
Abstract
Introduction:
Recent evidence would suggest a low rate of metabolic assessment in stone formers, even in those deemed as high risk. We wished to assess the attitudes and practice patterns of metabolic work up in North American members of the Endourological Society as part of the management of stone-forming patients.
Methods:
A 12-question online multiple-choice questionnaire (using Survey Monkey®) was distributed to all members of the Endourological Society through e-mail. Descriptive analyses were performed.
Results:
A total of 124 North American members of the Endourological Society responded (90% endourologists, 65% fellowship trained). Ninety-seven percent perform metabolic assessments without referring to a consultant. Eighty-three percent use a commercial analysis company and 17% request serum or urine parameters individually. Ninety-seven percent believe that 24–48-hour urine collection is a better way of assessing patients for metabolic abnormalities than a “basic analysis.” Many respondents (37%) would be more likely to metabolically assess if results were easier to interpret, and 35% would like assistance/advice in the interpretation of results. At initial investigation of a first-time stone former, 87% of respondents use serum chemistry, 48% use 24-hour urine, 26% use 48-hour urine (two consecutive 24-hour urine collections), 54% send stone for analysis, and 7% do not investigate. On recurrent stone formers, 69% use serum chemistry, 73% use 24/48-hour urine, and 23% send stone for analysis. On routine follow-up, 36% check serum chemistry, 55% use 24-hour urine, 2% use 48-hour urine, and 29% do not metabolically evaluate. The majority agree that pharmacologic therapy plays a strong role in preventing recurrence (90%). After initiating pharmacologic therapy, 59% reassess using serum chemistry and 84% and 7% use 24/48-hour urine collection, respectively. Physicians re-evaluate patients after 1 month (7%), 1–2 months (10%), 2–4 months (44%), 4–6 months (30%), or after 6–12 months (7%).
Conclusion:
This snapshot assessment of Endourological Society members' practices in the metabolic investigation of stone-forming patients demonstrates wide testing variations. Many physicians expressed interest in assistance/advice in the interpretation of the metabolic assessment results.
Introduction
O
Thankfully, most visits to the physician for kidney stones occur in the outpatient setting and represent an excellent opportunity for screening, treatment, and surveillance. Between 1992 and 2000, physician office visits in the United States for kidney stones increased by 43%. 6 When asked, most patients would consider preventative pharmacotherapy as preferable to stone episodes or surgical intervention. 7 Despite this, metabolic evaluation is not commonly performed even in high-risk stone patients. 8 This may be indicative of universally poor investigation of nephrolithiasis and may reflect physician confusion, reduced awareness, or lack of confidence in the interpretation of metabolic parameters. Recently, the American Urological Association (AUA) published updated guidelines in the medical management of kidney stones. 9 These were evidence-based suggestions with regard to the metabolic investigation of stones disease; dietary and pharmacologic advice was also given. In light of these new guidelines and based on recent evidence showing poor use of metabolic investigation, we wished to assess physician's attitudes and awareness toward the metabolic investigation of stone-forming patients.
Materials and Methods
A cross-sectional study was carried out to evaluate the attitudes and practice patterns in metabolic stone evaluation of stone-forming patients. A 12-question online multiple-choice questionnaire (using Survey Monkey®) was distributed to all members of the Endourological Society through e-mail (Supplementary Appendix 1; Supplementary Data are available online at
Due to the anonymous nature of the survey, participants' demographics such as age, gender, and regional variation were not assessed. However, the setting of their practice and some of their professional background were available. In addition, we assessed the urologists' awareness of the recent AUA guidelines. Analysis was carried out using Microsoft® Excel software.
Results
The survey was distributed to 2686 unique e-mail addresses in the Endourological Society's database; a total of 247 members (9.2%) responded. One hundred twenty-four of these members reported practicing in North America with the remainder being international. Due to variations in health systems and international clinical practice patterns, the reported results apply to the North American urologists only.
Of respondents, 90% considered themselves endourologists and 65% of these were fellowship trained. Further details regarding practice type, location, and practices can be found in Tables 1 and 2. The majority (96%) of respondents were aware of the new AUA guidelines. When performing metabolic evaluation, most urologists (97%) perform the assessment themselves rather than referring the patient to another clinician. Only 17% of respondents request serum or urine parameters individually, whereas the majority (82%) avails of a urine analysis company. The majority of respondents feel confident in their ability to interpret 24/48-hour urine results (97%). Despite this, physicians say that they would be more likely to order a full metabolic analysis (serum and urine) if it were easier to interpret and/or make clinical decisions (37%). In addition, many (35%) would be interested in assistance or advice in the interpretation of the metabolic evaluation.
SWL, shockwave lithotripsy; PCNL, percutaneous nephrolithotomy.
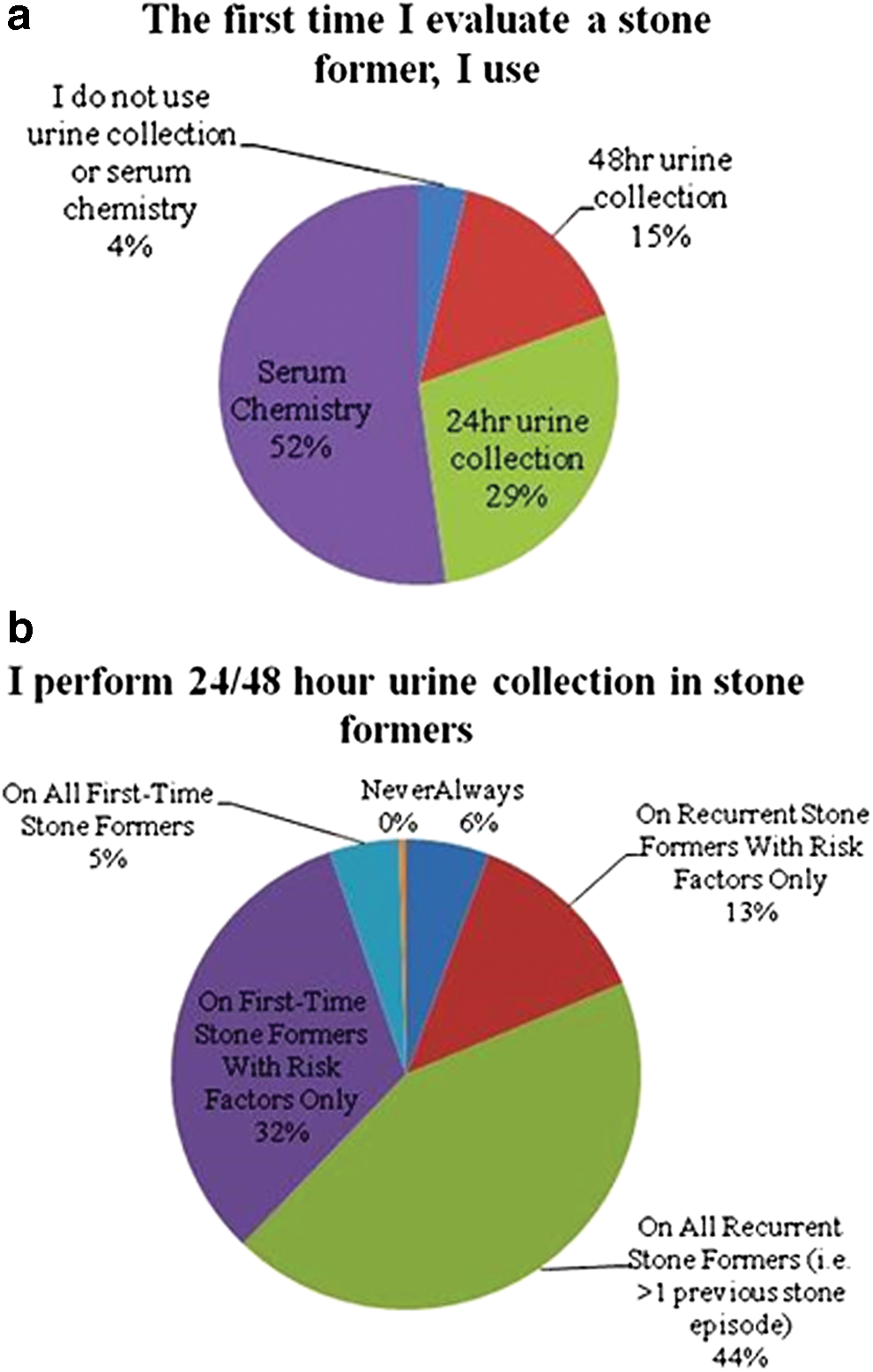
At initial investigation of a first-time stone former, 52% of physicians use serum chemistry, 29% use 24-hour urine collection, 15% use 48-hour urine collection, 54% send a stone for analysis if available, and 4% say they do not investigate (Fig. 1a). Respondents were asked when they perform 24/48-hour urine collection exactly; 44% said on all recurrent stone formers, 32% on first-time stone formers with risk factors only, 13% on recurrent stone formers with risk factors only, 5% on all first-time stone formers, 6% always, 0% never (Fig. 1b). Respondents were asked when they order parathyroid hormone and calcium levels in stone formers and results are depicted in Figure 2. On recurrent stone formers (i.e., >1 previous stone episode), 69% use serum chemistry, 73% perform a 24/48-hour urine, and 23% send a stone for analysis if available.
Respondents' preferences in
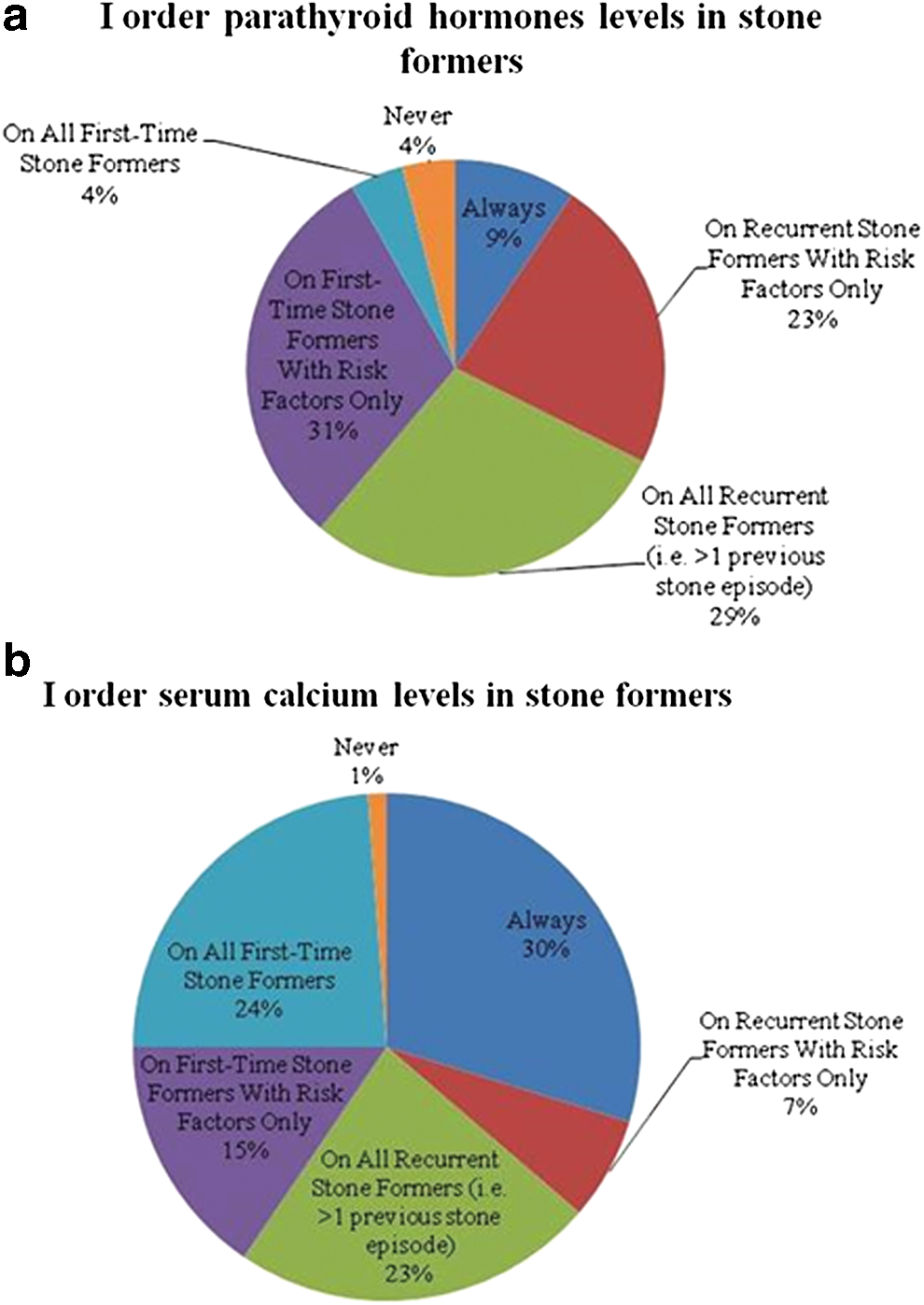
Practice patterns in ordering of
On a routine outpatient follow-up, 30% check serum chemistry, 45% 24-hour urine collection, 1% 48-hour urine collection, and 24% do not metabolically evaluate (Fig. 3). The majority of respondents agree that stone analysis is helpful (97%) and that they can get stone analysis easily (98%). Only 15% believe that stone analysis is too costly.

Preferences by respondents in reassessing stone formers on routine follow-up. Color images available online at
The majority of respondents agree that pharmacologic therapy plays a strong role in preventing recurrences (90%). The majority agree that they are confident in their knowledge of the side effects of pharmacotherapy (95%) and believe that 24–48-hour urine collection is a better way of assessing patients for metabolic abnormalities than basic metabolic analysis serum with or without stone analysis (97%). After initiating pharmacologic therapy, 38% say they reassess using serum chemistry, 54% use 24-hour urine collection, and 5% use 48-hour urine collection (Fig. 4a). After initiating pharmacologic therapy, respondents re-evaluate patients after 1 month (7%), 1–2 months (10%), 2–4 months (44%), 4–6 months (30%), or after 6–12 months (7%). Two percent of respondents did not re-evaluate their patients after initiating pharmacologic therapy (Fig. 4b). The majority of physicians feel that their patients are compliant with their medications (54%).
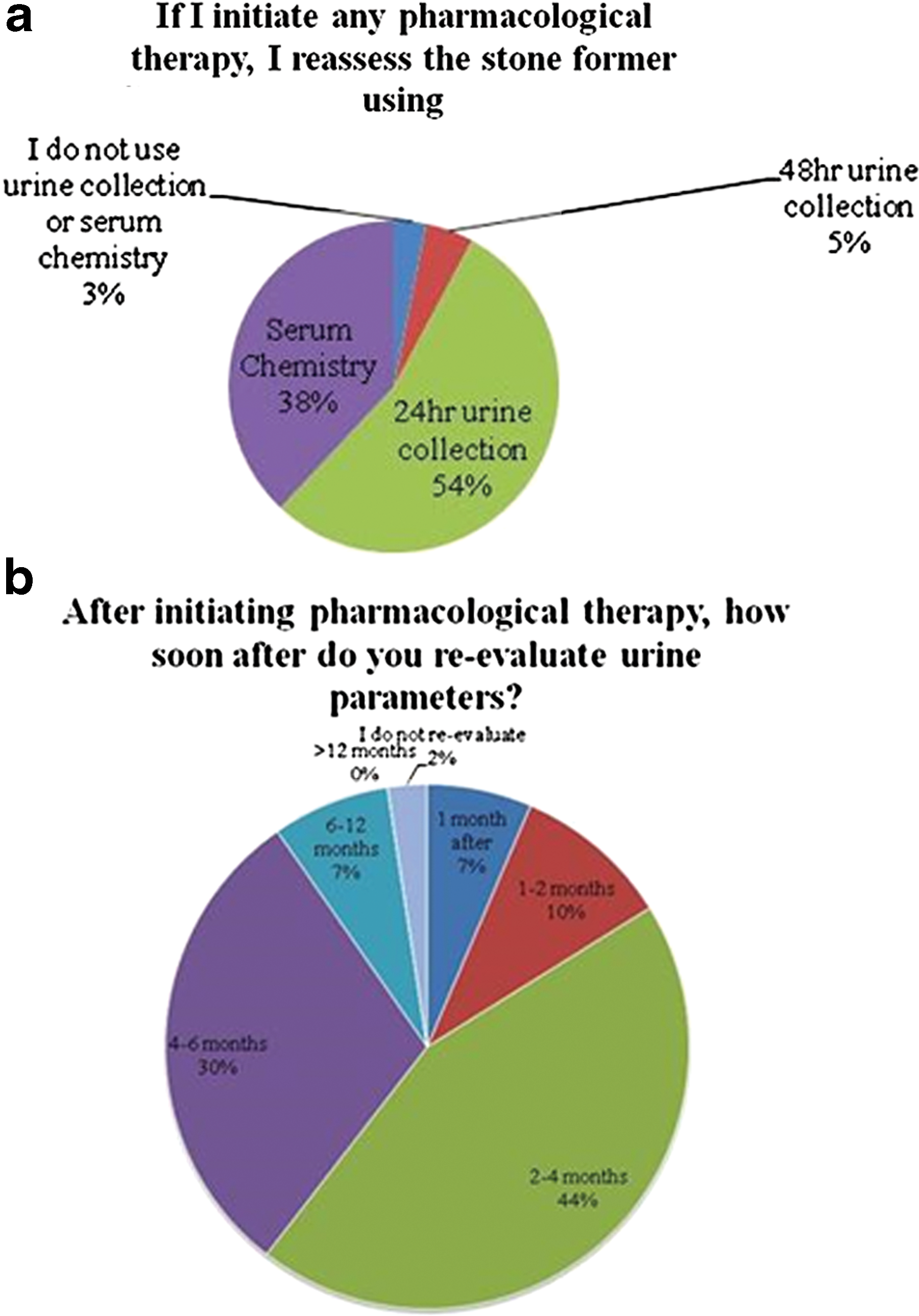
Preferences in use of
In terms of dietary recommendations, only 40% of physicians feel their patients are compliant with dietary/fluid advice. The majority feel they have the time to counsel patients on dietary changes to prevent stones (66%) and are confident in their ability to counsel patients in dietary changes (89%). Only 53% claim their patients have access to a dietary counselor.
Discussion
This study is an assessment of the current attitudes and practice patterns of the Endourological Society members in the investigation of stone-forming patients. The results demonstrate that most respondents are metabolically investigating stone-forming patients themselves without outside referral. Although there is a strong bias in favor of stone enthusiasts responding to the study, our research demonstrates a wide variability in how metabolic assessment is performed even within this select cohort.
Whether or not to investigate a stone-forming patient is not without controversy. Previously, as a result of lack of clear clinical care pathways and algorithms, a wide variety of testing variability and practice patterns developed. Whether it is a first-time or recurrent stone former, or routine follow-up, our data demonstrate wide variation in the assessment and reassessment of stone-forming patients. Our respondents have varying preference for serum analysis or urine analysis, with some (although less commonly) choosing neither investigation. Controversy exists on whether to do a full or partial metabolic investigation. 10 Proponents of a full evaluation argue that the majority (90%) of stone formers submitting a 24-hour collection will have a metabolic abnormality in which directed therapy can be initiated; that the condition has a high recurrence rate and a high medical and socioeconomic burden; and that complete evaluation when performed is informative, actionable, and cost-effective. Proponents of a partial evaluation argue that evidence is limited for whether a full metabolic assessment vs baseline biochemistry evaluation is associated with better outcomes 11,12 and that data are limited on whether dietary or fluid intake alone performs better than pharmacologic therapy. 11,12 Certainly, we are in real need for large-scale randomized controlled trials to prove if pharmacologic therapy is superior to dietary or fluid advice in the long-term management of stone-forming patients.
Unfortunately, each stone-forming patient is quite unique with a host of confounding variables that make large-scale study of different therapies hard to assess, for example, diet, climate, genetics, body weight, exercise, and occupation. Interesting to note in our data, despite a response by physicians saying they feel confident in their ability to interpret results (similar to prior studies), 13 the third respondents say they would be more likely to order metabolic investigation if they had assistance in interpreting the results. It is likely that respondents to this survey are interested in stone prevention and treatment, yet surprisingly within this group, a large proportion expresses interest in helping with interpreting the data. There is no doubt that the interpretation of metabolic results can often be complex with a host of variable factors that need to be connected to make the right diagnosis and initiate treatment. Data from Milose et al. 8 suggest that as low as 7% of high-risk stone-forming patients are investigated metabolically, 8 and this may reflect physician confusion/lack of confidence. Interestingly, the majority of respondents use a urine analysis company that usually has clear graphic data accompanied with interpretation. It would be interesting to know if the introduction of these companies has increased metabolic investigations by facilitating easier clinical decision-making.
The recent publication of AUA guidelines on the medical management of kidney stones (2014) has been an excellent first step in trying to consolidate the investigation of these patients. These guidelines recommend that “clinicians should perform a screening evaluation consisting of a detailed medical and dietary history, serum chemistries and urinalysis on a patient newly diagnosed with kidney or ureteral stones.” Our data suggest that this is being followed by the majority. However, there are many variances in which modality a physician would choose. The majority choose serum analysis with only half choosing urine analysis. It is interesting to note that there is a higher rate of urine analysis in recurrent stone formers, which indicates a preference for urine assessment in those with recurrent stones. The AUA recommends stone analysis at least once when a stone is available. We see that the overwhelming majority agree that stone analysis is helpful in our study, yet only half send a stone for analysis on first-time stone formers, and a quarter on recurrent stone formers.
There are no clear guidelines for clinicians on how to follow-up patients with regard to a routine clinic visit, mainly because long-term studies are lacking. In reality, clinicians will evaluate each patient individually and decide on their risk for future stone formation. Other issues that affect the decision on how to follow up include the type of stone formed, significant medical history, for example, short gut syndrome, patient anxiety, and stone status on recent imaging. There are no prospective longitudinal data in which clinicians can confidently predict when stones will form, as each patient differs greatly from the next. Our data show that clinicians are following patients closely after initiating therapy, however, there are still wide practice variations between them.
Our data have some limitations. With a low response rate to the questionnaire, it is hard to generalize on how stone-forming patients are being investigated by the urology community at large. In the era of subspecialization, it is likely that urologists with a specialist interest in stone treatments responded to the study introducing a bias into these results. In addition with stones being such a common clinical scenario, it is likely that these patients are being treated by a high proportion of urologists, not all of whom would be specifically trained in metabolic assessment and treatment of nephrolithiasis. These two factors would overestimate the impression that urologists are thoroughly metabolically investigating stone-forming patients.
Conclusion
In a contemporary assessment of the Endourological Society members' attitudes and practices in the metabolic investigation of stone-forming patients, we demonstrate a wide variation in the metabolic assessment of these patients. The majority of respondents are aware of recent AUA guidelines, agree that pharmacologic therapy plays a strong role in preventing recurrences, and over a third of physicians would be interested in assistance or advice in the interpretation of the metabolic assessment results.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviation Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.