
Abstract
Purpose:
To compare the Guy and Clinical Research Office of the Endourological Society (CROES) scoring systems in predicting postpercutaneous nephrolithotomy (PCNL) stone-free rate and complications.
Patients and Methods:
A total of 437 patients who underwent PCNL for renal stones were included in the recent retrospective study. All stones were evaluated with CT preoperatively. Mean stone diameter was 701.52±510.65 mm2. Guy and CROES nephrolithometry scores were calculated for each patient, and their correlation with stone-free status, operative and fluoroscopy time, and length of hospital stay was evaluated. Post-PCNL stone status was evaluated with plain radiography of the kidneys, ureters, and bladder. Postoperative complications were graded according to the modified Clavien classification, and the correlation of both scoring systems with postoperative complications was also investigated.
Results:
The mean Guy grade was 2.28±1.12, and the mean CROES score was 196.92±65.89. The overall stone-free rate was 75.1%. There was a significant correlation between the Guy stone score (GSS) and CROES score and stone-free status (P<0.001, P<0.001). Also, both scoring systems were correlated with operative time (P<0.001, P<0.001) and length of hospital stay (P=0.002, P=0.01). The overall complication rate was 34.6%, with most being modified Clavien grade I and grade II. Both scoring systems were significantly correlated with complication rates. Regression analysis showed that both scoring systems were significantly associated with stone-free rates, estimated blood loss (EBL) (>250 mL), and operative time.
Conclusion:
Both GSS and CROES nomograms had comparable accuracies in predicting post-PCNL stone-free status. Different from the previous reports, our results showed that both nomograms were predictive of overall complications, EBL, and operative time.
Introduction
S
Later, in 2013, Smith and associates 4 on behalf of the Clinical Research Office of the Endourological Society (CROES) PCNL Study Group proposed a new nephrolithometric nomogram using patient factors besides preoperative radiologic findings. 4 In this nomogram, all variables correspond to a numeric value including the case volume per year, unlike expert based scores used in GSS. In the recent study, we aimed to compare the Guy and CROES scoring systems in predicting post-PCNL stone-free rate and complications.
Patients and Methods
A total of 437 patients who underwent PCNL for renal stones between May 2012 and January 2015 were included in the recent study. This study was conducted retrospectively. The data were driven from the electronic medical records of the patients. Seventy-one of the patients underwent repeated PCNL for recurrent stones on the ipsilateral kidney. Twenty-seven of the patients had a nephrostomy tube in the ipsilateral kidney. Study exclusion criteria included age less than 18 years, no available preoperative CT imaging, and use of CT imaging for post-PCNL stone status. The patients who had been evaluated with noncontrast CT were excluded from the study to avoid a possible bias that can be caused by higher sensitivity of CT for detecting residual fragments after PCNL.
All procedures were performed in a tertiary referral center by two experienced endourologists (IHB and TD). All stones were evaluated with CT preoperatively. All PCNLs were performed under general anesthesia with the patient in the prone position. Fluoroscopy was used for access guidance and Amplatz dilators used for dilation. Fluoroscopy time was measured for the entire procedure beginning from access to nephrostomy tube placement. A 14F nephrostomy tube was inserted at the end of the procedure. The operative time was measured after the patient was turned to the prone position. The patients' demographic characteristics, stone burden, number of tracts and location, operative time, fluoroscopy time, presence of residual stones, and estimated blood loss (EBL) were recorded prospectively in all patients postoperatively.
At the 1-month follow-up visit, patients were evaluated with plain kidneys-ureters-bladder (KUB) radiography. Patients with asymptomatic residual fragments <4 mm were accepted as stone free. In our institution, KUB radiography is used for routine evaluation of post-PCNL stone status, because of the cost. CT is reserved for only symptomatic patients, radiolucent stones, and/or suspicion of residual fragments seen on KUB radiography.
Guy and CROES nephrolithometry scores were calculated for each patient, and their correlation with stone-free status, operative and fluoroscopy time and length of hospital stay (LOS) was evaluated. Patients were categorized into four grades (grades I. II. III, IV) according to the GSS as described previously 3 and into four grades according to the CROES nephrolithometry score (grade 1: 0–100, grade 2: 101–150, grade 3: 151–200, grade 4: 201–350). Postoperative complications were graded according to the modified Clavien classification, 7 and the correlation of both scoring systems with postoperative complications was also evaluated.
Statistical analyses were performed with the Statistical Package of Social Sciences version 21 (SPSS, Chicago, IL). Categoric variables were presented as numbers and percentages and compared with the chi-square test. Continuous variables were presented as means and standard deviations and compared with an independent sample t test. Correlation analyses were evaluated using the Pearson correlation coefficient (r).
Linear and logistic regression analyses were used to examine the possible association between both the Guy and CROES scoring systems and stone free status, blood loss, operative time, LOS, and fluoroscopy time. Receiver operating characteristic (ROC) curves were generated to assess the predictive role of both scoring systems on the stone-free rate. The Youden index method was used to find a cutoff value for the CROES score to predict stone-free status.
Results
The demographic and perioperative characteristics of the patients are summarized in Table 1. The mean GSS grade was 2.28±1.12, and the mean CROES score was 196.92±65.89. The overall stone-free rate was 75.1%. Stone-free patients had significantly lower stone burden (P<0.001), shorter operative time (P=0.005), shorter LOS (P=0.006), lower GSS grade (P<0.001), and higher CROES score (P<0.001).
SD=standard deviation; BMI=body mass index; CROES=Clinical Research Office of the Endourological Society.
There was a positive correlation between the GSS grade and operative time (r=0.20, P<0.001) and LOS (r=0.15, P=0.002). There was a negative correlation between the GSS grade and stone-free status (r = −0.38, P<0.001). There was a positive correlation between the CROES score and stone-free status (r=0.42, P<0.001) (Table 2). There was a negative correlation between the CROES score and operative time (r = −0.24, P<0.001) and length of hospital stay (r = −0.15, P=0.01).
Chi-square test.
Of the 437 patients, postoperative fever developed in 77, 38 needed blood transfusion, 7 experienced sepsis, 2 had pneumothorax, 1 had colon injury, and 1 had arteriovenous fistula. The overall complication rate was 34.6%, with most modified Clavien grade I and grade II (Table 1). Both scoring systems were significantly correlated with complication rates (Table 2).
Regression analysis showed that both scoring systems were significantly associated with stone-free rates, EBL (>250 mL), and operative time. Regression analysis revealed no significant association between both scoring systems and fluoroscopy time and LOS (Table 3).
95% CI of odds ratios (logistic regression analysis).
95% CI of B coefficient (linear regression analysis).
CI=confidence interval; EBL=estimated blood loss; N/A=not available.
ROC analysis revealed area under curve of 0.26 (95% confidence interval [CI] 0.207–0.311) and 0.77 (95% CI 0.73–0.82) for the Guy and CROES nephrolithometry scoring systems, respectively (Fig. 1). Cutoff value for the CROES score to predict stone-free status was 171.50.
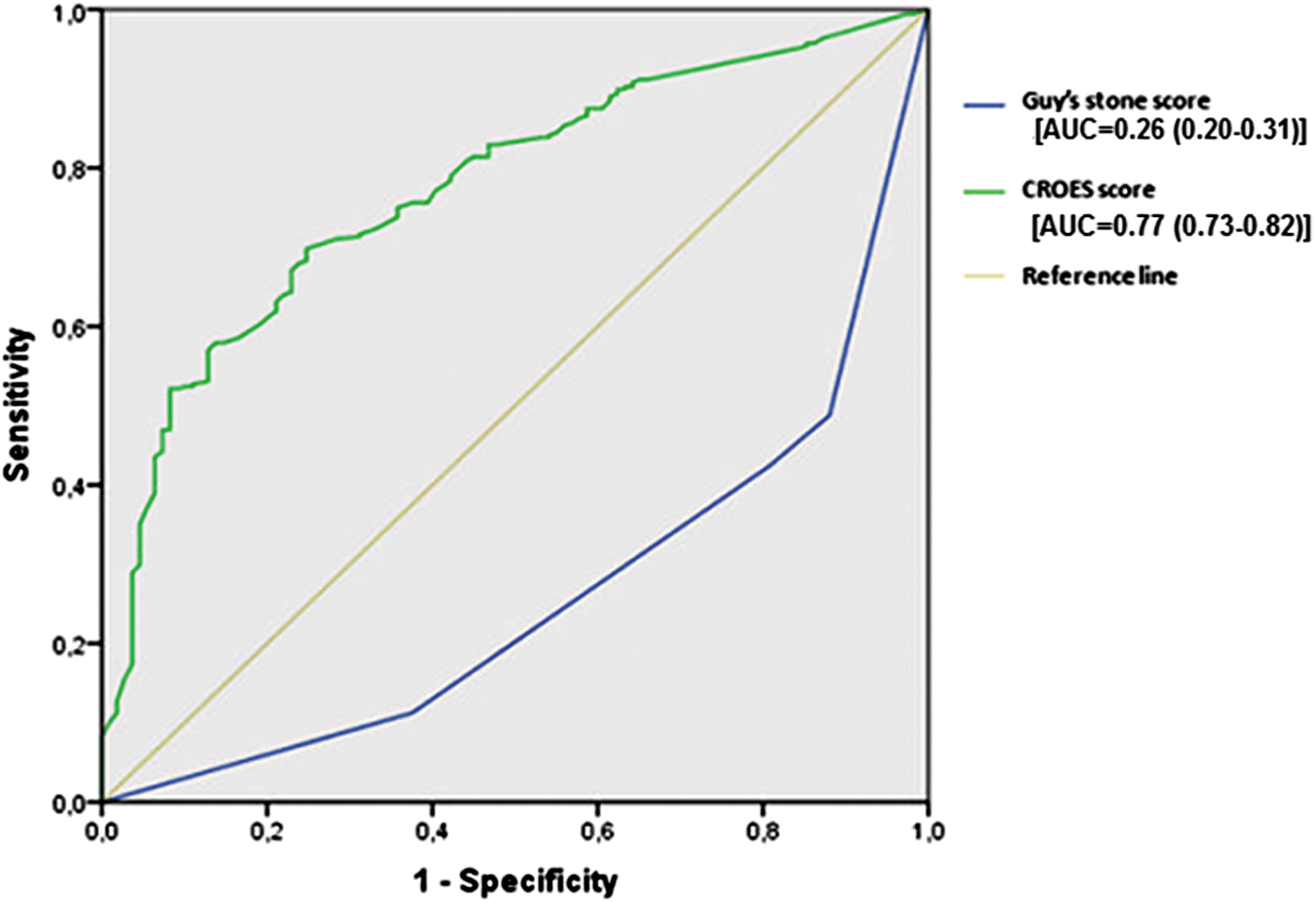
Receiver operating characteristic curves for both scoring systems in predicting stone free status. AUC=area under the curve; CROES=Clinical Research Office of the Endourological Society.
Discussion
It is possible to estimate the postoperative stone-free status of a patient using preoperative imaging characteristics. 8 –10 To standardize the terminology about complexity of the stones and to aid proper preoperative counseling of the patients, some authors developed different scoring systems. 3 –5 The ideal nephrolithometry index should be easy to perform in daily practice, include the patient characteristics besides preoperative imaging characteristics, and also should be affected by surgeon experience.
There is no universally accepted ideal scoring system yet. To support further studies intending to develop the ideal scoring system, comparison of the recent scoring systems are very important to show the strength and weakness of these systems. In the recent study, we aimed to evaluate the Guy and CROES scoring systems for predicting the PCNL stone-free status and complications. To the best of our knowledge, the current study is the first single center study with the largest sample size comparing these two widely accepted and used scoring systems for predicting post-PCNL outcomes.
In the current study, both scoring systems were significantly associated with stone-free rates (P<0.001 and P<0.001), EBL (>250 mL) (P=0.007 and P=0.003), and operative time (P=0.035 and P<0.001). Our results in terms of GSS were consistent with previous reports. 3,6,11 –13 The original study by Thomas and colleagues 3 and two validation studies performed by Ingimarsson and coworkers 6 and Mandal and associates 14 demonstrated that GSS was significantly associated with stone-free status. In addition, Labadie and colleagues 12 reported that GSS was significantly associated with EBL and LOS.
Vicentini and coworkers 11 reviewed 155 PCNLs and concluded that GSS was significantly associated with operative time and blood transfusion rates. In the study, both scoring systems were significantly associated with post-PCNL complications (P<0.001 and P<0.001). Noureldin and associates 13 did not find any association between GSS and post-PCNL complications, and they proposed that this might be because of the lower number of patients who underwent supine PCNL and because of relatively lower complication rates. Although our complication rates were similar to that of Noureldin and colleagues 13 and all PCNLs were performed in the prone position, our results were consistent with those of Vicentini and associates 11 and Mandal and coworkers 14 who have reported significant association between GSS and post-PCNL complications.
CROES nephrolithometric nomogram uses patient factors besides preoperative imaging findings for prediction analysis. Smith and colleagues 4 reported that the nomogram fits best at stone-free rates between 70% and 90%, but showed lower performance in the lower stone-free rate ranges, although still significant. In the recent study, we found a cutoff value of 171.50 for the CROES score to predict stone-free status. This cutoff value corresponds to an 81% chance of the stone-free rate consistent with the values reported in the original study. 4 External validation studies of CROES nephrolithometric nomogram has not been performed yet.
The original studies by Smith and associates 4 and Labadie and coworkers 12 demonstrated that the CROES nomogram was significantly associated with post-PCNL stone-free status. In the recent study, the CROES nomogram was found to be associated with operative time and LOS, unlike the study of Labadie and coworkers, 12 which reported lack of association between the CROES nomogram and EBL or LOS.
Although CT has been proposed as the most optimal imaging modality after PCNL, there is still some argument about the choice of imaging after PCNL, especially about the cost. 15,16 There is evidence to support that residual fragments smaller than 2 mm should probably be considered as clinically insignificant, whereas fragments larger than 3 to 4 mm are more likely to cause a stone-related event that may need some kind of surgical intervention. 17
A recent review by Sountoulides and associates 17 concluded that routine CT imaging after PCNL might be omitted and replaced by routine follow-up with KUB radiography in asymptomatic patients with radiopaque, nonstruvite stones. The post-PCNL follow-up was performed with KUB radiography in the original studies of both the Guy and CROES nomograms. 3,4 Both nomograms were also validated with the use of postoperative CT and rigorous stone-free criteria (<2 mm) at follow-up. 6,12
It was reported that the optimal time to perform imaging after PCNL is at the end of 1 month, because earlier imaging may produce false-positive results from inconsequential dust and may detect residual fragments that pass spontaneously during the immediate postoperative period. 18 In the recent study, we used KUB radiography at the 1 month visit for routine post-PCNL follow-up, as in the original studies.
After the emergence of different nomograms for predicting post-PCNL outcomes, some comparative studies were designed to investigate whether one nomogram has superiority to the other. Noureldin and coworkers 13 compared the GSS and S.T.O.N.E. nephrolithometry scoring systems in 185 PCNLs. They concluded that both scoring systems have comparable accuracies in predicting post-PCNL stone-free status. In another multicentric study, Labadie and associates 12 compared GSS, S.T.O.N.E., and CROES nephrolithometry nomograms in 246 patients. In this study, the patients who had previous ipsilateral renal surgery were excluded from the study, except the patients who underwent PCNL.
Although previous renal surgery is one of the parameters affecting the CROES score, this does not affect the Guy and S.T.O.N.E. scores. Thus, the exclusion of these patients might possibly cause a selection bias. Authors concluded that the GSS, S.T.O.N.E., and CROES nephrolithometry nomograms were equally predictive for the post-PCNL stone-free rates. They reported that although GSS and S.T.O.N.E. nephrolithometry were associated with EBL and LOS, the CROES nomogram was not predictive of complications, EBL, or LOS.
The recent study is the largest one that was conducted in a single tertiary center. In our opinion, scoring systems are useful for academic purposes to standardize the reporting of postoperative outcomes across different series. Although both scoring systems equally predict the postoperative outcomes of PCNL, the GSS is easy to perform and more convenient to be used in daily practice.
The limitations of our study include the retrospective design, exclusion of patients who were evaluated with CT postoperatively, and acceptance of the residual fragments <4 mm as stone free.
Conclusion
In the current study, we found that both GSS and CROES nomograms had comparable accuracies in predicting post-PCNL stone-free status. Different from the previous reports, our results showed that both nomograms were predictive of overall complications, EBL, and operative time.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.