
Abstract
Purpose:
To compare perioperative outcomes, specifically hospital length of stay (LOS), after retroperitoneal and conventional transperitoneal robot-assisted partial nephrectomy (RAPN).
Patients and Methods:
We retrospectively compared consecutive patients with a posterior renal mass undergoing retroperitoneal RAPN (n=116) versus transperitoneal RAPN (n=97) at our institution between July 2007 and March 2014. The surgical approach was based on patient and tumor characteristics, history of abdominal surgery, and surgeon preference. The primary outcome was postoperative LOS, and secondary outcomes included complication rate, inpatient narcotic pain medication use, and inpatient antiemetic use.
Results:
Baseline patient and tumor characteristics were similar between groups. A significantly great proportion of patients undergoing retroperitoneal RAPN had LOS equal to 1 day (57% vs 10%, P<0.01). Complication rates were similar between groups (P=0.37). Median pain medication use was also similar between groups (P=0.85). A significantly greater proportion of retroperitoneal RAPN patients, however, needed no antiemetics postoperatively (59% vs 43%, P=0.02). On multivariate analysis, transperitoneal RAPN was a significant predictor of LOS greater than 1 day (odds ratio=7.4, P<0.01), when controlling for age, sex, body mass index, patient comorbidity, previous abdominal surgery, baseline kidney function, nephrometry score, and tumor size.
Conclusions:
For patients with posterior renal masses, retroperitoneal RAPN significantly reduces their hospital LOS when compared with transperitoneal RAPN.
Introduction
W
Although RAPN is typically performed via a transperitoneal approach to the kidney, some have argued that further improvements in perioperative outcomes can be made by using the retroperitoneal approach. 8 This is based in part on the results of previous studies of retroperitoneal laparoscopic renal surgery, which have demonstrated shorter operative times and hospital length of stay (LOS). 9 –11 In addition, early studies comparing transperitoneal and retroperitoneal RAPN have demonstrated shorter operative times with retroperitoneal RAPN, with equivalent estimated blood loss (EBL), postoperative pain, and complication rates. 12,13 These previous studies of retroperitoneal RAPN, however, did not examine LOS and are confounded by differences in tumor location between retroperitoneal and transperitoneal groups.
To better define the potential benefits of retroperitoneal RAPN, we examined the perioperative outcomes of retroperitoneal versus transperitoneal RAPN for posterior renal masses at our institution.
Patients and Methods
Study population
With Institutional Review Board approval, we retrospectively reviewed our database for RAPN performed between July 2007 and March 2014. We identified 213 consecutive patients (retroperitoneal n=116, transperitoneal n=97) who received RAPN for a posterior renal mass, based on the designation of “A” in the R.E.N.A.L. (radius; exophytic/endophytic; nearness; anterior/posterior; location) nephrometry score. 14 No patients were excluded from analysis. Both the retroperitoneal and transperitoneal approach were used by both surgeons (SBB and RSF), and the contribution of each approach was roughly equivalent between surgeons. The choice of surgical approach was based on surgeon preference, which included patient body habitus, history of abdominal surgery, and tumor size. The yearly distribution of posterior renal masses managed by retroperitoneal or transperitoneal RAPN is provided in Figure 1. As familiarity with retroperitoneal access increased, the use of retroperitoneal RAPN increased during the study period.
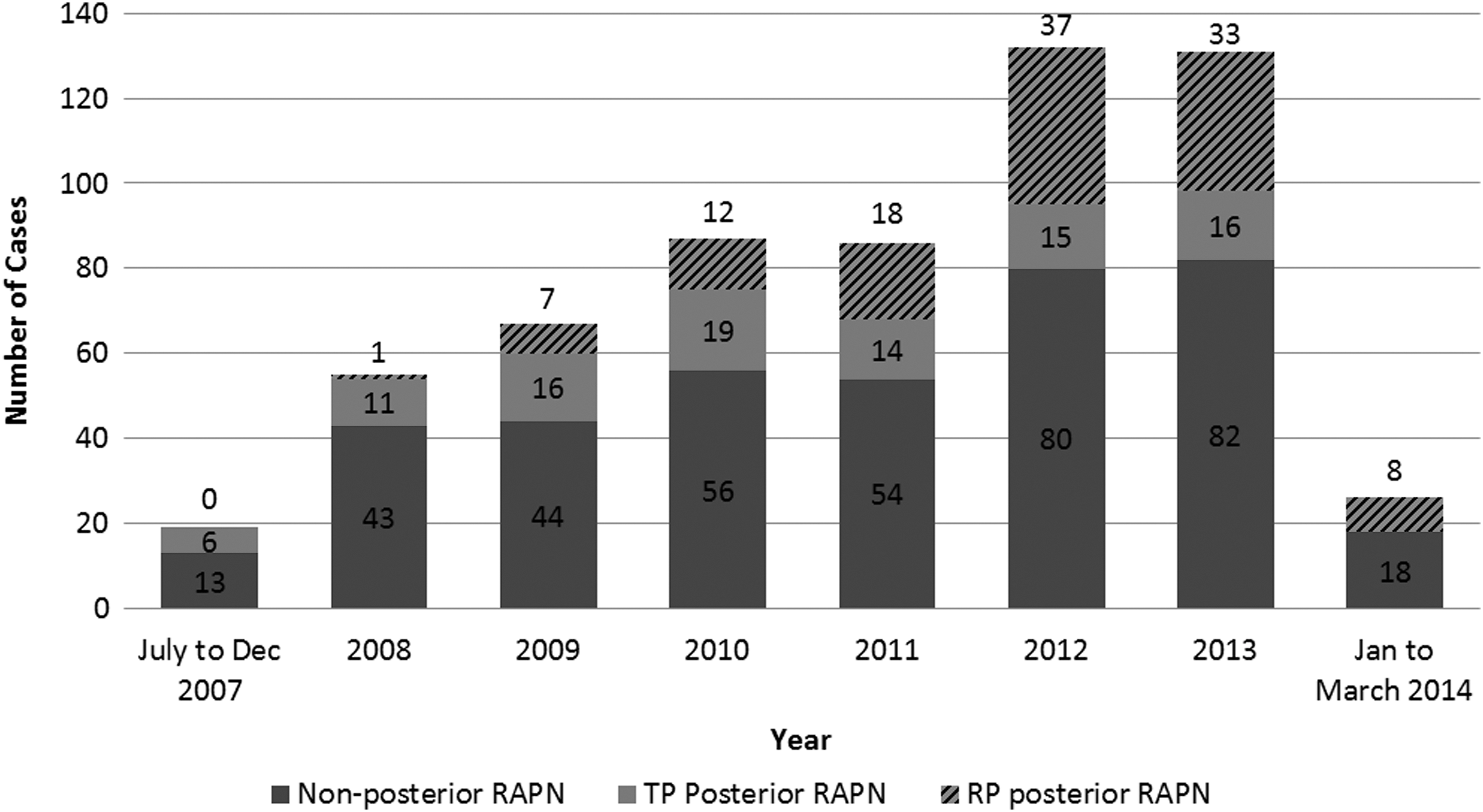
Distribution of robot-assisted partial nephrectomy (RAPN) cases during the study period, including (1) RAPN for nonposterior tumors (dark gray), (2) transperitoneal RAPN for posterior tumors (light gray), and (3) retroperitoneal RAPN for posterior tumors (dashed, light gray). TP=transperitoneal, RP=retroperitoneal.
Surgical technique
Transperitoneal approach
Our technique for both traditional clamped and off-clamp RAPN has been described previously. 15,16 A Veress needle is used to establish pneumoperitoneum, a 12-mm trocar (camera port) is placed lateral to the umbilicus, and two 8-mm trocars are placed in the midclavicular line—one inferior to the costal margin and one in the lower quadrant superior to the iliac crest. A 12-mm trocar (assistant port) is placed midline above the umbilicus. The robot is docked over the patient's shoulder along the line created by the camera port and renal hilum. The 30-degree downward lens, robotic scissors with monopolar cautery, and ProGrasp (Intuitive Surgical, Sunnyvale, CA) forceps are used. The bowel is reflected medially, the Gerota fascia is incised, the renal vessels are exposed and dissected circumferentially, and the kidney is mobilized. Perinephric fat is dissected to expose the tumor, and intraoperative ultrasonography is used to delineate tumor margins.
Retroperitoneal approach
Our technique for retroperitoneal RAPN is similar to that described by Hu and associates, 8 and our technique for retroperitoneal robotic access has been described previously. 17 Briefly, a skin incision is made 1 to 2 cm caudal to the tip of the 12th rib, blunt dissection is used to pierce through the lumbodorsal fascia, and blunt finger dissection is used to initiate creation of the retroperitoneal space. A 10-mm round preperitoneal dissection balloon (Covidien, Mansfield, MA) is inserted behind the kidney and fully inflated to complete creation of the retroperitoneal space. The balloon is removed, and a 12-mm trocar (camera port) is placed. The AirSeal system (SurgiQuest, Milford, CT) is used to prevent inadvertent loss of pneumoretroperitoneum. One 8-mm trocar is placed 1 to 2 cm caudal to the costovertebral angle, and once the peritoneum is bluntly dissected medially, another 8-mm trocar is placed in the anterior axillary line 1 cm caudal to the camera port. A 12-mm trocar (assistant port) is placed 2 cm medial to the anterior superior iliac spine. The robot is docked over the patient's forehead; the 0-degree lens, robotic scissors with monopolar cautery, and ProGrasp forceps are used. The Gerota fascia is incised, the kidney is mobilized, and the renal vessels are exposed and dissected circumferentially. Perinephric fat is dissected to expose the tumor, and intraoperative ultrasonography is used to delineate tumor margins.
Outcomes
Perioperative outcomes were recorded, including operative time, EBL, LOS, complications, and inpatient medication use. The primary outcome measure was LOS, which was calculated as the number of midnights spent in the hospital after surgery. Secondary outcomes included perioperative complication rates, inpatient narcotic pain medication requirement, and inpatient antiemetic requirement. Complications were classified by the Clavien-Dindo system, 18 with Clavien grade III or greater considered major complications. Narcotic pain medication use was converted to intravenous morphine equivalents for the analysis.
With the exception of patients experiencing complications necessitating higher levels of nursing care, patients were admitted to the urologic surgery inpatient floor postoperatively. All patients received the same postoperative admission order set, which included: (1) ambulation beginning on postoperative day 1, (2) liquid diet beginning on postoperative day 1, (3) standing oral acetaminophen 1000 mg four times daily (QID), (4) intravenous ketorolac 15 mg QID, (5) intravenous narcotic medications (morphine or dilaudid) as needed for breakthrough pain, (6) oral colace 100 mg twice daily, and (7) intravenous ondansetron 4 to 8 mg QID as needed for nausea. Narcotic pain medications were administered only when oral acetaminophen and intravenous ketorolac were not providing adequate pain control. All patients received some form of narcotic pain medication postoperatively. Not all patients received antiemetic medications postoperatively. Intravenous ondansetron was the first-line agent for postoperative nausea. Intravenous and rectal prochlorperazine, intravenous metoclopramide, and transdermal scopolamine were used in some patients as second-line agents. Once patients were tolerating a diet, intravenous narcotic pain medications were discontinued, and oral narcotic medications (hydrocodone or oxycodone) were ordered as needed. Discharge criteria included: (1) ability to ambulate without assistance, (2) tolerate a diet with evidence of return of bowel function, and (3) adequate pain control with oral medications.
Statistical analysis
All analyses were performed with SAS statistical software version 9.3 and R version 2.15.1. For univariate analysis, categorical variables were compared with the Fisher exact test, and continuous variables were compared with the Wilcoxon signed-rank test. Predictors of LOS were identified with multivariate logistic regression. LOS was considered a categorical variable for multivariate analysis, either equal to 1 day or greater than 1 day. Sensitivity analysis was performed controlling for surgeon, and no significant differences in study outcomes were noted. Predictors of increasing narcotic pain medication use were identified with multivariate linear regression, with morphine equivalents expressed as a continuous variable. Predictors of antiemetic use were identified with multivariate logistic regression. Antiemetic use was a categorical variable for this analysis—either no antiemetic use or any antiemetic use. Statistical significance was defined by P value less than 0.05 (two-tailed).
Results
Baseline characteristics are summarized in Table 1. Patient age, sex, history of abdominal surgery, baseline kidney function, tumor size, nephrometry score, and laterality did not significantly differ between retroperitoneal and transperitoneal RAPN groups. The proportion of patients considered obese, body mass index (BMI) greater than 30 kg/m2, was similar between groups (P=0.11). The distribution of patients with Charlson Comorbidity Index (CCI) equal to 0, 1, and 2 or greater was similar between groups (P=0.77).
RAPN=robot-assisted partial nephrectomy; SD=standard deviation; BMI=body mass index; CCI=Charlson Comorbidity Index; IQR=interquartile range; GFR=glomerular filtration rate.
Perioperative outcomes are summarized in Table 2. Operative time, EBL, and narcotic pain medication use did not significantly differ between RAPN approaches. The proportion of RAPN performed off-clamp was significantly higher in the retroperitoneal group (48% vs 13%, P<0.01). The proportion of retroperitoneal RAPN patients with LOS equal to 1 day was significantly higher (57% vs 10%, P<0.01). Proportion of patients not needing any antiemetics postoperatively was significantly greater for retroperitoneal RAPN (59% vs 43%, P=0.02). Complication rates were similar between groups (7% vs 10%, P=0.37), and major complication (Clavien III or greater) rates were similar as well (4% vs 7%, P=0.39). Specific complications are summarized in Table 3.
ICU=intensive care unit; POD=postoperative day; MI=myocardial infarction; DVT=deep venous thrombosis.
Predictors of LOS greater than 1 day are summarized in Table 4. Transperitoneal RAPN and increasing tumor size were significant and independent predictors of LOS greater than 1 day with odds ratio (OR) of 7.4 (P<0.01) and 1.6 (P=0.04), respectively.
Multivariate linear regression was performed to identify predictors of increasing inpatient narcotic pain medication requirement. Approach, nephrometry score, tumor size, laterality, clamped versus off-clamp technique, age, sex, BMI, CCI, baseline kidney function, previous abdominal surgery, and LOS were examined. Increasing tumor size (β=4.4, P=0.01), decreasing patient age (β = −0.61, P<0.01), and increasing LOS (β=20, P<0.01) were significantly associated with increasing narcotic pain medication use.
Multivariate logistic regression was performed to identify predictors of any postoperative antiemetic medication use. Approach, nephrometry score, tumor size, laterality, clamped versus off-clamp technique, age, sex, BMI, CCI, baseline kidney function, previous abdominal surgery, and LOS were examined. The only significant independent predictor of antiemetic use was transperitoneal RAPN (OR=2.3, P=0.04).
Discussion
We present what we believe to be the largest comparison of perioperative outcomes between retroperitoneal and transperitoneal RAPN. Previous studies have included potential confounding factors because of differences in tumor location between groups. 12,13 To reduce bias, because the retroperitoneal approach is ideally suited for posterior tumors, 8,19 we limited our study to only posterior renal masses. We found that for similar patients with posterior renal masses of similar size and nephrometry score, the average hospital LOS was significantly shorter (by nearly 1 day) after retroperitoneal RAPN. Furthermore, on multivariate analysis, the retroperitoneal approach was independently and significantly associated with LOS equal to 1 day. Although discharge criteria differ by institution and by surgeon, we use the same criteria for hospital discharge after RAPN for all patients. Given that return of bowel function and pain control are limiting factors to discharge, we examined postoperative narcotic pain medication and antiemetic use. Although postoperative narcotic medication use was nearly identical between retroperitoneal and transperitoneal groups, the patients who underwent retroperitoneal RAPN needed significantly less antiemetic medications, suggesting that an earlier return of satisfactory oral intake and bowel function were responsible for earlier hospital discharge.
Three previous studies comparing retroperitoneal and transperitoneal RAPN demonstrated improvements in perioperative outcomes for retroperitoneal RAPN. 12,13,20 In their small initial series of RAPN (n=26), Tanaka and associates 12 found a trend toward improved operative time with the retroperitoneal approach but were likely underpowered to demonstrate significant differences. In addition, only one patient in their transperitoneal group had a posterior tumor; therefore, their cohort did not represent those patients for whom a retroperitoneal approach is thought to be most beneficial. In a large single surgeon series of RAPN (n=107), Choo and colleagues 13 found significantly shorter operative times with retroperitoneal RAPN. A matched pair subset analysis was performed with 43 patients in each group (transperitoneal and retroperitoneal RAPN) matched for total nephrometry score. Tumor location, however, was not matched between groups with 8/43=19% of transperitoneal RAPN performed for posterior tumors and 6/43=14% of retroperitoneal RAPN performed for anterior tumors. In a multi-institutional series of RAPN from the United Kingdom (n=103), Hughes-Hallett and coworkers 20 found significant reductions in operative time, EBL, and LOS for retroperitoneal RAPN. As in the previously mentioned studies, the comparison between approaches is confounded: (1) only one of the three surgeons performed retroperitoneal RAPN, and (2) for the surgeon who performed retroperitoneal RAPN, no posterior tumors were managed by transperitoneal RAPN.
In the present study, we find that operative time and EBL were not significantly different between RAPN approaches. The proportion of off-clamp RAPN, however, was significantly higher for the retroperitoneal approach. Although off-clamp RAPN was increasingly used at our institution during the study period, we did not intend to preferentially apply off-clamp RAPN to retroperitoneal cases. Given that particularly in complex cases, blood loss during off-clamp RAPN is significantly higher than traditional clamped RAPN of similar tumors, 16,21 and the retroperitoneum provides a confined space capable of anatomic tamponade against bleeding, unrecognized biases may have led to higher off-clamp use for retroperitoneal RAPN. More importantly for the present study, higher use of off-clamp RAPN during retroperitoneal cases did not affect the primary and secondary study outcomes, because clamped versus off-clamp technique was included in all multivariate analyses with no significant relationship with greater LOS, narcotic pain medication use, or antiemetic medication use.
Mean hospital LOS was not reported by Tanaka and associateset 12 or Choo and colleagues. 13 Hughes-Hallett and coworkers 20 found a significant reduction in mean hospital LOS with retroperitoneal RAPN (2.5 vs 4.6 days, P<0.01). In our study of posterior renal masses, we also found a significant reduction in hospital LOS. With the increasing emphasis in reducing healthcare costs across medical and surgical specialties, the cost of robotic surgery has come under scrutiny. 22 As such, investigation of methods to reduce the financial costs of RAPN must be pursued, and a reduction in LOS represents one possibility. Also, with the aim of surgical evolution to reduce patient morbidity and mortality, reduction in hospital LOS represents a surrogate for reduced patient postoperative morbidity and improved convalescence. Because RAPN and LPN have provided a reduction in LOS compared with open partial nephrectomy, 4 retroperitoneal RAPN provides further reduction in LOS for patients with posterior renal masses compared with conventional transperitoneal RAPN. In our study, we demonstrate that the transperitoneal approach is an independent predictor of LOS greater than 1 day and, furthermore, the strongest predictor (Table 3).
In the present study, we also examined the impact of RAPN approach on postoperative inpatient medication use. We found that narcotic pain medication use was similar between groups. On multivariate analysis, increasing narcotic pain medication use was significantly associated with increased LOS, younger patient age, and larger tumor size. These associations are intuitive, because increased narcotic pain medication use may be associated with prolonged time to return of bowel function, elderly patients typically need less narcotic pain medication, and larger tumor size necessitates a larger extraction site and increased pain. Narcotic pain medication use may be reduced in patients who receive intraoperative or perioperative local anesthetic. Given that the total number and size of incisions for retroperitoneal and transperitoneal RAPN are not significantly different, we did not record the use of local anesthetic agents because it would not be expected to disproportionately affect one group.
Because intraperitoneal surgery is a risk factor for postoperative nausea and vomiting, 23 we hypothesized that antiemetic medication use would be increased in the transperitoneal RAPN group. In fact, we found that a significantly higher proportion of patients receiving transperitoneal RAPN needed postoperative antiemetics (55/97=57%) compared with retroperitoneal RAPN (47/116=41%). Furthermore, on multivariate analysis, transperitoneal RAPN was the only variable independently predictive of an antiemetic requirement after the surgical procedure. Given that recovery of bowel function is a major barrier to discharge after RAPN at our institution, this reduction in postoperative nausea evidenced by decreased antiemetic use may be the causal link to decreased LOS seen with retroperitoneal RAPN. Although antiemetic use was a secondary analysis in the present study, future prospective studies comparing transperitoneal with retroperitoneal RAPN may consider focusing on postoperative nausea and time to recovery of bowel function.
Our study is not without limitations. The retrospective nature of our study allows for potential sources of bias that cannot be eliminated. As a result of restricting our comparison of RAPN approach to posterior tumors, to reduce confounding from differences in tumor characteristics between treatment groups, the outcomes of this study are not generalizable to all patients undergoing RAPN. Because patients with posterior tumors were not randomly allocated to treatment groups, a potential selection bias exists for which patients underwent retroperitoneal RAPN. In addition, because the proportion of patients receiving retroperitoneal RAPN increased with time, the retroperitoneal RAPN results may represent more contemporary outcomes compared with transperitoneal RAPN. Finally, our single-institution experience allows for standardization of discharge criteria and details on postoperative inpatient medication use; however, the results may not be applicable to patients treated at low-volume, nonacademic centers.
Conclusions
For patients with posterior renal masses undergoing RAPN, the retroperitoneal approach is associated with a significantly reduced hospital LOS compared with the conventional transperitoneal approach. When controlling for preoperative patient and tumor characteristics, retroperitoneal RAPN was the strongest independent predictor of hospital LOS equal to 1 day. One factor responsible for this improvement in hospital LOS may be the significant reduction in postoperative antiemetic medication requirement seen with retroperitoneal RAPN.
Footnotes
Acknowledgment
Joel M. Vetter provided assistance with statistical analysis for this study.
Author Disclosure Statement
No competing financial interests exist.