
Abstract
Introduction:
Semirigid and flexible ureterorenoscopy (URS) procedures are safe and efficient treatment options for urolithiasis of all localizations. Sometimes, a Double-J stent is placed in preparation of definitive treatment. The aim of our study was to evaluate the influence of prestenting on the outcome of URS.
Patients and Methods:
We retrospectively analyzed 565 patients of our prospective, multicenter multinational database who underwent URS for renal or ureteral stones from June 2011 to December 2013. Demographic and stone-related data, surgery time, stone clearance, and complications were evaluated. Statistical analysis was performed comparing the prestented and nonstented groups.
Results:
Demographic data, stone size, and localization were comparable in both groups. Three hundred twenty-three patients were prestented and 242 nonstented. Overall, prestenting had significant influence on the stone-free rate (SFR) (86% prestented vs 74% not prestented, p = 0.0003) and complication rate (6.5% vs 14.5%, p = 0.003), but not on surgery time (55 ± 36 minutes vs 61 ± 35 minutes, p = 0.071). Subgrouped, this was also true for renal stones (83% vs 60%, p = 0.0001, odds ratio [OR] 3.15; confidence interval, CI [1.77, 5.62]/8.7% vs 19.4%, p = 0.02, 0.39 [CI 0.19, 0.83]). For ureteral stones, there was no significant influence on SFR (94% vs 90%, p = 0.4, OR 1.63 [CI 0.63, 4.22]), but significantly more complications (3.1% vs 10.7%, p = 0.02, OR 0.27 [CI 0.08, 0.86]) in the nonstented group.
Conclusion:
Prestenting positively affects safety and efficacy of URS. This is more pronounced in the treatment of kidney stones compared with ureteral stones. Although the SFR for ureteral stones is comparable without prestenting, the complication rate is higher.
Introduction
T
The increasing use of URS can be attributed to the high efficacy of the procedure with high stone-free rates (SFRs) and a concomitant low complication rate, as well as practically no contraindications. 4 This was made possible by the invention of better ureterorenoscopes with smaller diameters, better visualization, and higher active deflection in case of flexible ureterorenoscopes.
Preoperative placement of a Double-J stent (due to management of acute renal colic or as preparation of definitive treatment) is sometimes considered to facilitate the procedure. There is conflicting evidence in the literature regarding this issue. Some mostly smaller studies support the idea of prestenting at least in selected cases. 5 –13 On the other hand, there are a few studies evaluating emergency URS without prestenting and with good results. 14 –18 The aim of this study was to analyze the influence of prestenting on safety and efficacy of URS in our own multinational multicenter experience.
Patients and Methods
We retrospectively analyzed 565 URS procedures for renal or ureteral stones, from June 2011 to December 2013, of our prospective multicenter multinational database. Tertiary care centers from Stockholm (Sweden), Barcelona (Spain), Lillebaelt (Denmark), Patras (Greece), Sindelfingen (Germany), and Torino (Italy) participated in the project called International Collaboration in Endourology (UROICE) and contributed to the database. This is a multisurgeon study with more than one surgeon per center and also includes urologists in training.
All patients were evaluated routinely with urinalysis and blood tests. For the procedures classified as prestented, a Double-J insertion was performed before definitive stone treatment. Normally, the stents were placed 1–2 weeks before surgery. Different stents were used according to the local protocol of the participating centers, with the majority being 7F. Patients with urinary tract infection received antibiotic treatment before surgery, and most of the other patients received perioperative antibiotic prophylaxis. The procedures were performed in general anesthesia (or spinal anesthesia if there were contraindications for general anesthesia) and lithotomy position. Modern fiber-optic or digital flexible ureterorenoscopes (Flex X2, Storz; FlexXC, Storz; URS-P5, Olympus; URF-V, Olympus; Viper, Wolf), Ho:YAG laser, and nitinol baskets were used for treatment of renal stones. Ureteral calculi were treated by the use of semirigid or flexible ureterorenoscopes, Ho:YAG laser and forceps, or nitinol basket. A ureteral access sheath (UAS) was placed at the surgeon's discretion. Some of the centers used the UAS for treatment of ureteral calculi, while some did not. If considered and needed, a Double-J stent was placed at the end of the procedure. Demographic, stone, and surgery-related data were introduced in the database prospectively by the surgeon who did the procedure. An online secured front end was used for this purpose. Stone-free status was defined as no residual stones of any size and evaluated at the end of the procedure by endoscopic and radiologic control. The patients were followed routinely by ultrasound. Selected cases, which were in doubt of having residual fragments, received a CT scan. Follow-up data were introduced by each department after the treatment.
The R project for statistical computing, R 3.02 (R Foundation for Statistical Computing, Vienna, Austria;
Results
Overall, demographic data, stone size, and localization were comparable in both groups (Table 1). The distributions of demographic parameters differed comparing the contributing centers. Three hundred twenty-three patients were prestented and 242 nonstented. Of the prestented procedures, 69 were performed in anticipation of definitive stone treatment, while 254 were done primarily for immediate treatment of hydronephrosis and/or infection. UAS was used in 223 of 565 procedures. The use of UAS was more common in the nonprestented group (110 of 132 procedures vs 113 of 210, p = 0.015). Of the prestented patients, 298 received a Double-J stent postoperatively, 19 a temporary ureteral catheter, which was attached to the bladder catheter and removed after 1 or 2 days, and 6 no stent, while 209 of the not prestented patients received a Double-J stent, 16 a temporary ureteral catheter, and 17 no stent (p = 0.008).
ASA = grading of patients for surgical procedures according to American Society of Anesthesiologists; BMI = body mass index; UAS = ureteral access sheath.
The results and univariate analysis are shown in Table 2. In the overall group, which included both kidney or ureter stones, as well as both of them, prestenting had significant influence on the SFR (p = 0.0003) and complication rate (p = 0.003), but not on OR-time (p = 0.071). The complications consisted mainly of infections and Double-J stent changes due to displacement or occlusion from blood clots (Table 3). No major complications occurred. SFR and OR-time differed significantly between the contributing centers (p < 0.001), while there was no significant difference regarding complications.
Bold indicates significant differences.
In multifactorial analysis, the influence of prestenting on URS regarding SFR (p = 0.002) and complications (p = 0.002) was confirmed. The final model for SFR included stone size, prestented status, center, and UAS. For complications, backward selection removed every variable except prestented status. OR-time was not significantly influenced by the prestenting status and this parameter was removed by backward model selection for the resulting final model that included stone size, center, gender, age, and UAS.
Kidney stones only
Subgrouped for renal calculi, prestenting had significant influence on SFR and complication rate, but not on OR-time (p < 0.001, 0.021, and 0.5, respectively). Notably, there was no significant difference in stone size in the groups (p = 0.336). The odds of becoming stone free vs not becoming stone free were 4.77 in the prestented kidney stone group and 1.51 in the nonstented kidney stone group with a highly significant difference in the OR-test. The OR of 3.15 [confidence interval, CI 1.77, 5.62] showed a strong positive association of being prestented and becoming stone free (see also Fig. 1). The odds of having complications vs not having complications were 0.1 in the prestented group and 0.24 in the nonstented group (p = 0.02 in the OR-test). The OR was 0.39 [CI 0.19, 0.83], showing a significant negative association between being prestented and having complications (see also Fig. 2). Multifactorial analysis confirmed the influence of prestenting on SFR and complication rate, but not on OR-time (p < 0.001, 0.005, and n.s., respectively). The final models included stone size, prestented status, and center for SFR; prestented status and UAS for complications; and stone size, gender, center, and UAS for OR-time.
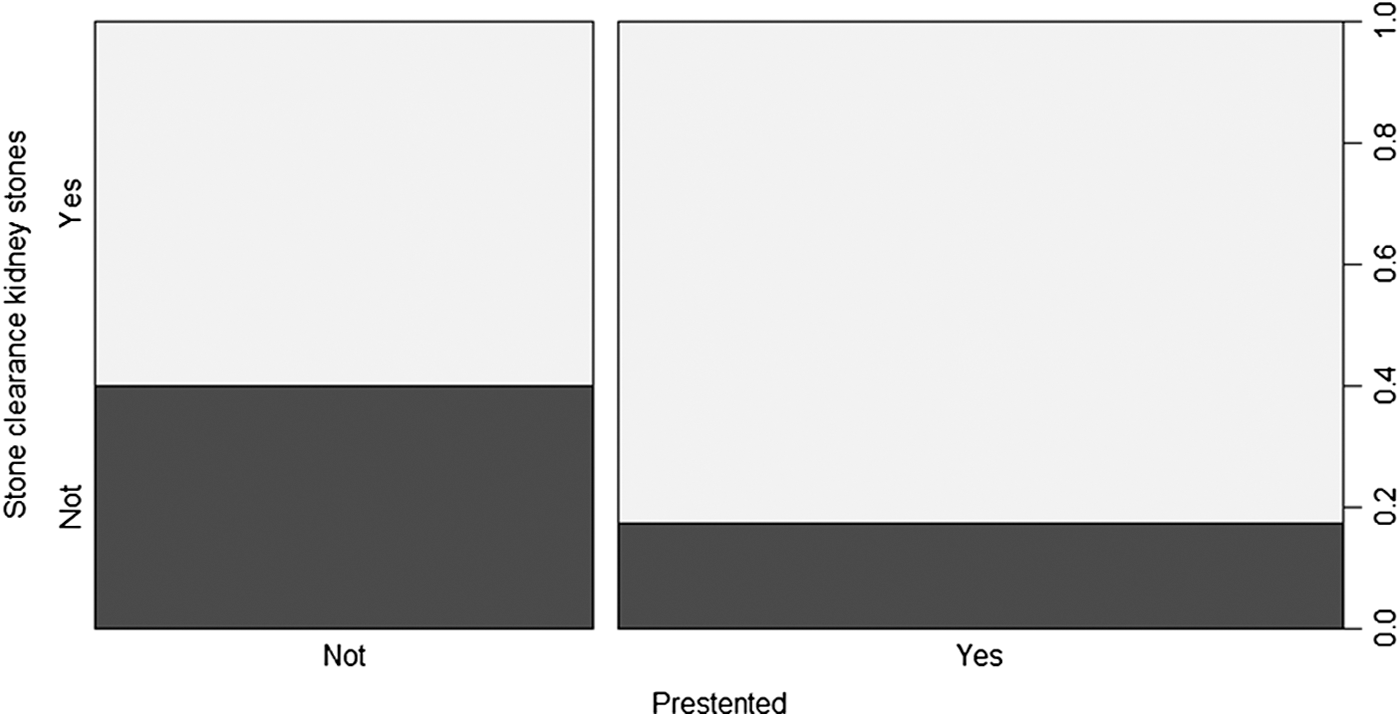
Stone-free rate for kidney stones depending on prestented status.
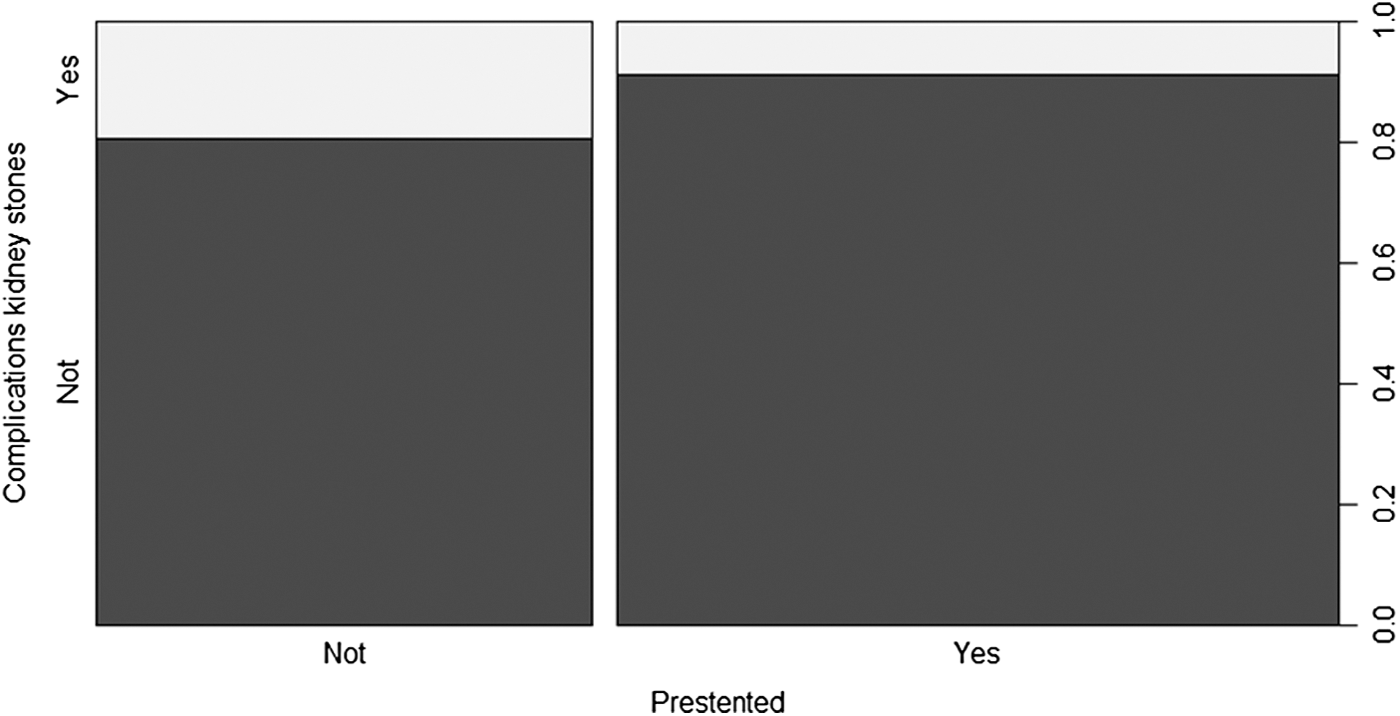
Complication rate for kidney stones depending on prestented status.
Ureter stones only
For ureteral stones, there was no significant influence of prestenting on the SFR (p = 0.4), but significantly more complications (p = 0.021) and longer OR-times (p = 0.015) in the nonstented group. There was also no difference in the groups regarding stone size (p = 0.4). The odds of becoming stone free vs not becoming stone free were 9.18 in the prestented ureteral stone group and 15 in the nonstented ureteral stone group, with no significant difference in the OR-test. The OR was 1.63 [CI 0.63, 4.22]. The odds of having complications vs not having complications were 0.03 in the prestented group and 0.12 in the nonstented group (p = 0.03 in the OR-test). The OR was 0.27 [CI 0.08, 0.86], showing a significant negative association between being prestented and having complications.
Multifactorial analysis did not confirm the influence of prestenting on OR-time. Prestenting status was removed from the final model, which included stone size, center, gender, and UAS. The results for complications (p = 0.03) and SFR (n.s.) were in line with univariate findings. For SFR, the prestented status was removed by model selection as it had no benefit for the explanatory model.
Discussion
In the Clinical Research Office of the Endourological Society (CROES) URS global study, nearly 20% of patients treated were prestented. 4 The habit of prestenting patients before URS might differ significantly depending on the treating center. There is evidence in the literature showing a trend toward a better outcome of URS after prestenting. The published studies are mainly retrospective series with small or no control group. An overview of these studies is given in Table 4. The better results for the prestented patients did not reach statistical significance in all comparative studies. Furthermore, in some studies, the benefit of prestenting was only shown for special circumstances. Netsch et al. performed a matched-pair analysis of 143 prestented vs 143 not prestented URS procedures for ureteral and renal stones and noted an increased SFR due to prestenting in treatment of calculi >5 mm, while in case of calculi <5 mm, no influence of prestenting was found. 9 Lumma and colleagues retrospectively compared 64 not prestented URS procedures with 486 prestented procedures and found a positive influence of prestenting only for proximal stone locations, but not for distal ureteral calculi. 8 No author recommended a routine stenting before URS.
SFR = stone-free rate; URS = ureterorenoscopy.
For ureteral stones, the literature provides some series on emergency URS procedures, which are not prestented by definition. 14 –18 The authors of these series examined the concept of undelayed URS in a time frame of 24–48 hours after the first colic. The published overall SFRs reach ∼90% or even higher in case of distal calculi with concomitant low complication rates. These good results support a nonstented approach for ureteral calculi.
To our knowledge, this is the largest series and also the first multicenter study published on the topic of prestenting before URS. It includes breakdowns for ureteral as well as kidney stones and aims to describe not only a possible difference but also how strong the association is.
The overall SFR of 81% in our series is in line with previous published results and only slightly lower than in the CROES study. 4 This is explainable by a higher percentage of kidney stones in our series. Our results clearly show a strong benefit of prestenting on therapy success of URS for kidney stones in terms of higher SFR (OR 3.15 [CI 1.77, 5.62]) and lower complication rate (OR 0.39 [CI 0.19, 0.83]), in both univariate and multifactorial analyses. A possible explanation for these findings is the passive dilation and paralysis of the ureter due to the indwelling stent. 19 Although this was not tested, we hypothesize that the adynamic ureter may result in an easier placement of the UAS and easier movement of the ureterorenoscope up and down. This may lead to more flexibility and finally a higher SFR. Additionally, an adynamic system may result in a higher volume of the upper tract and an improved flow alongside the ureterorenoscope or the UAS to the bladder and therefore better irrigation, better visual conditions, and a higher SFR.
Our findings of a higher SFR after prestenting for kidney stones are in line with previous published results. 5,8,9,12,13 A lower complication rate after prestenting was previously described by Lumma et al. 8 for renal and proximal ureteral localizations, but was not found for renal localizations by Mueller and colleagues. 13 A possible explanation is the lower number of procedures for kidney stones in this series (n = 91). Rubenstein and colleagues 5 and Netsch and colleagues 9 reported an overall complication rate, but did not include a subgroup analysis for kidney stones. Overall, they found no influence of prestenting on the complication rate with only few cases with complications. The other studies on prestenting did not report a statistical analysis regarding complications. Only Chu et al. 10 mentioned a significantly longer OR-time specifically for stones larger than 1 cm, but without differentiating between ureteral and renal stones.
For ureteral stones, we did not find a significant benefit in terms of higher SFR, but the complication rate (OR 0.27 [CI 0.08, 0.86]) was higher if the patient was not prestented. These results contradict those published by Lumma and colleagues. 8 They subgrouped their data into distal ureteral calculi and all other calculi more proximal (including proximal ureter stones and kidney stones) and reported a higher SFR and lower complications in the prestented group for all proximal, but not for distal, localizations without giving statistical tests. We performed a subgrouping into ureteral and renal stones in contrast as this normally coincides with the use of semirigid and flexible ureterorenoscopes in our practice. Therefore, an overlap for proximal ureter stones explains the differences. Mueller and colleagues 13 also performed a subanalysis for ureteral stones and found statistically significant lower complications and a higher SFR if the patient was prestented. The latter was not reproducible in our series and is also in conflict with published series on emergency URS.
Univariate analysis showed a significant difference for OR-time between the prestented and nonstented URS procedures for ureteral stones, but this was not confirmed by multifactorial analysis. This is explainable by a confounding with participating centers. Netsch et al. 9 also did not find an influence of prestenting on OR-time.
Prestenting did not result in fewer patients requiring a stent postoperatively. On the contrary, more patients who were prestented also received a stent at the end of stone treatment. This might be explainable by a tendency of some surgeons/centers to play it safe, which manifested before and after the procedure.
The outlined benefits of prestenting on success rates of URS have to be weighed up against the additional morbidity caused by the indwelling Double-J stent. Although this was not part of our study, multiple publications show that as much as 80% of stented patients suffer from various symptoms, including pain, voiding and storage symptoms, sexual dysfunction, and decrease in general health perception and work performance. 20 –22 Furthermore, prestenting requires an additional procedure with its own risks.
This study has some limitations that need to be considered. The foremost is its retrospective and uncontrolled nature. As this was not a randomized trial, the results are prone to influence by treatment bias. There is some heterogeneity in the protocols of the contributing centers regarding intraoperative technique and equipment such as the use of a UAS for proximal ureter stones. Differences between the centers might have influenced the results. On the other hand, this reflects the various approaches utilized in different clinical settings and thereby allows for a better generalization of the results.
In addition, we did not analyze the impact of the duration of prestenting on the outcome. Like in the already published literature, we were not able to present data about the time a Double-J stent should be left in the ureter to gain the mentioned benefits. Further evaluation of this topic would be desirable.
Conclusions
URS is a safe and efficient treatment option for urinary stones of all localizations, whether the patient was prestented or not. OR-time was not influenced by prestenting. For kidney stones, prestenting is an excellent concept to improve SFR and lower the complication rate. We could not find a significant influence of prestenting on SFR for URS of ureteral stones, but without prestenting, the complication rate was higher. These findings need to be weighed up against Doube-J stent-related complications as well as discomfort and reduction in quality of life, which were not part of this study.
Footnotes
Author Disclosure Statement
No competing financial interests exist.