
Abstract
Purpose:
To validate the effect of listening to music on perceived anxiety and pain during office-based flexible cystoscopy using the State-Trait Anxiety Inventory (STAI) and the Visual Analog Scale (VAS), in a well-matched North American veteran patient population in a prospective, randomized fashion.
Patients and Methods:
A total of 137 veteran patients receiving routine urologic care in a North American Veterans Affairs (VA) healthcare system were recruited over a 2-year period (June 2011 to June 2013). All patients were prospectively randomized to undergo office-based flexible cystoscopy with or without music. The music group consisted of 73 patients who listened to the same excerpt of classical music at the time of flexible cystoscopy; the nonmusic group consisted of 64 patients.
Results:
The median postprocedural STAI anxiety scores between the music and nonmusic groups were statistically significantly different: 30 (range 23–39) and 35 (range 28–49), respectively (P=0.0017). The median postprocedural pain VAS score between the music and nonmusic groups reached statistical significance: 0 (range 0–1) and 2 (range 1–2), respectively (P<0.0001). The median delta STAI anxiety score was statistically significantly different between the music and nonmusic groups: 0 (range −3–0) and 2 (range 0–4), respectively (P<0.0001).
Conclusions:
This study demonstrates that listening to music decreases anxiety and pain associated with flexible cystoscopy in a North American VA patient population. We recommend incorporating music as an effective adjunct to other maneuvers used at the time of flexible cystoscopy to reduce anxiety and pain.
Introduction
F
Music has gained increasing recognition as an effective tool to alleviate perceived pain and has been shown to be beneficial in a variety of clinical settings. 8 –14 Recent publication shows that patient-preferred music reduced anxiety during cystoscopy. 15 Although patient-preferred music may not be feasible, even in a very basic clinical setting, usually some music can be played during the procedure, and it will be a simple and cheap method to decrease patient anxiety and pain.
The State-Trait Anxiety Inventory (STAI) and the Visual Analog Scale (VAS) are well validated surveys that are often used to assess anxiety and/or pain. 8,9 STAI scores range from 20 to 80; STAI measures the transitional emotional status evoked by a stressful situation, such as a medical procedure or surgery. The VAS scores range from 0 to 10, which quantifies the pain level using verbal and visual descriptors. We sought to validate the effect of listening to nonpatient-preferred music on perceived anxiety and pain during office-based flexible cystoscopy using the STAI and VAS, in a well-matched North American veteran patient population in a prospective randomized fashion.
Patients and Methods
In this Institutional Review Board-approved study, a total of 137 patients were prospectively randomized to undergo office-based flexible cystoscopy with or without music over a 2-year period (June 2011 to June 2013). All patients recruited for this study were veterans who received routine urologic care and follow-ups at the Veterans Affairs (VA) San Diego Healthcare System (San Diego, CA). Patient privacy and confidentiality are protected according to the Health Insurance Portability and Accountability Act guidelines as per the VA guidelines and policies. A biased-coin randomization method was performed.
The music group consisted of 73 patients and the no-music group consisted of 64 patients. In the music group, patients listened to the same excerpt of classical music at the time of flexible cystoscopy; no music was played at the time of flexible cystoscopy in the nonmusic group. Inclusion criteria were patients who were >18 years old. Exclusion criteria were current urinary tract infection, anatomic urethral abnormalities, any analgesic use during the 24 hours before flexible cystoscopy, and inability to complete the surveys. Patients' medical history, including history of bladder cancer, prostate cancer, gross or microscopic hematuria, and current or past use of antidepressants and antianxiety medication, were all recorded.
All patients with a history of bladder cancer were confirmed to have had previous flexible cystoscopy and were currently undergoing flexible cystoscopy for surveillance, while those without bladder cancer were undergoing flexible cystoscopy for diagnostic purposes (e.g., gross or microscopic hematuria). Each patient consented for the study on the day of the procedure.
Preoperative and postoperative systolic and diastolic blood pressures and heart rates were measured for each patient. These physiologic parameters of vital signs were all obtained before flexible cystoscopy and before playing music; the postprocedure vital signs were obtained after the flexible cystoscopy was completed. Before each flexible cystoscopic examination, for the male patients in the study the penis was disinfected with povidone-iodine solution, and 10 mL of 2% lidocaine jelly was instilled intraurethrally. The lidocaine jelly was maintained for 15 minutes using an occlusive penile clamp at the tip of the penis that was fastened immediately after lidocaine injection. During the 15-minute dwell time of the 2% intraurethral lidocaine jelly and flexible cystoscopy procedure, the patient either listened to classical music for 15 to 20 minutes or did not hear any music at all.
Patients were placed in a specialized semirecumbent cystoscopy chair, and no additional manipulations were performed at the time of flexible cystoscopy (stent removal or bladder biopsy). All procedures were performed at the specialized cystoscopy suite at our institution by urology residents (postgraduate year 1 and 2). All patients viewed their procedures on a video monitor during the procedure, and the urology resident briefly mentioned each step in the process as it was being performed (instillation of analgesic, insertion of scope, and intravesical scoping). A 15F Olympus® flexible digital chip CYF-5 cystoscope (Olympus America Inc., Center Valley, PA) was connected to a digital video monitor that was used for all procedures.
The primary end point of this study was to measure anxiety and pain levels during office-based flexible cystoscopy with or without listening to music. We used the STAI and VAS, respectively, and higher scores indicate higher anxiety and pain for both tests. The patients were asked to complete two STAI anxiety surveys, one preprocedure and one postprocedure. Patients were also asked to complete a VAS survey postprocedure.
Statistics were generated and compared using an independent t test and chi-square tests. P values <0.05 were considered statistically significant. Delta anxiety score is defined as precystoscopy anxiety score minus postcystoscopy anxiety score.
Results
One hundred and thirty-seven patients were prospectively randomized into either the music group (n=73) or the nonmusic group (n=64). Table 1 outlines patient demographics and clinical characteristics for both groups. Patient enrollment, randomization, and analyses are presented in a Consolidated Standards of Reporting Trials flow diagram below (Fig. 1). There were no statistically significant differences in mean age, sex, or race. In addition, there were no statistically significant differences in history of bladder cancer, prostate cancer, hematuria, or use of antianxiety or antidepressant medications. The mean age was 65.8 and 67.1 years for men in the music and nonmusic groups, respectively. The majority of patients recruited for this study were men, 70/73 (96%) patients and 59/64 (92%) patients, respectively, while women constituted 3/73 (4%) patients and 5/64 8%) patients, respectively. The majority of the patients in each group self-identified as Caucasians, 56/73 (77%) patients and 47/64 (73%) patients in the music and nonmusic groups, respectively.
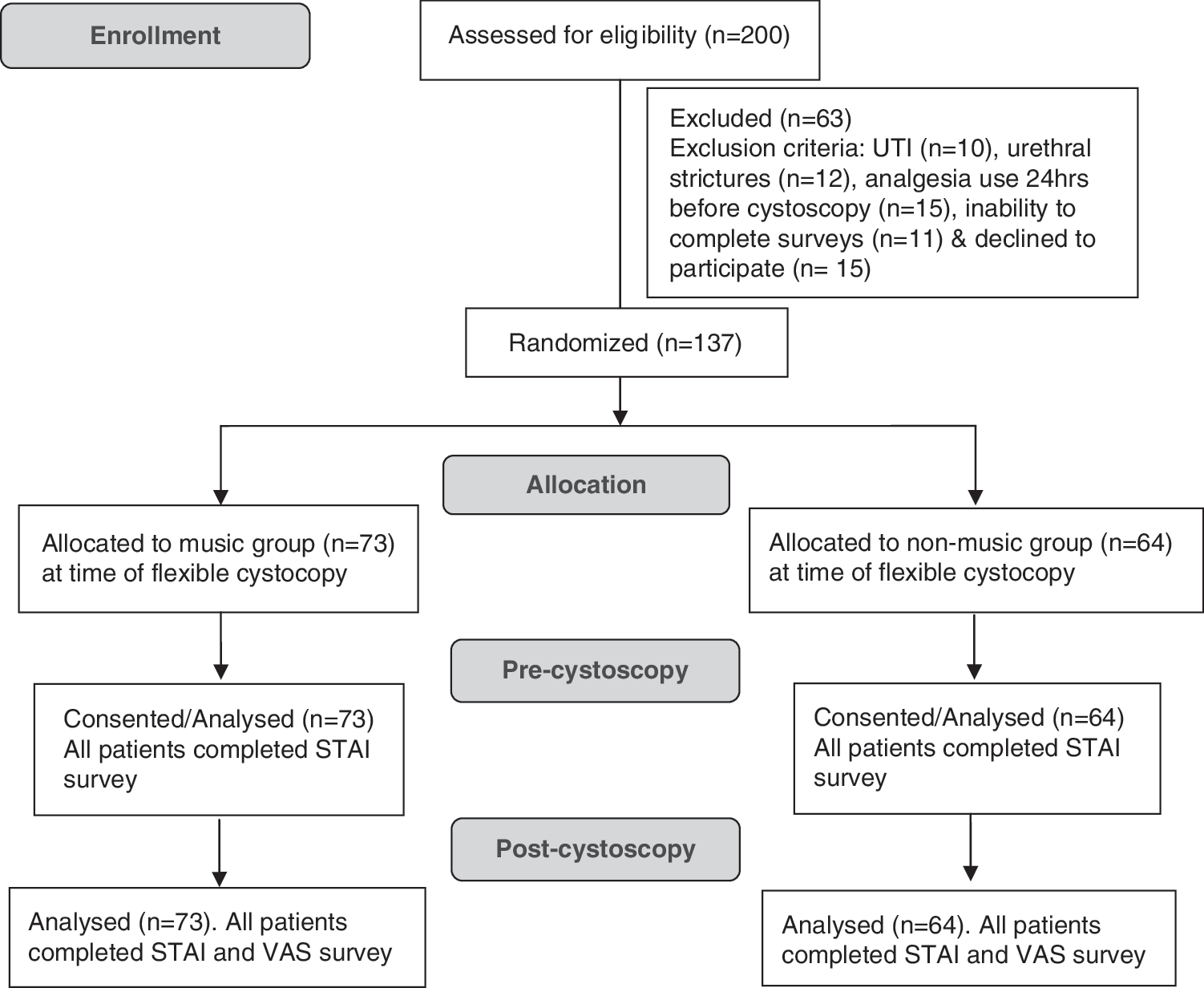
Flow diagram. UTI=urinary tract infection; STAI=State-Trait Anxiety Inventory; VAS=Visual Analog Scale.
SD=standard deviation.
More patients underwent surveillance flexible cystoscopy for a history of bladder carcinoma in the nonmusic groups, 24/64 (38%) patients, compared with 19/73 (26%) patients in the music group. Likewise, there were more patients with a history of prostate carcinoma who underwent flexible cystoscopy in the nonmusic group, 16/64 (25%) patients, compared with 13/73 (18%) patients in the music group. A history of hematuria (microscopic or gross hematuria) was an indication for flexible cystoscopy, which was performed in 41/73 (56%) patients and 29/64 (45%) patients in the music and nonmusic groups, respectively. In each group, 13 patients took antidepressant or antianxiety medications, 18% and 20% in the music and nonmusic groups, respectively.
The median anxiety level of music group patients was statistically less than that of nonmusic group patients. The median postprocedural STAI anxiety scores between the music and nonmusic groups were 30 (range 23–39) and 35 (range 28–49), respectively (P=0.0017) (Fig. 2). The median delta STAI anxiety score (precystoscopy anxiety score – postcystoscopy anxiety score) was also statistically significantly different between the music and nonmusic groups: 0 (range −3–0) and 2 (range 0–4), respectively (P<0.0001). Periprocedural physiologic parameters that correlated to anxiety and pain (systolic blood pressure, diastolic blood pressure, and heart rate) were not statistically different in both groups before and after flexible cystoscopy. Likewise, the median postprocedural pain scores, measured by VAS between the music and nonmusic groups reached statistical significance: 0 (range 0–1) and 2 (range 1–2), respectively (P<0.0001) (Fig. 3). Table 2 summarizes patient periprocedural physiologic parameters and compares the anxiety and pain scores between the music and nonmusic groups.
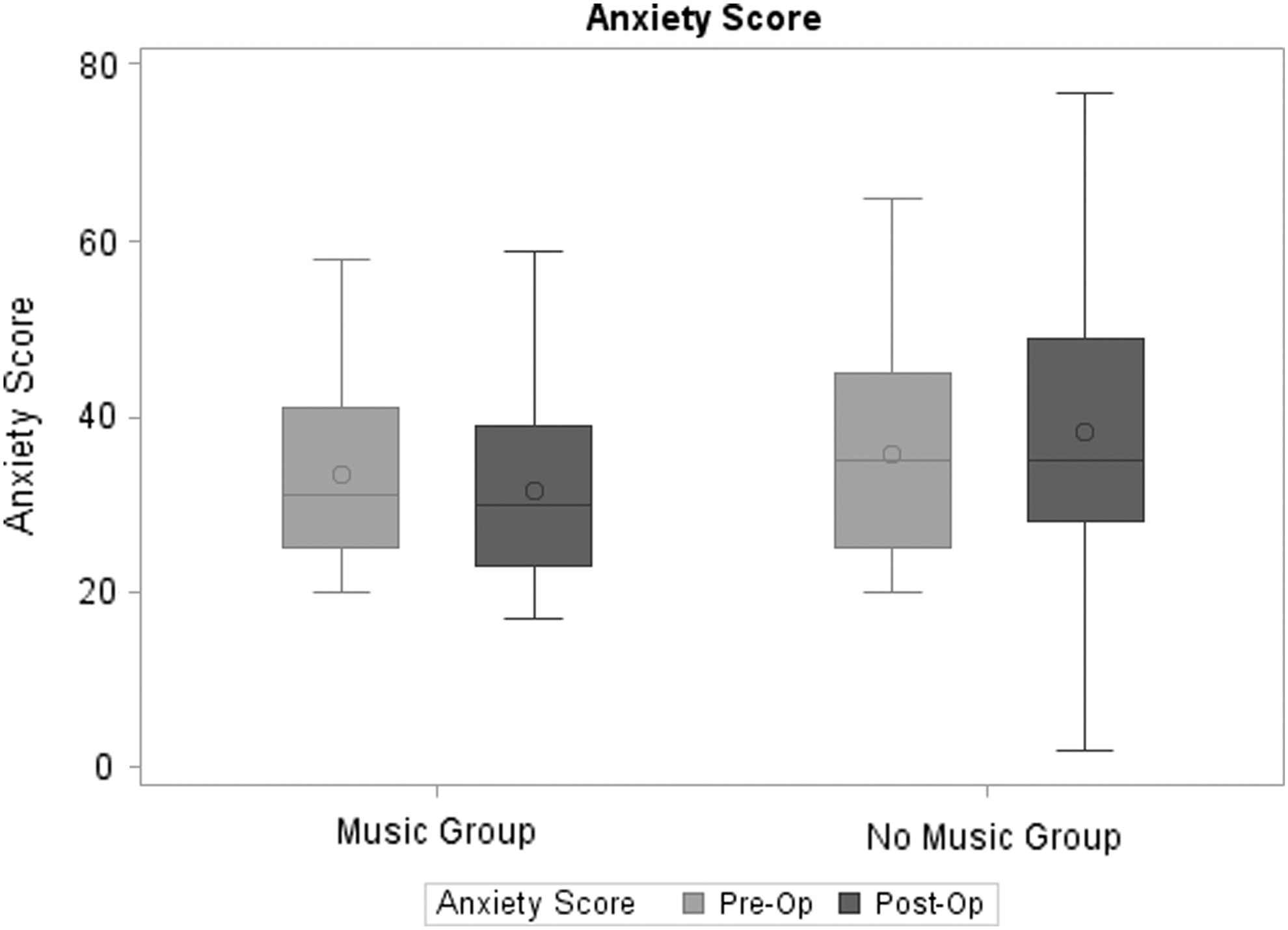
Periprocedural anxiety score as measured by the STAI between the music and nonmusic groups. Pre-op=preoperative; post-op=postoperative.
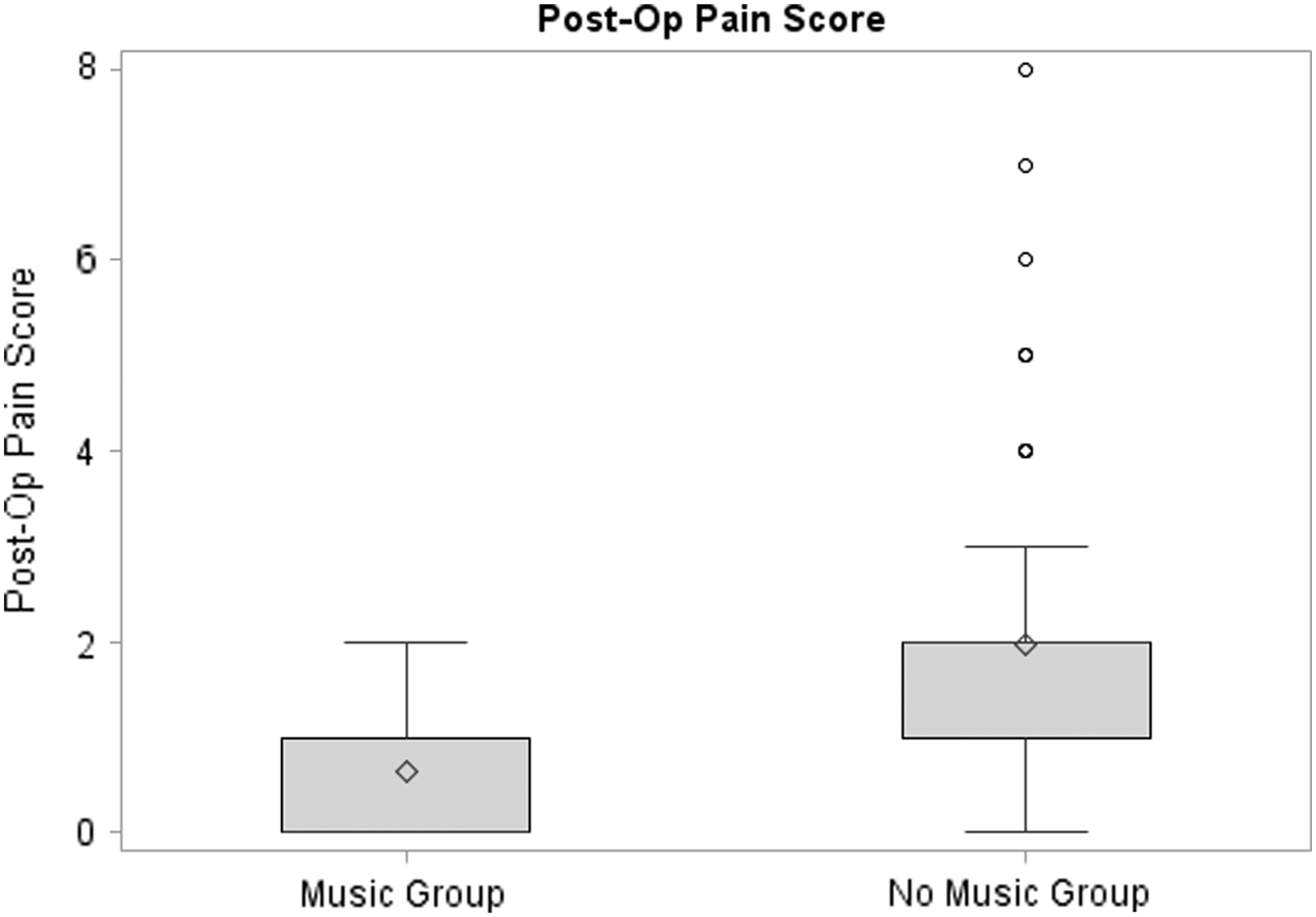
Postprocedural pain score as measured by the VAS between the music and nonmusic groups.
STAI=State-Trait Anxiety Inventory; IQR=interquartile range; VAS, Visual Analog Scale; Delta anxiety score=postanxiety minus preanxiety score.
Discussion
Over the last decade, various pharmacologic, environmental, and technologic advances have been adapted to reduce anxiety and pain associated with undergoing cystoscopy. 10 –21 None of these approaches, however, has proved to be sufficient to relieve anxiety and pain in patients during the procedure.
The majority of office-based cystoscopic procedures in the United States use flexible cystoscopes. Although fiberoptic technology is still used for many of the flexible cystoscopes in the country, digital technologies are available, allowing for enhanced visualization, higher resolution, decreased distortion, improved color representation, and larger image size compared with the standard fiberoptic visualization. 5 More recently, digital technology with distal sensor high definition images has been compared with standard digital visualization. Lusch and associates 5 demonstrated that the high definition digital flexible cystoscope has a higher resolution than the standard digital flexible cystoscope.
Although better visualization using the digital devices has not been correlated directly to patient comfort, one can hypothesize that it can reduce the time of the procedure, device manipulation, and secondary procedures, such as concomitant biopsies. These improved features of the digital flexible cystoscopy will likely result in improved patient comfort during office-based flexible cystoscopy procedures.
Environmental modifications, such as video monitoring by patients at the time of flexible cystoscopy, have been considered. 22 In a randomized study of 100 men undergoing standard office-based digital flexible cystoscopy conducted by Patel and colleagues 22 at the Cleveland Clinic, the study demonstrated that men viewing cystoscopy on the video monitor experienced an approximately 40% decrease in the pain level compared with those who did not view the procedure on the monitor. The study by Patel and colleagues 22 encouraged office urologists to incorporate this useful technique during flexible cystoscopy.
An additional environmental modification, such as periprocedural music, has gained increasing recognition as an effective tool to alleviate perceived pain and has been shown to be beneficial in a variety of clinical settings including burns rehabilitation, hospice palliative care, during colonoscopy, laceration repair, as well as prostate biopsies. 23 –28 For instance, Lee and coworkers 25 conducted a prospective randomized trial to examine the role of relaxing music in decreasing the dose of sedative medication needed for colonoscopy, measured by using the VAS scales and vital signs monitoring. In the study by Lee and coworkers, 25 a cohort of 165 patients scheduled to undergo elective colonoscopy were randomized into three different groups: Group 1 consisted of a combination of music and sedation, group 2 consisted of sedation alone, and group 3 consisted of music alone.
Results of this study demonstrated that group 1 patients were willing to repeat the same mode of sedation when queried immediately after colonoscopy (87%) and 24 hours later (75%), which was significantly different from the corresponding results in the other two groups (P=0.04 and P<0.01, respectively) and concluded that music can decrease the dose of sedative medication needed for colonoscopy and the combination of music and patient-controlled sedation was the best-accepted mode of sedation among the three groups.
Likewise, the urology literature has recognized this beneficial association between listening to music at the time of cystoscopy as evidenced by two recently published randomized studies from Far Eastern institutions. These two randomized studies suggest that listening to music during flexible or rigid cystoscopy enhances patient comfort and ameliorates postprocedure anxiety and pain. 29,30
It is well known that listening to music reduces perceptions of discomfort by activating the cingulofrontal cortex, which functions in attention shifting and pain modulation. Clinical reports suggest that music improves psychological and physiologic parameters. Music also has anxiolytic effects and has been applied to ameliorate stressful interventions. During laceration repair, for instance, the incorporation of music decreased pain and allowed for reduced doses of co-administered sedatives and analgesics. 26
In this study, we did not choose patient-preferred music. Some urology settings may not allow this luxury. Our study included periprocedural physiologic parameters such as blood pressure and heart rate as objective representations of the emotional state of the patient in addition to validated anxiety and pain questionnaires. These parameters are directly influenced by sympathetic nervous system activation from emotional distress or anxiety through the release of catecholamines, specifically norepinephrine and epinephrine. Higher catecholamine levels from anxiety and fear result in elevated blood pressure and heart rate. Thus, the combination of these objective physiologic indicators with the subjective patient-provided information on anxiety and pain provided a more holistic assessment of the impact of music on how a patient experiences flexible cystoscopy.
Importantly, this current study observed a significant decrease in the postprocedural anxiety and pain in the patients who listened to music during office-based flexible cystoscopy (Table 2, Figs. 2 and 3). Our results are consistent with previously published reports that music increases patient satisfaction and improves patient comfort while also reducing anxiety. 29,30 Subsets of patients with a history of bladder carcinoma that necessitated repeated surveillance office-based flexible cystoscopies were also included in this cohort. We observed that listening to music at the time of respective cystoscopy did not influence their periprocedural STAI anxiety scores when adjusting for other variables.
It is noteworthy that this study was conducted on patients at a VA hospital who have an increased prevalence of posttraumatic stress disorder and generalized anxiety disorder. Despite this, our results indicate significant reduction in the postprocedural anxiety and pain in veteran patients who listened to music during office-based flexible cystoscopy. To our knowledge, this is the first study to systematically demonstrate reduced anxiety and pain after flexible cystoscopy, as well as validate previously published reports from Far Eastern institutions, using validated questionnaires in a well-matched North American veteran population in a prospective randomized fashion. We anticipate this study will be a prerequisite for future studies to revalidate this concept in a civilian-based population in other healthcare settings worldwide.
This current study has several inherent limitations, such as relatively small sample size, and the study was not blinded for the patients and physician, possibly resulting in some bias in data interpretation or reporting of anxiety and pain levels in patients. Our measurements of music's efficacy were solely based on the patients' subjective feelings of anxiety and pain at the time of flexible cystoscopy. Specifically, we used well-validated questionnaires such as the STAI and VAS to determine the levels of our measured parameters, because these tools are widely used for such research worldwide. Lastly, all patients in the music group listened to the same classical music during the procedure. If classical music was not their preferred musical genre, however, this might have affected the results for some patients.
Despite these limitations, our study demonstrates that listening to music during office-based flexible cystoscopy ameliorates feelings of anxiety and pain during this invasive procedure. Music is simple, inexpensive, and readily available, and proves to be an effective adjunct to other maneuvers used at the time of flexible cystoscopy to reduce anxiety and pain. Additional studies are needed to further validate the efficacy of music during flexible cystoscopy in larger randomized studies where patient satisfaction and comfort are end points.
Conclusion
This study demonstrates that listening to music decreases anxiety and pain associated with flexible cystoscopy in a well-matched North American VA population. As a nonpharmacologic and noninvasive intervention, music might be one of the simple but important strategies that can be offered during office-based flexible cystoscopy to improve patient satisfaction and comfort. Hence, we recommend incorporating music as an effective adjunct to other techniques used at the time of flexible cystoscopy to reduce anxiety and pain.
Footnotes
Author Disclosure Statement
No competing financial interests exist.