
Abstract
Purpose:
To evaluate the ignition and burn risk associated with contemporary fiberoptic and distal sensor endoscopic technologies.
Materials and Methods:
We used new and used SCB Xenon 300 light sources to illuminate a 4.8 mm fiberoptic cable, 10 mm laparoscope, 5 mm laparoscope, rigid cystoscope, semirigid ureteroscope, flexible cystoscope, flexible fiberoptic ureteroscope, distal sensor cystoscope, and a distal sensor ureteroscope (Karl Storz, Inc., Tuttlingen, Germany). We measured peak temperatures at the distal end of each device. We then evaluated each device on a flat and folded surgical drape to establish ignition risk. Finally, we evaluated the effects of all devices on human cadaver skin covered by surgical drape.
Results:
Peak temperatures recorded for each device ranged from 26.9°C (flexible fiberoptic ureteroscope) to 194.5°C (fiberoptic cable). Drape ignition was noted when the fiberoptic cable was placed against a fold of drape. Contact with the fiberoptic cable, 10 mm laparoscope, 5 mm laparoscope, and distal sensor cystoscope resulted in cadaver skin damage. Cadaver skin damage occurred despite little or no visible change to the surgical drape. Rigid and flexible fiberoptic cystoscopes and flexible fiberoptic ureteroscopes had no effect on surgical drapes or cadaver skin.
Conclusions:
Fiberoptic light cables and some endoscopic devices have the potential to cause thermal injury and drape ignition. Thermal injury may occur without visible damage to drapes. Surgeons should remain vigilant regarding the risks associated with these devices and take necessary safety precautions to prevent patient injury.
Introduction
C
Xenon light sources are known to provide sufficient illumination to perform laparoscopic or endoscopic procedures. When compared with alternative technologies, however, such as light emitting diode (LED) or halogen light sources, xenon light sources may generate higher temperatures and more potentially damaging thermal energy. 3 Recently, a patient was reported to have full thickness cutaneous burns after a fiberoptic cable was left on the operating table while connected to a xenon light source. 4 While fiberoptic cables have been clearly associated with thermal injuries in the operating room, 5,6 it is currently less clear whether different types of cystoscopes and ureteroscopes, including those equipped with distal sensor technologies, are also capable of generating damaging levels of heat when illuminated by a xenon light source.
Previous studies have evaluated for burn risk associated with fiberoptic light cables and some endoscopic devices. 1 –6 Andonian and colleagues 7,8 evaluated digital endoscopic devices equipped with internal light sources and distal sensor technology and found that these contemporary technologies may reduce risk of drape ignition and thermal injury. To the best of our knowledge, no previous study has provided a comprehensive comparison of burn risk associated with fiberoptic light cables, laparoscopes, conventional cystoscopes and ureteroscopes, as well as contemporary distal sensor cystoscopes and ureteroscopes.
We performed an in vitro study to systemically evaluate the risk of thermal injury associated with fiberoptic light cables, 10 mm laparoscopes, 5 mm laparoscopes, rigid cystoscopes, semirigid ureteroscopes, flexible fiberoptic cystoscopes, and flexible fiberoptic ureteroscopes, as well as distal sensor cystoscopes and distal sensor ureteroscopes. Potential burn risk was evaluated by exposing each device to surgical drapes and human cadaver skin.
Materials and Methods
Light sources and instruments evaluated
We evaluated seven standard fiberoptic endoscopic devices: A standard gray fiberoptic light cable (495 NE 4.8 mm) (Karl Storz, Inc., Tuttlingen, Germany), 10 mm Hopkins II 0° laparoscope (26003AA Karl Storz, Inc.), 5 mm Hopkins II 0° laparoscope (26006AA Karl Storz, Inc.), rigid cystoscope (27410SK Karl Storz, Inc.), semirigid ureteroscope (27010L Karl Storz, Inc.), 15F flexible fiberoptic cystoscope (11272CU1 Karl Storz, Inc.), and 6.7F flexible fiberoptic ureteroscope (11278AU1 Karl Storz, Inc.). Two Karl Storz SCB Xenon 300 light sources (20133120 Karl Storz, Inc.) were used to illuminate each fiberoptic device. One light source was equipped with a used xenon bulb (55 usage hours) while the other included a new xenon bulb (0 usage hours). We also evaluated two distal sensor endoscopic devices; a series 11272 VNU flexible video-urethro-cystoscope (96136011D Karl Storz, Inc.) and a series 11278 VU flexible video-uretero-renoscope FLEX-XC (96136014D Karl Storz, Inc.). The distal sensor cystoscope was illuminated using the SCB Xenon 300 light source (Karl Storz, Inc.) and the distal sensor ureteroscope used a built-in LED light source incorporated into the handle of the device.
Temperature measurements
Using both new and used xenon bulbs, we measured temperatures using a TM-902C K-type digital thermometer with thermocouple probe (Apuhua Electronic Technology Co., LTD, Guang Dong, China). We placed the tip of the thermocouple probe in contact with the distal end of each device and recorded the baseline temperature (room temperature). No difference was observed between room temperature and the starting temperature of each device. Time recording began when the light source was powered on to an intensity set at 100%, and temperatures were recorded from the digital thermometer liquid crystal display (LCD) at 30 second intervals for the first 2 minutes and then 1 minute intervals until a total time of 10 minutes. Subsequently, we powered off the light source and allowed all instruments to cool to room temperature. Peak temperatures for each device were recorded after 10 minutes.
Experimental procedure
After temperatures of the devices were measured, we placed the distal end of each device in contact with surgical drapes made of woven fibers (Kimberly-Clark Health Care, Roswell, CA) to evaluate for ignition or charring. After turning on the light source equipped with the used xenon bulb for 10 minutes, we positioned the device flat on a 10 cm×10 cm surface of drape for 5 minutes. The time in which charring began and the appearance of the drape were recorded for 5 minutes. Next, starting from the baseline temperature, we again turned on the light source for 10 minutes and placed the distal end of the device directly against a 2 cm fold in the drape for 5 minutes. Again the time of charring and final appearance were recorded. We repeated this method for each of the nine devices included in our study.
To further investigate the risk of thermal injury to human tissue, we obtained a fresh human cadaver forearm. The skin of the forearm was covered with surgical drape. After illuminating the light source with a used xenon bulb for 10 minutes, we systemically placed the distal end of the endoscopic device directly in contact with the drape for three different time intervals: 30 seconds, 2 minutes, and 10 minutes. After each period, the appearances of the surgical drape and the underlying skin were recorded. This protocol was repeated for each of the nine endoscopic devices.
Our primary outcome included peak temperatures reached by the fiberoptic cable, laparoscope, and endoscopy devices after the new and used light sources were illuminated for 10 minutes at 100% intensity. Additional metrics included the presence of charring, discoloration, or any change in appearance in surgical drapes; and the presence of burns, discoloration, or any change in appearance to cadaver skin after timed exposures to each device.
Results
Peak temperatures recorded for each device after 10 minutes ranged from 26.9°C (flexible fiberoptic ureteroscope) to 194.5°C (fiberoptic cable) using a used xenon bulb and 28.1°C (flexible fiberoptic ureteroscope) to 192.4°C (fiberoptic cable) using a new xenon bulb (Fig. 1). Using used and new xenon bulbs, the 5 mm and 10 mm laparoscopes reached temperatures of 71.1°C –75.0°C and 48.7°C–50.6°C, respectively. Peak temperatures reached using new bulbs averaged 2.3°C greater than temperatures achieved using used xenon bulbs. Of note, the distal sensor cystoscope and ureteroscope heated to temperatures higher than the rigid or flexible fiberoptic devices (Fig. 2). No visible thermal damage occurred with any instrument when laid flat on the drape surface, but significant charring resulting in a 6 mm×8 mm hole was noted when the fiberoptic cable was placed against a fold of drape. In fact, charring began 2 seconds after the fold was exposed to the tip of the fiberoptic cable. Minor gray-colored charring of the folded surgical drape was observed after 5 minutes of direct contact with the 10 mm laparoscope, 5 mm laparoscope, and distal sensor cystoscope (Table 1).
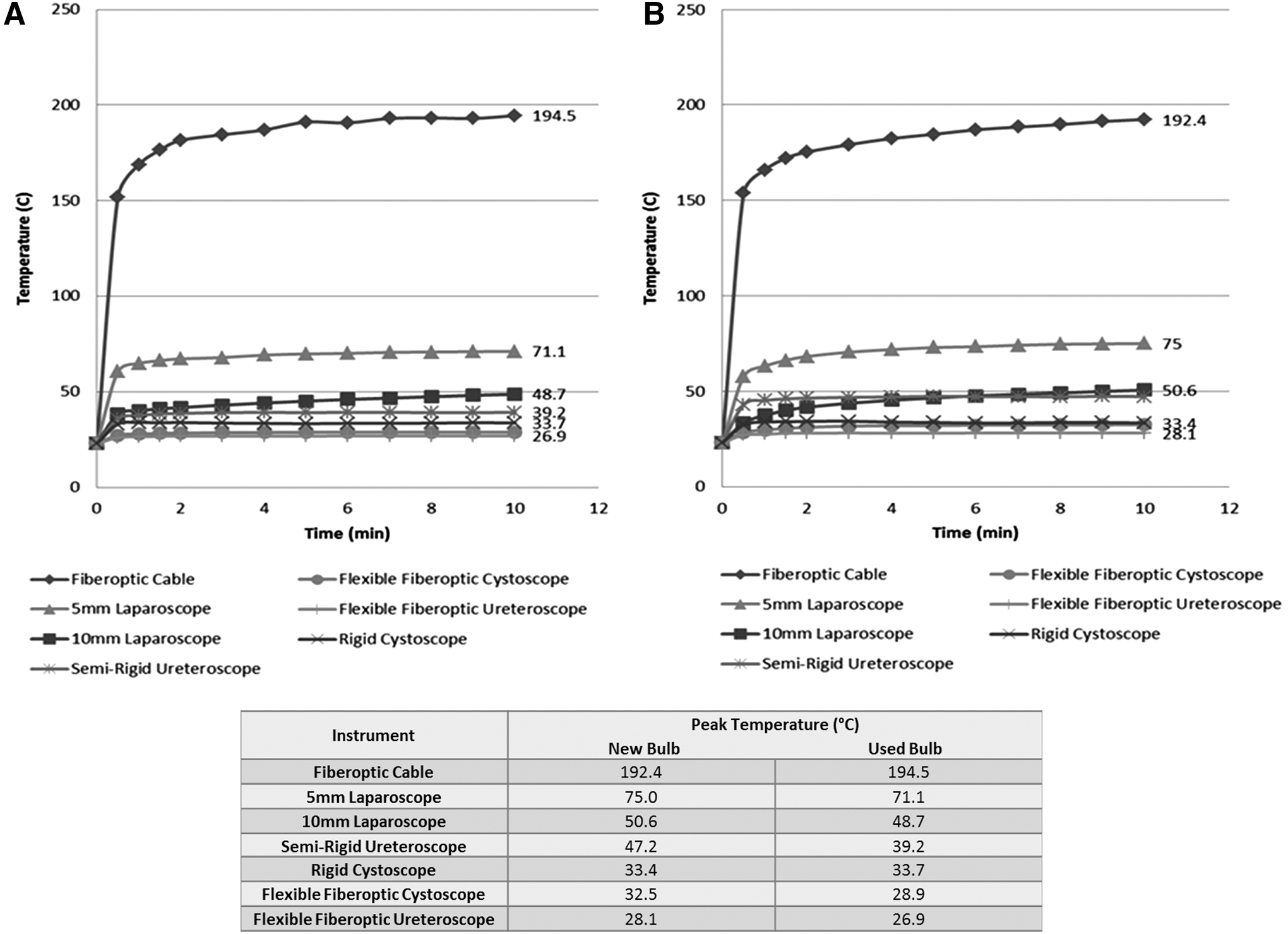
Peak temperatures of contemporary endoscopy technology illuminated by (
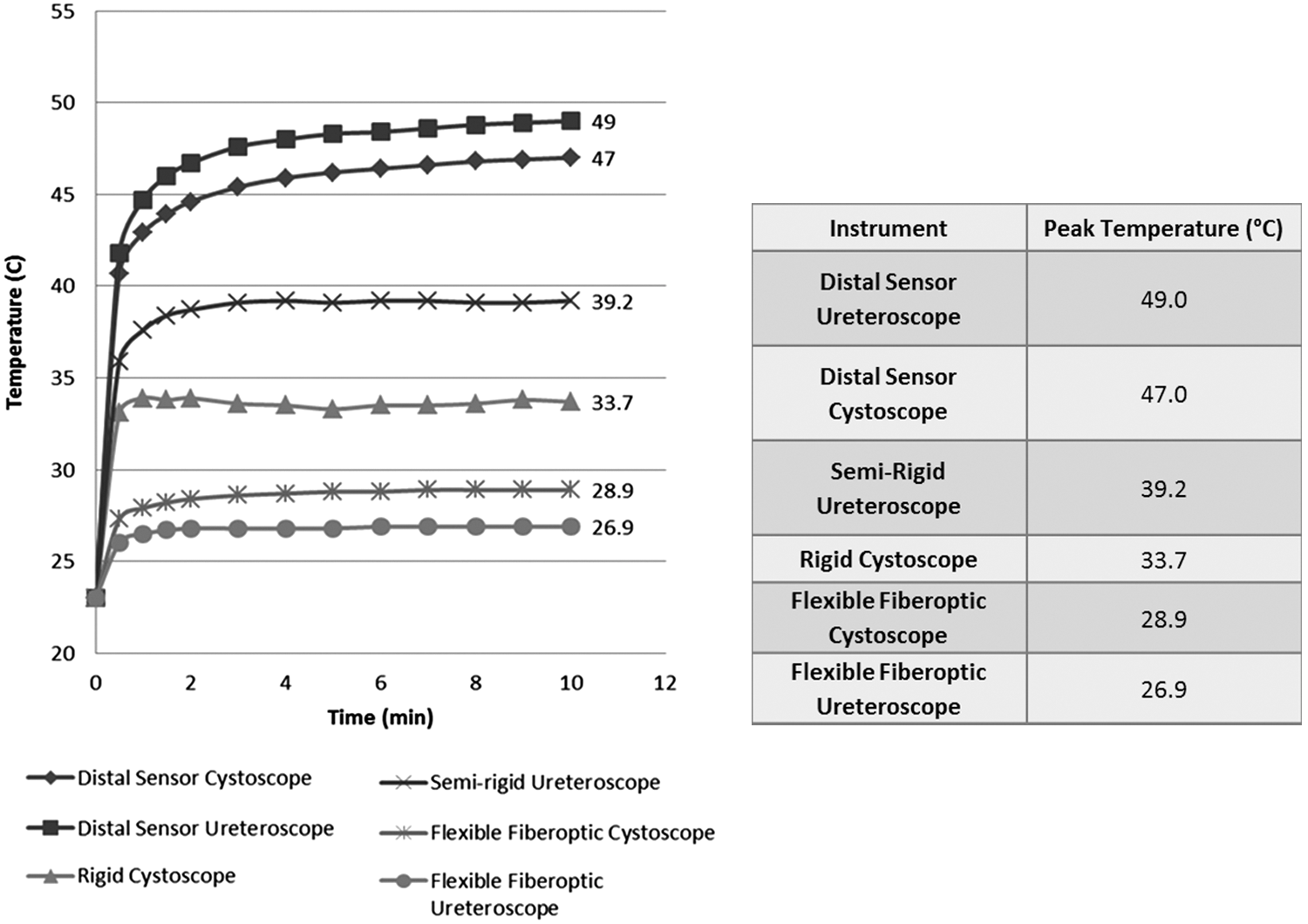
Comparison of peak temperatures for different ureteroscope and cystoscope devices.
NC=no change.
The fiberoptic cable and 5 mm laparoscope caused cadaver skin burns in as little as 30 seconds when exposed directly to drape-covered cadaver skin (Fig. 3 and 4). Longer exposures resulted in larger and darker colored cutaneous burns. Contact with the 10 mm laparoscope and distal sensor cystoscope for 10 minutes caused a noticeable gray discoloration of the cadaver skin. In all cases, the area of cadaver skin damage exceeded the area of damage to surgical drapes. Remarkably, contact with the 10 mm laparoscope, 5 mm laparoscope, and distal sensor cystoscope resulted in underlying cadaver skin damage despite there being no visible change to the surgical drape. No thermal damage to drape or cadaver skin was appreciated after 10 minutes of exposure to the rigid cystoscope, semirigid ureteroscope, flexible fiberoptic cystoscope, flexible fiberoptic ureteroscope, or distal sensor ureteroscope (Table 1).
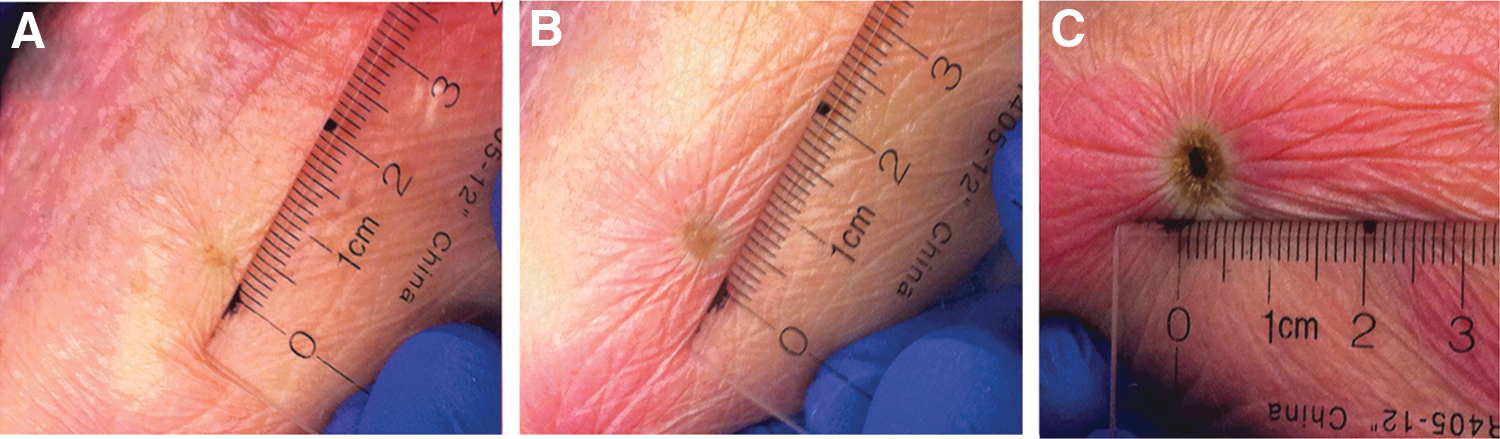
Human cadaver skin covered with surgical drape exposed to fiberoptic light cable for (
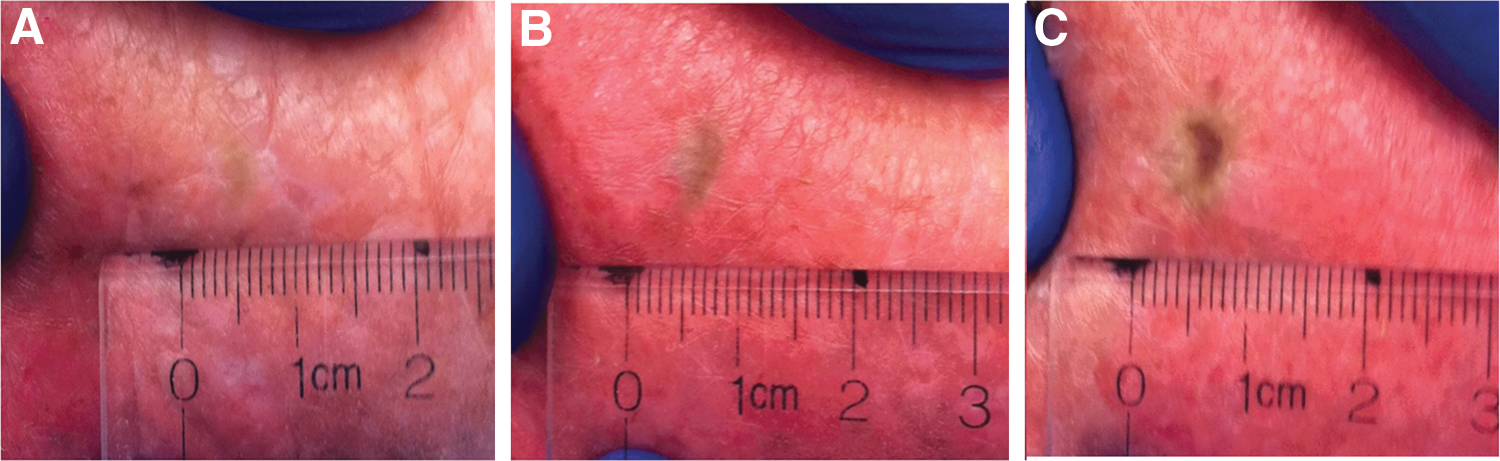
Human cadaver skin covered with surgical drape exposed to 5 mm laparoscope for (
Discussion
Our findings revealed that the fiberoptic cable produced temperatures significantly greater than other endoscopy instruments. Not only was the fiberoptic cable hotter than other instruments, but it also heated up more expeditiously than the other devices we studied. In only 30 seconds, the fiberoptic cable was capable of heating up to temperatures greater than 150°C. In 2008, Hindle and coworkers 5 evaluated at the histologic level the volume of cutaneous tissue damage occurring after direct contact with the tip of a fiberoptic cable. Their results showed significant volumes of injury occurring after only 15 seconds of contact, and longer exposure times were associated with larger volumes of tissue damage. 5 It is clear that fiberoptic light cables are capable of producing harmful levels of thermal energy in very brief periods. Like other hazardous instruments in the operating room, fiberoptic cables should be used with caution and attended to during procedures. Contact with skin or surgical drapes, even for a few seconds, should be avoided. Not only do fiberoptic cables pose a burn risk to patients, they can also present a real risk for drape ignition if placed in contact with surgical drapes. 6
A previous study that compared used and new xenon light source bulbs found that new bulbs were capable of producing temperatures significantly higher than used bulbs. 5 In that study, peak temperatures at the distal end of a fiberoptic cable using new bulbs were over 100°C hotter than used bulbs. Total usage hours of their used bulbs, however, were not reported in this study. Our findings suggest that bulb status has a minimal effect on peak temperatures of endoscopic devices when the bulb has been previously used for 55 hours. Temperatures were similar between bulbs with peak temperatures averaging only 2°C to 3°C hotter for fiberoptic devices illuminated with a new bulb compared with the used xenon bulb.
Cutaneous tissue damage is expected to occur when skin is exposed to temperatures above 50°C. 9 In our study, the 5 mm laparoscope reached temperatures greater than 70°C, and a previous study recorded temperatures as high as 95°C 10 at the distal end of a laparoscope. It has been suggested that fiberoptic endoscopes do not pose a significant burn risk in the operating room. 6 Our results, however, clearly demonstrate that a 5 mm laparoscope can cause skin burns in as little as 30 seconds of exposure. Furthermore, other endoscopic instruments that approach peak temperatures of 50°C can cause discoloration to cadaver skin with prolonged exposure. Ten minutes of exposure to the 10 mm laparoscope and distal sensor cystoscope resulted in gray skin discoloration in the cadaver model. Interestingly, the distal sensor ureteroscope device, which recorded a peak temperature of 49°C, did not cause noticeable skin discoloration after 10 minutes of exposure. This may be because of the smaller area of skin contact on the distal end of the ureteroscope or the type of light source used by the distal sensor ureteroscope. While the distal sensor cystoscope uses a xenon light source, distal sensor ureteroscopes are illuminated using LED light sources that may produce a broader, more homogeneous distribution of light and deliver lower doses of photons to human tissue. 11
In all cases of burns found in our study, the area of skin damage exceeded the area of visible damage to surgical drapes. In the case of the 10 mm laparoscope, 5 mm laparoscope, and distal sensor cystoscope, thermal damage to skin occurred in the absence of any visible changes to overlying surgical drapes. It is evident that human tissue may be more susceptible to thermal injury than drapes. This finding is concerning because many surgeons likely believe that patients are safe if there is no evidence of a burn on the surgical drape. Clearly, surgical drapes have the capacity to mask underlying thermal injury to patients. Underlying skin burns could be initially missed if they are hidden by normal-appearing surgical drapes. Therefore, it is important that surgeons take the necessary time to inspect skin under drapes if there is any suspicion that the patient has been exposed to endoscopic energy sources. All healthcare team members in the operating room should be aware of the burn risk associated with endoscopic devices, take necessary safety precautions to avoid unnecessary exposure to illuminated devices, and report any incidents of exposure during procedures.
Some endoscopic instruments are unlikely to result in thermal injury to patient skin even after prolonged exposure. Our findings suggest that rigid cystoscopes, semirigid ureteroscopes, flexible fiberoptic cystoscopes, and flexible fiberoptic ureteroscopes likely do not pose a risk for direct thermal injury. Furthermore, these devices caused no visible change to surgical drapes or cadaver skin. Despite these findings, good technique should always be practiced, and patient exposure to these devices should be minimized despite the diminished risk of injury.
Our study is the first to systematically compare peak temperatures produced by distal sensor endoscopes and their conventional counterparts. While distal sensor devices are similar in size and shape to other types of endoscopic devices, they reached peak temperatures close to 50°C, hotter than other types of cystoscopes or ureteroscopes. Like the other types of cystoscopes, the distal sensor cystoscope uses a xenon fiberoptic light source. The distal sensor ureteroscope, however, is equipped with a LED light source built into the handle of the device. Previous studies have reported the potential of LED technology providing illumination in laryngoscopic and colonscopic procedures with decreased heat production compared with xenon light sources. 3,12 Our initial findings, however, suggest that the LED-illuminated ureteroscope produces more thermal energy than its xenon-illuminated counterparts. Additional studies comparing a larger number of LED and fiberoptic urologic devices may shed more light on this matter.
All laparoscopic and endoscopic surgeries need light sources for proper visualization of tissue, and these light sources are capable of generating thermal energy. Our study systematically demonstrates the risks associated with instruments that use fiberoptic and LED light sources. While there appears to be little risk of thermal injury from rigid or flexible fiberoptic cystoscopes and ureteroscopes, the distal ends of fiberoptic cables, 10 mm laparoscopes, 5 mm laparoscopes, and distal sensor cystoscopes are capable of generating temperatures high enough to damage human cadaver skin. Furthermore, cutaneous burns are possible even when no charring or damage to surgical drapes occurs. Therefore, it is of utmost importance that healthcare professionals be aware of the risks associated with these devices and take necessary safety precautions in the operating room to prevent patient injury. Based on our findings, we have developed a list of safety recommendations to be implemented in safety training programs for healthcare professionals working in the operating room. We advise surgical teams to always turn off light sources when not in use, avoid placing fiberoptic devices near patients or surgical drapes, and inspect skin under surgical drapes if thermal injury is suspected. A complete list of safety recommendations is found in Table 2.
There are several limitations in our study. Our experiment was limited to evaluation of a single manufacturer because of the availability of these technologies at our institution. We would not anticipate, however, a vast range in the performance and the heat generated across different manufacturers of contemporary endoscopic technology, which all use very similar technologic concepts. The cadaver model applied in this evaluation is another limitation, because thermal changes caused by endoscopic instruments in living human subjects may be different than changes observed with cadaver skin. Finally, our study used only one method of temperature measurement and did not include real time or continuous temperature measurements. Including additional heat detection methods, such as modern thermal imaging infrared cameras, may provide more accurate temperature ranges for each device evaluated in this study. Temperature measurements using thermocouples, however, have been shown to be accurate in previous studies. 5,13,14
Conclusion
Fiberoptic light cables, 10 mm laparoscopes, 5 mm laparoscopes, and distal sensor cystoscopes are capable of generating temperatures high enough to cause cutaneous thermal injury. Rigid cystoscopes, semi-rigid ureteroscopes, flexible fiberoptic cystoscopes, flexible fiberoptic ureteroscopes, and distal sensor ureteroscopes, however, pose limited risk for direct thermal injury. Significant tissue injury can occur in the absence of visible damage to surgical drapes. As such, surgeons should be aware of the risks associated with fiberoptic cables, laparoscopes, and some endoscope devices and take necessary safety precautions to prevent patient injury.
Footnotes
Acknowledgments
The authors thank Susan Demas from the Department of Orthopedic Surgery surgical skills laboratory at the University of California, Irvine, for her technical assistance. We also thank the Willed Body Program for providing the human specimen used in this study and Karl Storz, Inc. for providing the endoscopic technology.
Author Disclosure Statement
No competing financial interests exist.