
Abstract
Purpose:
To determine risk factors of reoperation after holmium laser enucleation of the prostate (HoLEP) for management of lower urinary tract symptoms (LUTS) secondary to benign prostatic hyperplasia (BPH) with time to event analysis.
Methods:
A prospectively maintained database was reviewed for patients undergoing HoLEP. Baseline and follow-up data were compared in terms of International Prostate Symptoms Score, quality of life, peak flow rate, residual urine, and prostate-specific antigen (PSA) at 1, 6, and 12-months and then annually. Perioperative and late adverse events were recorded. Reoperation was defined as the need for any surgical intervention to relieve bothersome LUTS after HoLEP. Multivariate logistic regression was used to determine covariates associated with reoperation and the Kaplan-Meier curve assessed the time to reoperation.
Results:
A total of 1216 HoLEP procedures were performed between March 1998 and October 2013 with a mean prostate volume of 94.8±52.7 cc. Catheter time and hospital stay were 1.4±1.9 and 1.3±1.6 days, respectively. After a median follow-up of 7.6 years (1–14 years), 52 (4.3%) patients needed reoperation for recurrent LUTS, including 13 (1.07%) for residual/recurrent adenoma, 14 (1.15%) for bladder neck contracture (BNC), and 25 (2.05%) for de novo urethral stricture. In multivariate regression, smaller prostate size (<62 cc), PSA reduction <50%, and history of previous prostate surgery were significantly associated with recurrence of adenoma. BNC was significantly associated with smaller glands (<54 cc) while longer operative time and postoperative catheterization were significantly associated with urethral stricture. Kaplan-Meier curve demonstrates post-HoLEP freedom from reoperation of 96.9% at 5 years and 95.1% at 10 years.
Conclusions:
In a single center large series, HoLEP has 95% reoperation-free probability at 10 years. Relatively small-size prostate may have an impact on recurrence of adenoma and bladder neck contracture. PSA reduction <50% was significantly associated with recurrence of adenoma while longer operative time and postoperative catheterization were significantly associated with postoperative urethral stricture.
Introduction
T
Achieving prostatic cavities similar to those of open prostatectomy, HoLEP proved itself as one of the endoscopic procedures with equal or superior efficacy compared with the traditional transurethral resection of the prostate (TURP). 3 Furthermore, it is not only safe, effective, and durable, 4 –13 even in patients with coagulopathy, 14 but it is also more cost-effective than TURP. 15,16 Meta-analyses have confirmed how well established HoLEP has now become, 9,15,17,18 with a low long-term re-treatment rate and the more pronounced improvement in prostate symptoms score and flow rate than after TURP. 18
Currently, HoLEP is widely accepted and performed in so many centers all over the world, which necessitates improving its technical aspects to minimize postprocedure reoperation. We believe that determination of risk factors associated with long-term reoperation of the procedure will help to address the challenge of increased financial costs associated with the need for reoperation, especially with diseases that significantly increase the economic burden on the healthcare system, such as BPH. This would optimize patients' satisfaction, which represents the cornerstone for any prostatic intervention.
In addition, increasing patients' life expectancy is associated with more need for reoperation that usually challenges the long-term outcome of any prostatic intervention. Therefore, the aim of the present study was to identify risk factors that could be associated with reoperation after HoLEP for management of symptomatic BPH in a large series of patients with relatively long follow-up. Time to event analysis will be an integral outcome parameter.
Methods
Study design
A prospectively collected database, maintained since March 1998, was reviewed for patients who underwent HoLEP for symptomatic BPH. The procedures were performed or supervised by a single surgeon (MME). Demographic, operative, and perioperative parameters were recorded including energy used, operative time (enucleation and morcellation times), hemoglobin, hematocrit and sodium deficit, catheterization time, and hospital stay. Moreover, early adverse events and long-term complications were recorded.
Baseline and follow-up data were compared both subjectively and objectively in terms of the International Prostate Symptom Score (IPSS), quality of life (QoL), peak flow rate (Qmax) (mL/sec), postvoid residual (PVR) urine volume (mL), and prostate-specific antigen (PSA). Postoperative follow-up was performed at 1, 6, and 12 months and then annually.
Outcome measures
Once symptoms and/or an obstructed flow were detected by uroflowmetry, flexible cystoscopy was performed under local anesthesia to diagnose the cause and level of obstruction. Herein, we assessed the need for any surgical intervention to relieve bothersome lower urinary tract symptoms (LUTS) after HoLEP, including redo HoLEP, incision of bladder neck contracture (BNC), and visual urethrotomy for de novo urethral stricture.
Perioperative and follow-up data of each reoperated group were compared with the whole patient population who were not reoperated to determine the possible associated risk factors. Analysis of the time to reoperation (event) will be detailed.
Surgical procedure
HoLEP was performed as described previously. 19 The procedure basically involves anatomic dissection of the prostatic adenoma off the surgical capsule via a retrograde approach, starting at the apex followed by intravesical morcellation of the prostatic tissues. A 100-W holmium laser (Versapulse; Lumenis Inc., Santa Clara, CA) was used with a 550-nm quartz end-firing fiber (SlimLineTM 550, Lumenis Inc.), through a modified continuous-flow 26F resectoscope with a distal bridge and video system. An enucleation loop has been recently used as a laser guide with a retracting beak, and working element. 20
Under general or regional anesthesia and using warm physiologic saline as an irrigant, urethral meatus calibration was performed using Van Buren sounds up to 30F. Then, either a two- or three-lobe technique was used after inspection of the prostate, depending on the prostate anatomy and the presence of a prominent median lobe.
A rigid indirect nephroscope, with a 5-mm working channel, was used to introduce the tissue morcellator (Lumenis Inc.) at the end of the procedure. After morcellation of the prostate tissue, a standard 22F two-way or three-way catheter was inserted whereby intermittent or continuous bladder irrigation was set up, if required. Typically, the urethral catheter was removed the next morning and the patient discharged from the hospital, as long as he was able to void adequately.
Statistical analysis
Data were analyzed using the commercially available Statistical Package for Social Sciences for Windows, version 20 (IBM
Results
Demographic data
A total of 1216 consecutive patients operated on between March 1998 and October 2013 were analyzed, with a mean age of 71.9±12.3 (50–93) years, including 315 (25.9%) patients with an American Society of Anesthesiologists score ≥2. Preoperative and perioperative data are presented in Table 1. The mean preoperative prostate volume measured by transrectal Ultrasonography (TRUS) was 94.8±52.7 (13–380) cc, including 452 (37.2%) patients with prostate volume >100 cc and 156 (12.8%) patients with prostate volume ≥150 cc. Previous prostate surgeries were performed in 85 (7%) patients including 48 (3.9%) TURP, 13 (1.1%) HoLEP, 9 (0.7%) transurethral incision of the prostate, 6 (0.5%) GreenLight photoselective vaporization of the prostate, and 7 (0.6%) other procedures.
Baseline minus immediate postoperative level.
SD=standard deviation; LUTS=lower urinary tract symptoms; ASA=American Society of Anesthesiologists; IPSS=International Prostate Symptom Score.
Perioperative data
Concomitant cystolitholapaxy was performed in 98 (8.1%) patients, transurethral bladder biopsies in 11 (0.9%), and visual internal urethrotomy in 5 (0.4%) patients, while open diverticulectomy was performed for 3 patients. Intraoperatively, 44 (3.6%) adverse events were encountered including 26 (2.1%) intraoperative bleeding, 14 (1.1%) superficial bladder mucosal injuries, 2 (0.16%) urethral injuries, and 2 (0.16%) capsular perforations. Monopolar electrocautery was used in 31 (2.5%) patients either for hemostasis in 28 (2.3%) or residual tissue resection at the end of HoLEP in 3(0.2%) patients. Recystoscopy to complete morcellation was needed for 21 (1.7%) patients while open cystostomy was performed in 3 (0.3%) patients to extract large adenomas.
The mean catheter time and hospital stay were 1.4±1.9 and 1.3±1.6 days, respectively. Preoperative prostate volume was positively correlated with total energy used (r=0.46, P<0.001), total operative time (r=0.48, P<0.001), enucleation time (r=0.42, P<0.001) and morcellation time (r=0.54, P<0.001). Postoperatively, 17 (1.4%) patients failed the first trial of voiding and needed recatheterization, including 9 patients who presented preoperatively with indwelling urethral catheters. Gross hematuria was observed in 16 (1.3%) patients and was managed conservatively (Table 2), while only 15 (1.2%) patients needed perioperative transfusion of blood or packed red blood cells, including 10 (0.8%) patients who were receiving anticoagulants concomitantly.
CIC=clean intermittent catheterization.
Outcome measures
After a median follow-up of 7.6 years (1–14 years), including 64 (5.3%) patients who had a median follow-up of 11.7 years (11-14 years), PSA was reduced by 75%, IPSS improved by 62%, QoL improved by 60%, Qmax improved by 162%, and PVR improved by 88% (Fig. 1). Of 452 (36.8%) patients who presented with indwelling urethral catheters, 9 (2%) patients were unable to void early postoperatively, including 2 (0.5%) patients in whom chronic retention developed necessitating clean intermittent catheterization (CIC).
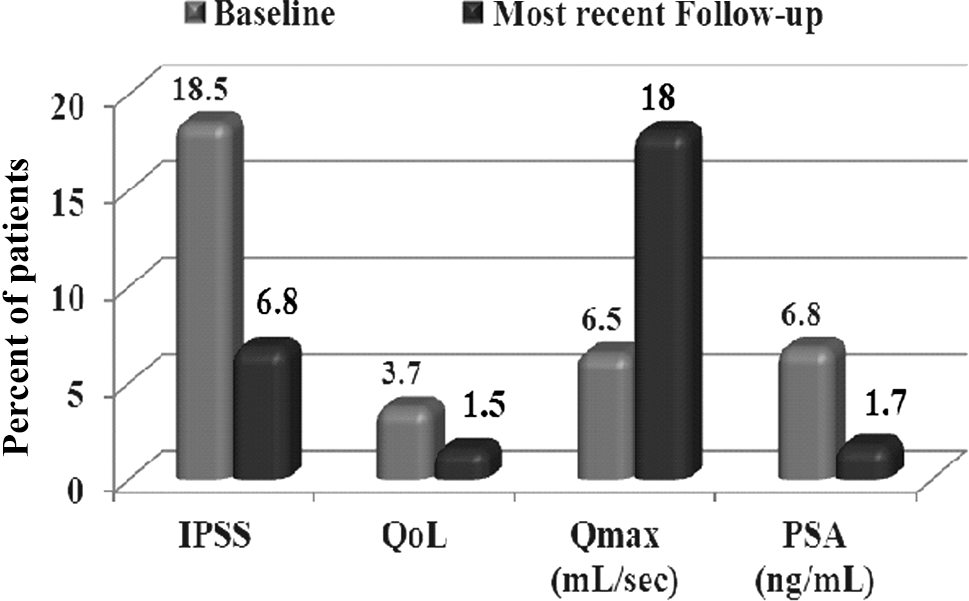
Percent changes of functional outcomes and prostate-specific antigen (PSA) from baseline for patients undergoing holmium laser enucleation of the prostate after a median follow-up of 7.6 years. P<0.001 for all parameters. IPSS=International Prostate Symptom Score; QoL=quality of life; Qmax=peak flow rate.
At the most recent follow-up, stress urinary incontinence (SUI) was noted only in 6 (0.5%) patients, none of whom needed anti-incontinence procedures. Four other (0.3%) patients had chronic retention necessitating CIC. Residual/recurrent adenomas were detected in 13 (1.07%) patients with a median (range) duration for recurrence of symptoms of 80 (21–172) months, including 9 (69.2%) patients who were operated on during the early learning curve (first 2 years) of HoLEP at our institution. BNC had been detected in 14 (1.15%) patients with a median duration of diagnosis of 72 (18–102) months. De novo urethral stricture was detected in 25 (2.05%) patients with a median (range) duration of diagnsis of 20 (12- 49) months.
Bladder stones secondary to recurrent obstruction developed in nine (0.7%) patients. Compared with those who did not have recurrence, patients who underwent redo HoLEP for recurrent adenoma had significantly less percent reduction of PSA at 3 months postoperatively (49% vs 82%, P=0.001), smaller glands detected by the preoperative TRUS (62.4 vs 94.6 cc, P=0.006), previous prostate surgery (38.5% vs 6.5%, P=0.001), and longer operative time (131 vs 105 min, P=0.04). BNC was significantly associated with younger age (67±8.4 vs 72±8 years, P=0.02) and smaller glands (54.2 vs 94.6 cc, P=0.004) (Table 3). Urethral stricture was significantly associated with significantly smaller glands, longer operative time, and longer duration of postperative catheterization (P≤0.01) (Table 3). Time to reoperation was presented by a Kaplan-Meier survival curve (Fig. 2).
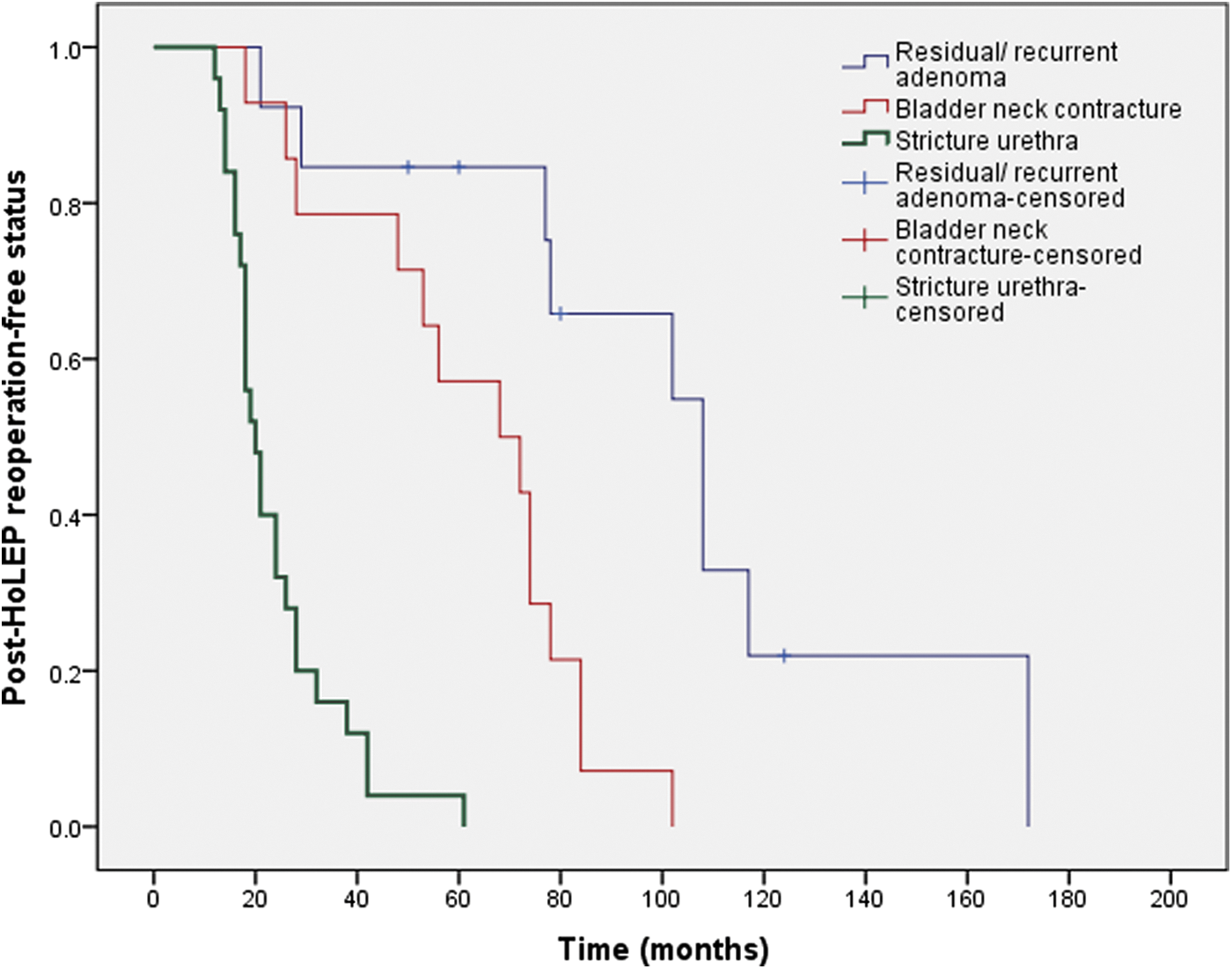
Kaplan-Meier plots showing time to reoperation after holmium laser enucleation of the prostate (HoLEP).
Data are reported as number (%) or mean±standard deviation.
On a multivariate model, however, the percent of PSA reduction <50% at 3 months post-HoLEP (adjusted odds ratio [aOR], 95% confidence interval [CI]): 1.36 [1.14–1.82], P=0.002), smaller prostate size (aOR, [95% CI]: 1.12 [1.02-1.74], P=0.03) and a history of previous TURP (aOR: 4.18 [1.89–7.02], P=0.01) were significantly associated with post-HoLEP recurrence of adenoma. BNC was significantly associated with smaller glands (aOR: 1.84 [1.23–3.58], P=0.02) while a longer operative time (aOR: 1.45 [1.16–2.11], P=0.01) and preoperative catheterization (aOR: 2.37 [1.18–3.13], P=0.02) were significantly associated with postoperative urethral stricture (Table 4). None of the patients in whom regrowth of the adenoma, BNC, or stricture urethra developed had intraoperative complications during their reoperation. A Kaplan-Meier curve demonstrates freedom from post- HoLEP reoperation to be 96.9% at 5 years and 95.1% at 10 years (Fig. 3).

Kaplan-Meier plots showing reoperation-free status after holmium laser enucleation of the prostate (HoLEP).
OR=odds ratio, CI=confidence interval; PSA=prostate-specific antigen; BNC=bladder neck contracture.
Discussion
Since its introduction into clinical practice, HoLEP has been demonstrated to be a safe and efficient option for management of symptomatic BPH. Systematic reviews and meta-analyses confirmed the superior outcome of HoLEP over the monopolar TURP and open prostatectomy in terms of safety, durability, short hospital stay, and cost-effectiveness of its reusable fiber. 9,15,18 Therefore, with continued modification of the technique and development of new supporting technologies, the future of HoLEP looks exciting as a size-independent potential new gold standard for management of bladder outlet obstruction secondary to BPH.
Reoperation for management of recurrent LUTS, however, usually challenges the long-term outcome of any treatment option for BPH, especially with increasing patient age and comorbidities. Therefore, we are sharing our experience in the current report with a large series of HoLEP with up to 14-years of follow-up and trying to address the risk factors associated with post-HoLEP reoperation.
All subjective and objective voiding parameters were significantly improved immediately postoperatively including IPSS, QoL, Qmax, and PVR and maintained their significant improvement after a mean follow-up of more than 7 years. Moreover, PSA maintained its significant reduction by 75% at the most recent follow-up, representing a surrogate indicator for glandular size reduction after HoLEP.
These results are consistent with those reported recently in a comparable large series of HoLEP procedures in terms of safety and efficacy for symptomatic BPH. 21 Both cohorts similarly confirmed the maintenance of long-term improvement in all subjective and objective parameters evaluated that were achieved immediately after the surgical procedure. Moreover, perioperative and long-term complications rates were similarly reported. Only one patient in the former study, however, needed reoperation for prostatic regrowth, which may be because of its relatively shorter follow-up (9.6 months vs 7.3 years, respectively).
De novo SUI, a source of significant stress and anxiety to the patient, might result from excessive stretching of the urinary sphincter during blunt dissection of the prostate apex and usually improves after adaptation of the bladder and sphincter to the relief of obstruction. It persisted only in 0.5% of our patients at the most recent follow-up, which is much lower than reported previously. 12
In the current study, 21 (1.7%) patients needed endoscopy to complete the enucleation and/or to morcellate the tissue from the bladder. A staged procedure is infrequently used unless the procedure seems to be exceptionally long because of a large gland or concomitant procedure such as cystolithotripsy, to avoid long lithotomy positioning for the elderly patient and potential fluid overload. The significant association between longer operative time and postoperative urethral stricture in the current study supports the consideration of staged procedures.
After a median follow-up of 7.6 years, 4.3% of our patients needed reoperation for relief of recurrent LUTS because of persistent or recurrent adenoma, BNC, or urethral stricture. This was consistent with the 5% previously reported after 5 years of follow-up. 7
Thirteen (1.1%) patients needed redo HoLEP in our series, which is comparable to that of open prostatectomy, 7,13 having the lowest reoperation rate among all surgical procedures for BPH. 22 Persistence or recurrence of adenoma after HoLEP may be because of the multinodular nature of the BPH, where few subcapsular nodules may consequently regrow and cause obstruction. In addition, the enucleation may not be complete in recurrent or previously operated cases because of altered tissue consistency previously observed, with consequent slower morcellation rates and higher energy needs. 23,24 This could explain the significant association detected between reoperated cases for recurrent adenomas and history of previous prostatic surgery. Despite the observation that morcellation time of the recurrent adenoma was significantly longer in our series, it did not keep its significance in the multivariate model.
Of interest, even though the size was still respectable in the current study (a mean of 62.4 cc), smaller prostate size was significantly associated with recurrence of adenoma. The smaller the gland size, the more likely we needed to reoperate in a small number of patients. This might be because the plane of enucleation in small glands is not always as obvious as in larger glands. TRUS determined prostate size is an opertator-dependent procedure and, hence, the more objective postoperative PSA reduction might represent a better surrogate for prostate size reduction after HoLEP. Patients who underwent redo HoLEP for recurrent adenoma had significantly lower mean percent of PSA reduction 3 months postoperatively, which might explain the impact of residual adenoma on further recurrence of obstruction after surgery. The Kaplan-Meier curve revealed a freedom from post-HoLEP reoperation of 97% at 5 years and 95% at 10 years, which represent a further proof of the the durability of HoLEP.
BNC and urethral stricture were detected in 3.2% of our patients at the most recent follow-up, which is consistent with that reported previously. 12, 25 –27 Considering that 71.4% of our patients in whom BNC developed had prostates smaller than 50 cc, those patients undergoing HoLEP for small glands may possibly need concomittant bladder neck incision. In a recent similar large series of more than 1000 patients, BNC and urethral stricture were detected in 16 (1.5%) and 24 (2.3%) patients, respectively, 21 where a positive correlation was observed between prostate size and postoperative BNC. Bladder neck incision was routinely performed in the latter study after HoLEP for glands smaller than 40 cc. Nevertheless, it has been reported previously that fewer patients with such small-size prostates needed recatheterization and reoperation after HoLEP than those undergoing holmium bladder neck incisions. 28
Meta-analysis confirmed that HoLEP was comparable to TURP in terms of postoperative urethral stricture (2.6% vs 4.4%) and reoperation (4.3% vs 8.8%). 29 Moreover, pooled data analysis of nine previous studies including 1847 patients showed that urethral stricture, BNC, and reoperation were, respectively, detected in 35 (1.9%), 27 (1.5%), and 33 (1.8%) patients at 12 months after HoLEP. 30 Variation in the technique and training level among different surgeons might have direct impact on the outcome of a given procedure.
The current study is not without limitations, considering its retrospective nature and the too small number of reoperated patients to show any significant differences in other parameters that might be associated with reoperation such as concomitant surgical procedures and energy used. Nevertheless, this large series of HoLEP, with its long follow-up, reflects the long-term safety and durability of the procedure and the overall low rate of reoperation.
Conclusion
In a single center large series, HoLEP has 95% reoperation-free probability at 10 years. The relatively small-size prostate may have an impact on recurrence of adenoma and bladder neck contracture, however. PSA reduction <50% after 3 months was significantly associated with recurrence of adenoma while longer operative time and postoperative catheterization were significantly associated with postoperative urethral stricture.
Footnotes
Author Disclosure Statement
No competing financial interests exist.