
Abstract
Purpose:
To investigate the effect of missed internal ureteral stents (IUS) on renal function and to describe different modalities of management and associated morbidity.
Patients and Methods:
A retrospective study included patients with missed IUS (>1 year). The complications of missed IUS were categorized according to the forgotten, encrusted, calcified (FECal) grading system. The estimated glomerular filtration rate (eGFR) was calculated using the Modification of Diet in Renal Disease (MDRD) equation at time of initial stent placement and time of stent removal. An age- and sex-matched group of patients who had IUS and had available follow-up for the same duration of the study group were used as a control.
Results:
A total of 46 missed IUS in 46 patients were included. Complicated stents were reported in 34 (73.9%) patients. FECal grade 1 was reported in 16 (57.2%) patients followed by grade 2 and 4 in 5 (17.8%) patients each. Retrograde removal, visual cystolitholapaxy, ureteroscopy with laser disintegration of encrustations and combined retrograde and antegrade approach have been used in 21, 5, 10, and 9 patients, respectively. In the missed IUS group, the mean±standard deviation (SD) eGFR has declined from 65.5±26.3 mL/min/1.73m2 to 54.3±30 mL/min/1.73m2 (P=0.001). While in the control group, the mean±SD eGFR has increased from 57.5±30 mL/min/1.73 m2 to 66.7±27 mL/min/1.73 m2 (P=0.001).
Conclusions:
Missed IUS were associated with significant complications that necessitated more invasive intervention. In addition, IUS had a negative impact on renal function at time of removal.
Introduction
I
Missed IUS is a serious potential complication and is associated with increased patient morbidity. Current literature focused primarily on the associated encrustation, migration, and fragmentation and the proper management based on retrospective data. 6 –10 On the other hand, no previous data are available regarding the impact of missed IUS on RF. Theoretically, the presence of IUS is associated with increased incidence of urine reflux as well as urinary tract infection (UTI), both of which have a significant impact on RF. Recently, it has been reported that 50% of patients with IUS lasting more than 3 months experienced a decline in RF during follow-up. 11
This study aims to evaluate RF outcome in patients with missed IUS in comparison with baseline RF. In addition, to control for the effect of age and other cofactors on RF, a matched control group formed of patients who underwent temporal IUS and has the same duration of follow-up was used for comparison.
Patients and Methods
After obtaining Institutional Review Board approval, a retrospective study was conducted to evaluate RF outcome in patients admitted for removal of missed IUS between January 2013 and January 2014. Inclusion criterion was missed IUS for more than 1 year. Patients with IUS fixed for malignant diseases or planned for permanent stent fixation were not included in the study.
Data collection
The following data were retrieved from the electronic database and included age, sex, body mass index, medical comorbidities, and American Society of Anesthesiologists score at time of stent removal. From the laboratory data, serum creatinine measurements were retrieved at time of stent placement (nadir) and at time of removal. In all cases, the polyurethane Double-J stent was fixed to relieve upper tract obstruction or for postoperative stent placement. The nature, the level, and the side of obstruction and complicated stents were identified. Stent complications included encrustation, obstruction, migration, broken stent, secondary stones, and UTI.
Intervention
All patients received preoperative antibiotics according to the results of urine culture. With the patient in the supine lithotomy position and under the effect of spinal anesthesia, trial removal of the IUS was attempted in a retrograde manner. If this failed, trial removal with the aid of ureteroscopy and laser disintegration of stones and encrustation was performed. If retrograde removal failed, the patients were turned to the prone position and underwent percutaneous renal puncture and antegrade removal of the IUS. Different methods of intervention and associated complications were reported. The complications were graded according to the modified Clavien system.
Outcome assessment
The primary outcome was the changes in RF at time of IUS removal. Renal function was assessed by estimated glomerular filtration rate (eGFR) calculated using the Modification of Diet in Renal Disease equation (MDRD) at the time of stent insertion and at the time of stent removal. 12
We retrieved from the dedicated electronic data the patients who were treated by fixation of a temporary IUS in the same period at which the missed IUS were fixed. Patients who underwent removal of the stent at the due time were identified. Those passed a period without IUS similar to the period of stent missing were determined. Then these patients were called and asked to be enrolled in the study. Among 86 patients eligible for evaluation, a matched 46 patients were included and underwent serum creatinine and ultrasonographic evaluation of the upper urinary tract and had their baseline and follow-up eGFR calculated. The secondary outcome was to assess the morbidity and management of missed IUS removal. Encrustation was assessed by preoperative CT and intraoperative finding using the FECal (forgotten, encrusted, calcified) scale (Table 1). 9 Secondary stones and encrustation were used to assess stone burden by the formula stone burden=length×width on CT and radiography. The stone burden was considered mild if≤100 mm2, moderate if 101 to 400 mm2 and severe if >400 mm2, 13
Statistical analysis
The comparison of mean values between independent groups was performed using the Student t test while comparison of matched groups was performed using paired t test. The comparison of changes in the eGFR values between the study and control group was performed using repeated measure analysis of variance. Bivariate correlations between continuous variables were tested using the Spearman rho. All statistical tests were performed using IBM v. 20 (Chicago, IL), with a P value of less than 0.05 considered significant.
Results
A total of 46 patients underwent surgical removal of 46 missed IUS during the specified period. IUS were fixed on emergency and elective basis in 34 (73.9%) and 12 (26.1%) patients, respectively. The IUS were missed for a median (range) of 19 (12–96) months. Patients' demographics are enlisted in Table 2. Stent complications were reported in 34 (73.9%) patients. Encrustation was the most common complication in 70.5%. Complications of missed IUS are described in Table 3.
IUS=internal ureteral stent; SD=standard deviation; DM=diabetes mellitus; ASA=American Society of Anesthesiologists; BMI=body mass index; LUTS=lower urinary tract symptoms.
FECal=forgotten, encrusted, calcified; UTI=urinary tract infection; IUS=internal ureteral stent.
Management of IUS
Nephrectomy was performed in one patient with a nonfunctioning kidney. In 21 patients, retrograde removal of the missed IUS was performed; these stents were noncomplicated, complicated with encrustations, and migrated in 12, 8, and 1 cases, respectively. Percutaneous antegrade removal of three stents was performed because of encrustations on the upper coil. Combination of both approaches was needed for removal of four broken missed IUS and two IUS with encrustation on the upper coil (FECal grade 3). Visual cystolitholapaxy was performed for five IUS with FECal grade 4 encrustations on the lower coil before removal of the IUS. The remaining 10 stents needed the use of ureteroscopy for removal using laser lithotripsy to disintegrate encrustation and secondary stones in 7 and 2 patients, respectively. In the remaining one, ureteroscopy was used to remove upward migrated IUS.
Perioperative complications
Perioperative complications were reported in 8 (17.4%) patients. Postoperative pain and fever were reported in six patients (modified Clavien grade I) that were managed by oral antipyretics. Ureteral mucosal injury was reported in one patient (modified Clavien grade IIIa) and necessitated refixation of a stent for an additional 4 weeks. Postoperative urinary sepsis was reported in one patient (modified Clavien grade IVa), and the patient recovered with proper antibiotic treatment.
Effect of missed IUS on RF
In the missed IUS group, the mean±standard deviation (SD) eGFR has declined from 65.5±26.3 mL/min/1.73m2 to 54.3±30 mL/min/1.73m2 (P=0.001), while in the control group with the same follow-up duration, the mean±SD eGFR has increased from 57.5±30 mL/min/1.73 m2 to 66.7±27 mL/min/1.73 m2 (P=0.001). When comparing the eGFR between both groups at baseline and at last follow-up separately, there was no difference between the mean eGFR between both groups at baseline (P=0.1), while at last follow-up, the difference reached marginal significance (P=0.05). When comparing the change of renal function in both groups, there was no significant difference (P=0.6). Figure 1 demonstrates the changes in renal function in both groups.
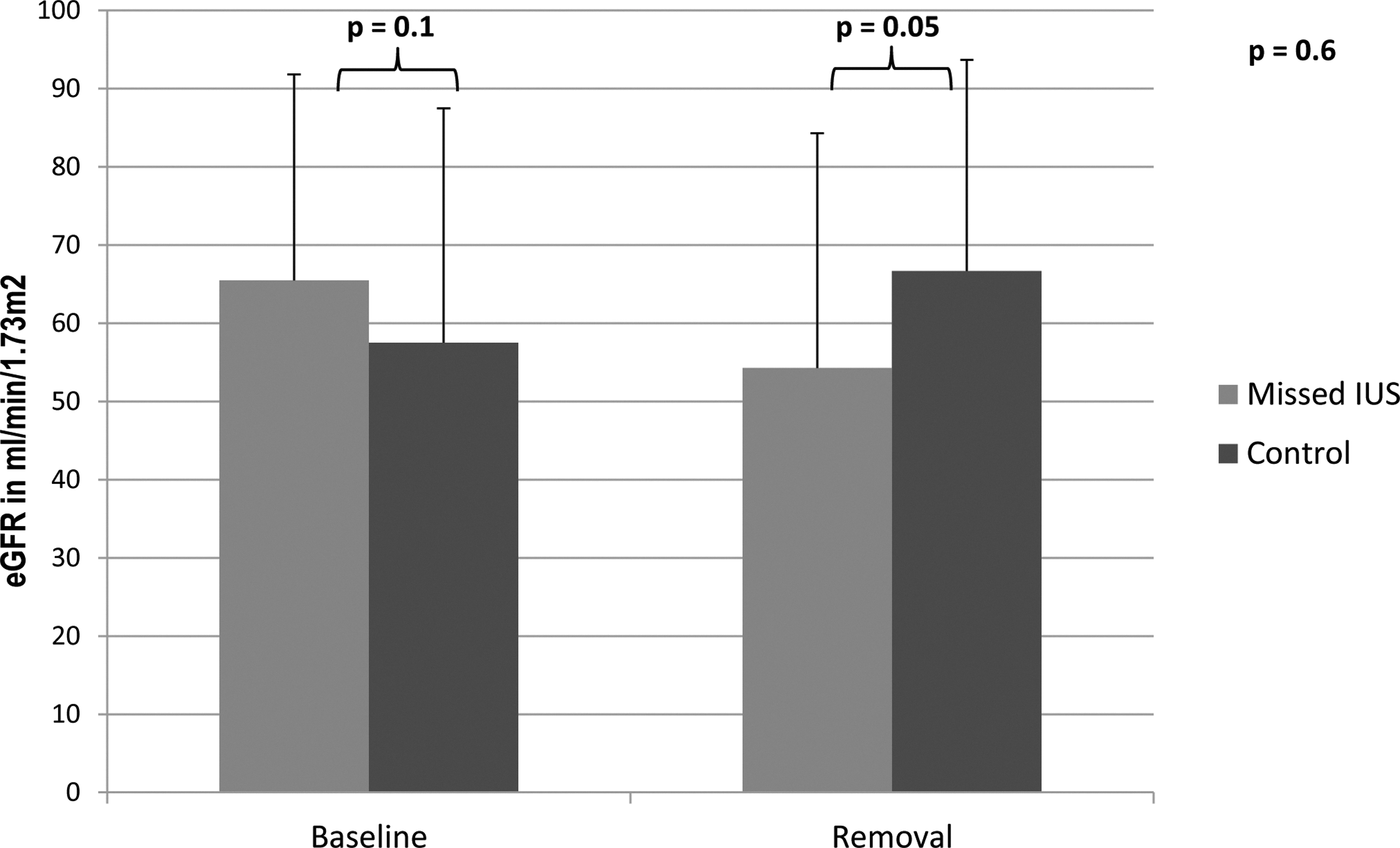
The changes in renal function at baseline and time of removal of missed internal ureteral stents (IUS) and at time of removal of IUS and last follow-up for control group. eGFR=estimated glomerular filtration rate.
Among the study group, complicated IUS have no statistically significant reduction in eGFR when compared with noncomplicated missed IUS (P=0.5). The indwelling time of the IUS appeared to have no statistically significant correlation on eGFR changes before and after stent removal (Spearman rho=0.154 and P=0.3). Positive urine culture was associated with statistically significant reduction in eGFR (P=0.02).
Discussion
A forgotten IUS is a serious complication that is most likely because of patient noncompliance, lack of understanding, and poor administration of stent registry. 14 It has been documented that IUS-related complications are mainly related to stent indwelling time. Monga and associates 15 reported that all cases with forgotten IUS were complicated after a mean indwelling time of 22.7 months. Singh and colleagues 7 reported that after a mean indwelling time of 24.2 months, 14 of 19 forgotten stents were complicated. Kawahara and coworkers 16 reported that 47% of IUS were complicated after 3 months of indwelling. In this report, 74% of missed IUS were complicated with a median indwelling time of 19 months.
Management of the complicated missed IUS is a complex clinical scenario. Simple retrograde removal, antegrade removal, combined approaches, laser and pneumatic lithotripsy disintegration of incrustation, cystolitholapaxy, and open removal have been reported. 10,17 It may necessitate multiple procedures. In the current study, the mean number of the procedure needed for removal of the complicated IUS was 1.2 procedures. Multiple procedures were needed in nine (19.6%) patients. Similar results were previously reported by Weedin and colleagues. 10 Encrustation and secondary stones were managed according to location. Cystolitholapaxy was performed for encrustations on the lower coil. Ureteroscopy with laser disintegration of the encrustation and secondary stones was performed in 19.5% of patients. Pneumatic lithotripsy could be the quicker and more efficient method to remove the encrusted stent. Moreover, the laser may melt the ureteral stent. 18 Many recent studies have demonstrated, however, that holmium:yttrium-aluminum-garnet laser lithotripsy is superior to pneumatic lithotripsy in terms of better fragmentation and lower complication rates. 19,20 In this study, ultrasound and pneumatic lithotripsy were used during antegrade removal of the stent.
There are many potential factors lying behind retained IUS including patient noncompliance, forgetting the stent, the lack of access to medical care, and the poor administration of a stent registry. 16,21 Patient education and establishing a tracking system for stent identification is of paramount importance to reduce such a complication. It has been shown that computer systems based on paperwork performed by surgeons have been used to track stents with some success. Nevertheless, they provided little advantages over the routine paper system. 22,23 Lynch and associates 21 have developed an electronic stent registry that operates continuously without dependence on human interrogation. This system has improved the stent insertion capture rate.
Despite the fact that previously published studies had assessed the complications of the missed IUS and the proper way to solve this surgical dilemma, few studies have addressed the effect of stent missing on RF. 7,8 These studies included a small number of cases, and even the impact on RF was not the primary outcome of interest. In one multicenter retrospective study, Modi and coworkers 24 reported reduction of serum creatinine in 35% of cases with indwelling stents. Serum creatinine, however, is not an accurate estimate of the RF, and the included patients had malignant ureteral obstruction. In the current study, we evaluated the changes in the RF in patients with missed IUS for more than 1 year by changes in eGFR using the MDRD formula at the time of stent insertion and at the time of its removal. We detected a significant deterioration of RF at the time of IUS removal.
Several mechanisms have been postulated to explain the potential deterioration of RF with the forgotten IUS. Complicated stents especially with encrustation and secondary stones resulted in progressive hydronephrosis and subsequent RF deterioration. 7,8 In the current study, 74% of the missed IUS were complicated and 65.2% were complicated with encrustations and secondary stones. Stent complication, however, was not an independent predictor of renal function deterioration. In addition, hydronephrosis has been noticed to progress with indwelling time. Indwelling time is reported to be an important factor in deterioration of RF in patients with indwelling IUS. This is explained by increasing the incidence of stent complications and impaired ureteral peristalsis and the vesicoureteral reflux that accompany the presence of the stent. 11,15,16,25 Nevertheless, indwelling time was not significantly correlated with the deterioration of RF in the current study. A larger sample size might be needed to detect this effect.
Moreover, UTI was reported to be independent predictor of RF deterioration in patients with indwelling IUS because of the potential risk of renal scarring and especially in the presence of urinary reflux. 11,26 Paick and associates 27 reported that bacterial colonization of the stent begins 2 weeks after placement and the rate of colonization increases with longer periods. In this study, 52.2% patients had positive urine cultures at the time of stent removal and it was associated with statistically significant reduction on RF. Because culturing of the stent is more accurate in identifying UTI, 26,28 there might be underestimation of the impact of positive urine cultures in the current study. On the other hand, it is to be noted that positive stent culture does not necessarily translate into a clinically significant UTI.
We hypothesized that if the IUS were removed in the due time, there would have been a better effect on RF outcome. Therefore, we identified from our electronic database a matched group of patients who underwent placement and removal of IUS and had the time elapsed since removal of the stent equal to the period of the missed IUS group. Surprisingly, we have shown that the mean eGFR had improved between the time of removal of the IUS and the time of last follow-up. Therefore, the best treatment of missed IUS is to avoid it with its associated complications and the need for complicated surgical procedures to remove it. This could be done by proper education of the patients that they have a foreign body that needs to be removed and establishing a proper registry system for stent identification and recall in the determined time.
To the best of our knowledge, this is the first study with a primary focus on assessing changes in the RF in patients with missed IUS. Nevertheless, the study has several limitations. Being a retrospective study with the inherent problem of selection bias of cases is a major concern, but this study could not be applicable in a prospective manner. The relatively small number of cases that may affect the study results is another limitation. The effect of other confounding variables on RF could not be assessed because of the small number of patients. Last, there are no available data about renal function after the removal of forgotten stents that might give the whole picture about RF recoverability.
Conclusion
Missed IUS are associated with added comorbidity that requires more than just removal. From the findings of this study, there is a significant decline in RF at time of stent removal. All efforts should be exerted to ensure IUS removal on time and avoidance of such complications.
Footnotes
Author Disclosure Statement
No competing financial interests exist.