSA level <10 ng/ml. With the aid of validated questionnaires, patients were asked about urinary incontinence complaints and erectile disorders after 3, 6, and 12 months from discharge.
In the second group we had 44 patients with T1-T2 R0, no patient had R1. 16 patients had T3, 7 patients had R1.
USING HIGH INTENSITY FOCUSSED ULTRASOUND AS A FOCAL THERAPY IN THE TREATMENT OF PROSTATE CANCER (HIFU)
EVALUATION OF PSA VALUES BEFORE, DURING AND AFTER PROSTAT BIOPSY IN PROSTATE CANCER
Necmettin Erbakan University Meram Medical Faculty Urology Department, Konya, Turkey
University Hospital “Lozenetz”, Department of Urology, Sofia, Bulgaria
The urine draining duration with urethral catheter is 5–25 days (Ø 6,5 days). An early post-operative complication occurred in 1 (5%) case - removal of the catheter by the patient himself on postoperative day 1 which resulted in extended wear of the catheter and subsequent urinary incontinence. We saw no hematoma or wound infections.
Cancer results: 19 (95%) patients were with cancer limited to the prostate (pT1a-pT2b). 1 (5%) patient was with a locally advanced prostate cancer pT3a, Gleason 8, N0, R1. The remaining patients had no positive surgical margins.
POSTER SESSION 3: RENAL PATHOLOGY
EVALUATION OF RENAL FUNCTION CHANGES AFTER RADICAL AND PARTIAL NEPHRECTOMY AT SINGLE INSTITUTION IN OTHERWISE HEALTHY INDIVIDUALS
Estimated Glomerular Filtration Rate (eGFR) in Group I and Group II
Statistical significant difference for p<0,05.
Statistical significant correlation for Pearson r→1.
TRANSPERITONEAL LAPAROSCOPIC NEPHRECTOMY FOR PYONEPHROTIC KIDNEYS
The nephrectomy was done outside Gerota fascia and specimens were removed without morcellation. The patients were assessed for operative time, peroperative and postoperative complications, conversion rate, and hospital stay.
The mean operating time was 170 minutes (range 110–240).
The mean hospital stay was 3.7 days (range 2–7).
LAPAROSCOPIC FENESTRATION OF LYMPHOCELE AFTER KIDNEY TRANSPLANTATION - FIRST LINE THERAPY? - 2 CASES FROM OUR PRACTICE
In the second case we performed a laparoscopic fenestration of the lymphocele initially.
RETROPERITONEOSCOPY: THE FIRST 100 CASES
Tamega e Sousa Hospital, Penafiel, Portugal
The aim of this work is to present our inicial experience in retroperitoneoscopy.
Nowadays open pyeloplasty is considered the procedure of choice for the treatment of stenosis of the pyeloureteral junction. However, in connection with the development of minimally invasive surgery in the treatment of UPJ strictures were applied endoscopic and laparoscopic techniques. The success of endoscopic procedures do not exceed 70 – 80%, while the success of laparoscopic technique comparable with open surgery.
Between 2007 and 2013 in our clinic performed 271 laparoscopic UPJ. Mean patient age was 43 years (18 – 71), including 159 women, 112 men. Pyeloplasty on the left side was performed in 154, on the right - in 117 people.
In our clinic with strictures associated with the presence of an additional vessel pyeloplasty was performed by Heinz- Andersen. Vertical plastics took place at 44.6% (121) of the cases, the horizontal - 26.6% (72). When UPJO associated with high discharge of the ureter was performed Y - V Foley plasty in 10.7% (29) people. In the presence of dysplasia upper ureter performed by plastic Culp-DeWeerd in 18.1% (49). Mean operative time was 135 min (90 – 320). Blood loss did not exceed 50 ml. In all cases, the upper urinary tract were drained JJ- stent mounted antegrade 86.3% (234) and the retrograde 13.7% (37). Antimicrobial therapy was administered broad-spectrum antibiotics for 40 minutes before surgery intravenously and orally until the urethral catheter was removed. Within 15 days of NSAID used. Drainage was removed on 2nd day after the operation. Urethral catheter was removed on 4e-7th postoperative day. Duration of hospital days averaged 7 (5–15). 6 weeks after surgery JJ-stent was removed. Control excretory urography was performed at 3 and 6 months after surgery.
We observed intraoperative complications: once wound intestines and omentum. In the early postoperative period in 16 (5.9%) patients developed acute pyelonephritis, uroplania detected in 9 (3.3%) patients, urinary leakage drainage - 13 (4.8%) patients, bleeding on drainage developed at one person 0.37%. In the late postoperative period 32 (11.8%) patients had acute pyelonephritis, relapse of UPJ strictures occurred in 11 (5.6%) patients.
Reasons for failure of laparoscopic pyeloplasty in our opinion is the use for hemostasis in the area of UPJ monopolar, current wide selection of ureter, pelvis and ureter dissection using “hot” scissors, very frequent anastomotic sutures, the tension of the ureter, ureteral torsion, prolonged exposure of the drainage in the area of the anastomosis, chronic infection, prolonged exposure JJ- stent.
Laparoscopic pyeloplasty is a minimally invasive procedure that provides a persistent clinical and radiographic results similar to those of open pyeloplasty. While remaining technically complex procedure, laparoscopic pyeloplasty able to eliminate all possible causes of UPJO with minimal risk of bleeding complications. In experienced hands, laparoscopic pyeloplasty is an effective, minimally invasive method of treatment, applicable in most patients with UPJ strictures.
LONG-TERM OUTCOME FOR TREATMENT OF SIMPLE SYMPTOMATIC RENAL CYSTS WITH PERCUTANEOUS ALCOHOL SCLEROTHERAPY
Source of Funding: none
Results following Ultrasound guided drainage of cortical cysts.
Total 236
Males 157
Females 79
Mean follow up (Months) 25,1 (sd:7,2)
Cyst size (mm in CT) 57.8 (sd: 23,7)
Immediate complications (%), (N) 9.32% (22)
Late complications 0
Recurrence (%), (N) 10.59% (25)
New cyst Occurrence (%), (N) 4.23% (10)
Need for further intervention (%), (N) 14.83% (85)
Improvement in pain / Discomfort (%), (N) 83.89% (198)
Improvement in BP (%), (N) 15.68% (37)
RESULTS OF RETROPERITONEOSCOPIC CYSTECTOMY FOR RENAL CYSTIC DISEASE
Characteristics of Patients
POSTER 4: UROTHELIAL CANCER
PURE INTRACORPOREAL LAPAROSCOPIC RADICAL CYSTECTOMY WITH ORTHOTOPIC “U”- SHAPED ILEAL NEOBLADDER
DOES NBI CYSTOSCOPY INCREASE THE DETECTION RATE OF NON-MUSCLE INVASIVE BLADDER NEOPLASMS? SINGLE CENTRE EXPERIENCE
The purpose of this study was to evaluate how the use of preoperative NBI cystoscopy in respect to WL cystoscopy, related to pT and the grading after TURBT, increases our predictive power of identifying non-muscle invasive bladder lesions.
Indication about use of TURBt was performed in agreement to the EAU Guideline 2010. The characterization of the sites, including the number, size and appearance of the neoplasms, were recorded on a topographic bladder map. Before we performed a cystoscopy with white light and after with NBI light. All endoscopic resections were performed with an Gyrus PK scalpel, bipolar generator (Olympus, Tokyo, Japan). Resection of each lesion was carried out with white light, whilst a resection of surgical margins was performed along with the bed of surgical resection using only NBI light, which was sent separately with a sequence number identifying them. All histopathological evaluations were performed by a single pathologist based on the 2004 WHO classification.
The follow-up was performed in according to the EAU Guide lines 2010. During the follow-up, all procedures were always performed by the same urologists who had performed the initial TURBT, after the initial assessment of the topographic map where they were shown the location of the tumours detected in white light or in NBI light.
In the positive oncological specimens before WL TURBT group, we observed an overall suspicious bladder lesions detection rate by 64,24% (512 pts), with an overall increased NBI suspicious bladder lesions, visible lesions only before NBI cystoscopies, detection rate by 12,42% (99 pts.) and an overall false positive rate by 11,91% (95 pts).
About to
About to
DIAGNOSTIC ACCURACY OF TRANSRECTAL AND TRANSVAGINAL ULTRASONOGRAPHY FOR SUPERFICIAL BLADDER CANCER
OUR EXPERIENCE IN THE TREATING WITH TURBT THE PATIENTS WITH INFILTRATIVE TUMORS AT STAGING T3a and T3b
University Clinical Center of Kosovo, Urology Department, Prishtina, Kosova
There was no significant difference in recurrence-free survival between groups (not on statin mean 75.3 months, on statin 50.2 months; log rank p=0.26).
NON-INVASIVE PAPILLARY UROTHELIAL CARCINOMAS OF THE UPPER URINARY TRACT – ENDOSCOPIC TREATMENT BY ELECTROABLATION
Medical University, Plovdiv, Bulgaria
We matched a ureterorenoscopy with therapeutic ablation by 7,5 Ch semirigid ureteroscope (Figure 2, tumor with electrode).
In patients with pelvic kidney tumors lesions were in accessible places for treatment. Before destruction of tumors we always take a biopsy. Ablation was done by Hulbert ball tip electrode (115 cm, 3 Ch insulated conductors connected with high-frequency generator, which is on Figure 3).
In 2 cases, the controlling ureterorenoscopy proves tumor relapses in 6 months after the 1st intervention. Local tumor control was achieved by conducting a second ablation. These patients, 9 and 12 months after the secondary intervention showed no signs of local recurrence. In the follow-up period, the control instrumental examinations (cystoscopy, ureteroscopy) and cytology test of urine have all been negative in terms of carcinoma in remaining 8 patients. Figure 4 illustrates the oncologycal results since 2012.
The studied group with all the patients.

Tumour electro ablation by electrode.

Hulber ball tip electrode by which we do electroablation.

Oncological results in the followup period.
Indication of suitability for TURBt was provided on the basis of the EAU Guideline 2010. All patients provided written informed consent prior to the study. All procedures were carried out initially by performing a cystoscopy with white light. The characterization of the sites, including the number, size and appearance of the neoplasms, were recorded on a topographic bladder map. At this a cystoscopy with NBI was carried out to confirm what had been seen in the white light examination, and to report suspicious areas with NBI light. These, too, were recorded on the topographic bladder map. All endoscopic resections were performed with a Gyrus PK scalpel, bipolar generator (Olympus, Tokyo, Japan). Resection of each lesion was carried out with white light, whilst a resection of surgical margins was performed along with the bed of surgical resection using only NBI light, which was sent separately with a sequence number identifying them. All histopathological evaluations were performed by a single pathologist based on the 2004 WHO classification.
The follow-up was performed in according to the EAU Guide lines 2010.
In our experience, using NBI cystoscopy significantly increased our predictive power to find out lesions not visible with WL cystoscopy, both unifocal (p<0,0001), and <3 cm (p<0,0001), and primitive (p<0,02).
HOW CAN THE USE OF NBI CYSTOSCOPY INCREASES THE ABILITY TO IDENTIFY NON-MUSCLE INVASIVE BLADDER CANCER? - PRELIMINARY EXPERIENCE IN A SINGLE CENTRE
Indication of suitability for TURBt was provided on the basis of the EAU Guideline 2010. All patients provided written informed consent prior to the study. All procedures were carried out initially by performing a cystoscopy with white light. The characterization of the sites, including the number, size and appearance of the neoplasms, were recorded on a topographic bladder map. At this a cystoscopy with NBI was carried out to confirm what had been seen in the white light examination, and to report suspicious areas with NBI light. These, too, were recorded on the topographic bladder map. All endoscopic resections were performed with an Gyrus PK scalpel, bipolar generator (Olympus, Tokyo, Japan). All histopathological evaluations were performed by a single pathologist based on the 2004 WHO classification.
In all, 512 patients (64,24%) had bladder tumour, 402 (50,4%) were detected both with WL and NBI and 99 (12,42%) only with NBI Cystoscopy.
Overall false positive detection rate was 35,75% (285 pts.).
The use of WL and NBI cystoscopy permit to have a sensibility of 80,66% and of 97,85% with PPV of 68,49% and of 63,74%, respectively. On accuracy we observed a 63,74% and 62,86% respectively.
IS OUR ENDOSCOPIC RESECTION TECHNIQUE CORRECT? DOES THE USE OF NBI, AFTER WLTURB, CAN INCREASED OUR ABILITY TO DETECT PERSISTENT DISEASE? A SINGLE CENTRE PRELIMINARY EXPERIENCE
Indication of suitability for TURBt was provided on the basis of the EAU Guideline 2010. All patients provided written informed consent prior to the study. All procedures were carried out initially by performing a cystoscopy with white light. The characterization of the sites, including the number, size and appearance of the neoplasms, were recorded on a topographic bladder map. At this a cystoscopy with NBI was carried out to confirm what had been seen in the white light examination, and to report suspicious areas with NBI light. These, too, were recorded on the topographic bladder map. All endoscopic resections were performed with an Gyrus PK scalpel, bipolar generator (Olympus, Tokyo, Japan). Resection of each lesion was carried out with white light, whilst a resection of surgical margins was performed along with the bed of surgical resection using only NBI light, which was sent separately with a sequence number identifying them.
All histopathological evaluations were performed by a single pathologist based on the 2004 WHO classification.
For each patient treated with WLTURBt, we have after resected both the margins and the bottom using NBI, finding the presence of 521 neoplastic lesions, 33,1% demonstration of persistent disease. In the following table we can see the distribution respect NBI cistoscopy.
The group with persistent disease both on margins and bottom was the more represented, 41,03%.
HOLMIUM YAG LASER EN-BLOC RESECTION OF PRIMARY SUPERFICIAL BLADDER CANCER. A SINGLE CENTER EXPERIENCE
A NEW METHOD FOR THE DIAGNOSIS OF THE INTRAPERITONEAL BLADDER RUPTURE: FLUORESCEIN
POSTER 5: UROLITHIASIS
FACTORS THAT AFFECTING THE SUCCESS OF RETROGRADE INTRARENAL SURGERY
IS RETROGRADE URETEROSCOPIC INTRARENAL SURGERY (RIRS) A GOOD AND EFFECTIVE TREATMENT IN PATIENTS WITH RENAL AND UPPER URETERIC STONE UNTIL 4.3 CM?
Flexible ureteroscopes allows a variety of procedures like treatment of kidney stones, renal pelvic tumors and calyceal diverticulum's. It's possible with many accesories instruments like, tipless nitinol baskets, wire, thinner hydrophilic coated kink resistant access sheath, Holmium laser with thinner fibers (200 micron) to access lower calyx without affecting the deflection of the flexible scope.
The percutaneous nephrostolithotripsy (PCNL) is a gold standard procedure for large kidney stones, and also has certain limitations in patients with bleeding diathesis, [1] obesity and malrotated kidneys.
Retrograde ureteroscopic intrarenal surgery (RIRS) is a less morbid procedure than PCNL, less hospitalization'time and better compliance for the patients.
So, we have evaluated the feasibility of RIRS as a viable alternate to PCNL in treating patients with renal and upper ureteric calculus of 2 cm to 4.3 cm stone burden, the cases which are usually taken up for PCNL otherwise.
From 2011 to genuary 2014, a total of 36 cases of upper ureteric and renal stone of 2 cm to 4.3 cm stone burden for which PCNL would be done otherwise were treated by RIRS.
We do not routinely pre stent the patient. The largest fragment was basketed out to assess the size.
Several techniques can be applied to improve the fragmentation minimize the need for re-look surgery. The major time consuming maneuver in RIRS is trying to fragment the stone in lower or middle calyx. This can be overcome by repositioning the stone in a favorable upper calyx. This will help the flexible scope to be straight during fragmentation process and avoids strain on the deflection mechanism and the risk of laser fiber damaging the scope.
This study was not done in a randomized way and did not have a control group. The follow-up for residual fragments was done with ultrasound and X-ray KUB.
The stone free rate in RIRS is 82.6% in first sitting, 97.2% and 100% in thirth sitting.
PCNL was the only option to treat large upper ureteric/renal stones before the introduction of RIRS. RIRS is superior in terms of less complication, less morbidity and good stone free rate and has an advantage of one day of hospital stay and resuming duties after two days. RIRS is, for us, a viable alternate for PCNL for upper tract stones up to 4.3 cm.
THE EFFICACY OF PERITUBAL ANALGESIC INFILTRATION IN POSTOPERATIVE PAIN FOLLOWING PERCUTANEOUS NEPHROLITHOTOMY – A PROSPECTIVE RANDOMIZED CONTROLLED STUDY
LOW-COST TREATMENT OF URETERAL STONES: A SINGLE HIGH FLOW CENTER EXPERIENCE
Urolithiasis is a common and costly disease. URS is the most commonly advocated treatment for patients with ureteral calculi with a stone-free rate higher than 90% after a single treatment. In 2007 the EAU Guideline recommended that for ureteral stones requiring removal, because up to 98% of ureteral calculi <5 mm in diameter are likely to pass spontaneously, both SWL and URS are acceptable first-line treatments in healthy non-pregnant adults who have unilateral calculi.
Complete clearance was considered if there were no fragments on USG screening after three weeks. The stone free rate in RIRS is 86.6% in the first sitting and 100% at second sitting.
Between July 2004 and January 2014, we evaluated medical data related to semirigid ureteral ureteroscopy (URS) with ureterolithotripsy using a Holmiun laser performed in our centre The aim of this study was to demonstrate how, in a center such as ours with high patient numbers, it is possible to perform a ureterolithotripsy for ureteral stones using a minimum set of instruments to complete the treatment.
With the development of smaller caliber ureteroscopes and the introduction of improved instrumentation, including the holmium:YAG laser, ureteroscopy has evolved into a safer, more effective method of treating ureteral stones.
The use of holmium laser lithotripsy is a safe and effective means of treating ureteral stones regardless of sex, age, stone location, or stone size. Complications were uncommon. The instrumentation we used was extremely limited, in order to reduce costs related to the procedure to an absolute minimum whilst maintaining the two quality indicators for the procedure, namely success-rate and length of hospitalisation (86.1% and 34 hours), which reflect those obtained with other experiences.
FLEXIBLE URETERORENOSCOPY VERSUS SHOCK WAVE LITHOTRIPSY FOR THE TREATMENT OF UPPER/MIDDLE CALYX KIDNEY STONES OF 10–20 MM: A RETROSPECTIVE ANALYSIS OF 174 PATIENTS
FLEXIBLE URETERORENOSCOPY VS SEMIRIGID URETEROSCOPY FOR THE TREATMENT OF PROXIMAL URETERAL STONES: A RETROSPECTIVE ANALYSIS OF 124 PATIENTS
LEAVING FRAGMENTS IN SITU AFTER URETEREOSCOPY: FEASIBILITY AND OUTCOMES
Department of Urology, Military Hospital Avicenne, Marrakech, Morocco
In 208 ureteral stones fragments were removed using forceps (group A). In 172 patients fragments (<4 mm) were left in situ for spontaneous passage (group B). Patients were followed clinically and with radiography for 3 months.
Procedure duration, peroperative complications, analgesic use, hospitalization, adjuvant procedures, and stone-free rates were recorded and compared retrospectively.
The mean operative times for groups A and B were 38.±6.4 and 31.2±7.1 minutes, respectively (p<.001). Mucosal injury due to forceps or basket use was observed in 11.2% in group A and 2.2% of the patients in groups 8 (p<.001). One case of ureteral stripping was noted in group A.
Further oral or intramuscular analgesia was required in 28% and 49% of the patients in group A en B respectively during the week following procedure.
The percentage of patients requiring adjuvant procedure was higher in group B but difference was not significant (p=0.06). Stone-free rates and were similar between the 2 groups.
Department of Urology, Military Hospital Avicenne, Marrakech, Morocco
Characteristics of patients and stones, peroperative and postoperative data, stone free rate were retrospectively collected and reviewed.
No statistically significant differences in terms of blood transfusion, fever, and prolonged urinary leakage were detected in all groups. Postoperative hospital stay and paralytic ileus rates were significantly higher in group A (p<0.05). The stone-free rates in groups A, B, and C, at discharge were 97%, 68% and 64% and 76%, 90% and 86%, respectively (p<0.05).
METAL TELESCOPIC DILATION IN PERCUTANEOUS NEPHROLITHOTOMY: A SINGLE-CENTER EXPERIENCE
URETEROSCOPIC LITHOTRIPSY AS E BEST TREATMENT FOR THE MIDDLE AND LOWER PARTS OF URETEROLITHIASIS
University Clinical Center of Kosovo, Urology Department, Prishtina, Kosova
USE OF NTrap® DURING URETEROSCOPIC LITHOTRIPSY FOR UPPER URETERAL STONES
National Police Hospital, Korea Republic
MINIMALLY INVASIVE PERCUTANEOUS NEPHROLITHOTOMY IN CHILDREN: EXPERIENCE FROM THE UK
COMPARISON OF STANDARD AND TOTALLY TUBELESS PERCUTANEOUS NEPHROLITHOTOMY APPROACHES ACCORDING TO MODIFIED CLAVIEN COMPLICATION GRADING
Department of Urology, Diskapi Yildirim Beyazit Training and Research, Ankara, Turkey
LAPAROSCOPIC PYELOLITHOTOMY IN HORSESHOE KIDNEY
14:00-15:00 POSTER 6: VARIOUS POSTER 6: VARIOUS
ASYMMETRIC DIMETHYL ARGININE LEVELS IN TESTICULAR TISSUE AND BLOOD OF RATS WITH INDUCED EXPERIMENTAL VARICOCELE
CLINICAL SIGNIFICANCE OF SPERM MOTILITY
The
DETERMINATION OF GENITAL HYGIENE BEHAVIOURS IN WOMEN WITH CYSTITIS
School of Nursing, Gulhane Military Medical Academy
Department of Urology, Charité University Hospitals, Berlin, Germany
Using this robust reusable tunnelling device to position the mesh and an improved knotting technique, we were able to perform laparoscopic sacrocolpopexies that were technically optimised with respect to reduction in operating time, savings in materials used, and minimisation of risk, together with optimal postoperative mesh positioning confirmed by MRI. The instrument can be used again promptly after simple cleaning and sterilisation, with virtually no effect on costs.
The results of 21 laparoscopic sacrocolpopexies performed with this instrument confirmed these advantages.
Stress Urinary Incontinence (SUI) is a condition of social dimension which generally pertains to women of various age. The only effective treatments of SUI are surgical procedures. The use of ‘tension free trans-vaginal tape’ (TVT) insures a minimal invasive procedure, but also carries potential complications from long term effects. One of these complications may be the migration of thread, or tape, into the urinary bladder creating conditions for urinary stones (cystolithasis). There are a number of treatment methods for cystolithasis, among them optical lithotripter, ultrasound and pneumatic probes, and recently, the holmium laser.