
Abstract
Objectives:
Laparoendoscopic single-site surgery (LESS) and natural orifice transluminal endoscopic surgery (NOTES) produce excellent cosmetic outcomes, but are technically challenging. The objective of this study was to test the functionality and feasibility of a novel minimally invasive surgical paradigm, which maintains triangulation but uses special externally assembled instruments to minimize the postoperative cosmetic impact.
Methods:
Percutaneous Externally Assembled Laparoscopic (PEAL) instruments have specialized 2.96-mm shafts with interchangeable 5-mm working tips that are assembled externally. First, 5-mm laparoscopic, PEAL, and 2-mm needlescopic instruments were tested to determine piercing force on fresh human cadaver organs. In a bench-top study, 20 subjects assembled and used PEAL instruments in five different skills tests that were also compared with the same tasks using conventional laparoscopic instruments. Finally, PEAL instrument functionality was tested in a four-porcine nephrectomy feasibility study.
Results:
PEAL (2.80 lbF) and 5-mm laparoscopic instruments (2.28 lbF) had a significantly higher mean organ piercing perforation force compared with needlescopic instruments (1.39 lbF, p < 0.05). Average assembly time of PEAL instruments was 31.08 seconds (range: 19.83–43.85). There were no significant differences in the amount of time needed for completion of the bench-top tasks between laparoscopic and PEAL instruments (p > 0.05 for all tasks). Four-porcine PEAL nephrectomies were completed with no complications and minimal blood loss (mean 7.5 mL). Mean operative time was 98.25 minutes (range 79–116).
Conclusion:
PEAL tools are easily assembled, have similar safety and efficacy compared with standard laparoscopic tools, and are less likely to injure organs compared with needlescopic instruments. They function well during laparoscopic nephrectomy and may decrease the invasiveness of conventional laparoscopic instrumentation.
Introduction
S
Needlescopic instrumentation has been combined with hybrid forms of LESS and NOTES to re-establish triangulation and simplify these procedures. 15,16 The postoperative cosmetic impact of these instruments has been minimal, however, the available 2–3-mm instrumentation is limited and has reduced functionality. 16 –18
In an attempt to maintain the triangulation and nearly scarless cosmetic outcome associated with needlescopic instruments, while also allowing for a more functional 5-mm instrument tip, we designed, developed, and created a novel surgical paradigm called Percutaneous Externally Assembled Laparoscopic (PEAL) surgery. The purpose of this study was to test the bench-top functionality of PEAL instruments and then confirm the feasibility of PEAL nephrectomy in a porcine model.
Materials and Methods
Concept of PEAL surgery
In previously published studies, it was shown that needlescopic 2-mm ports facilitated both LESS and NOTES nephrectomy with minimal cosmetic impact. 15,16 However, the limited availability and decreased functionality of needlescopic instruments, led us to consider whether it would be possible to maintain a small shaft size (≤3 mm) but incorporate a larger (5–10 mm) more functional instrument tip.
To accomplish this goal, a ≤3-mm shaft could be percutaneously inserted, without a port, allowing the largest caliber and most rigid shaft possible for the incision size. The shaft tip could be brought out through a larger umbilical port, which would be hidden in the crease of the umbilicus. By externalizing the distal instrument shaft, a 5-mm instrument tip could be screwed into position and brought back into the abdomen for use in PEAL surgery (Fig. 1a).
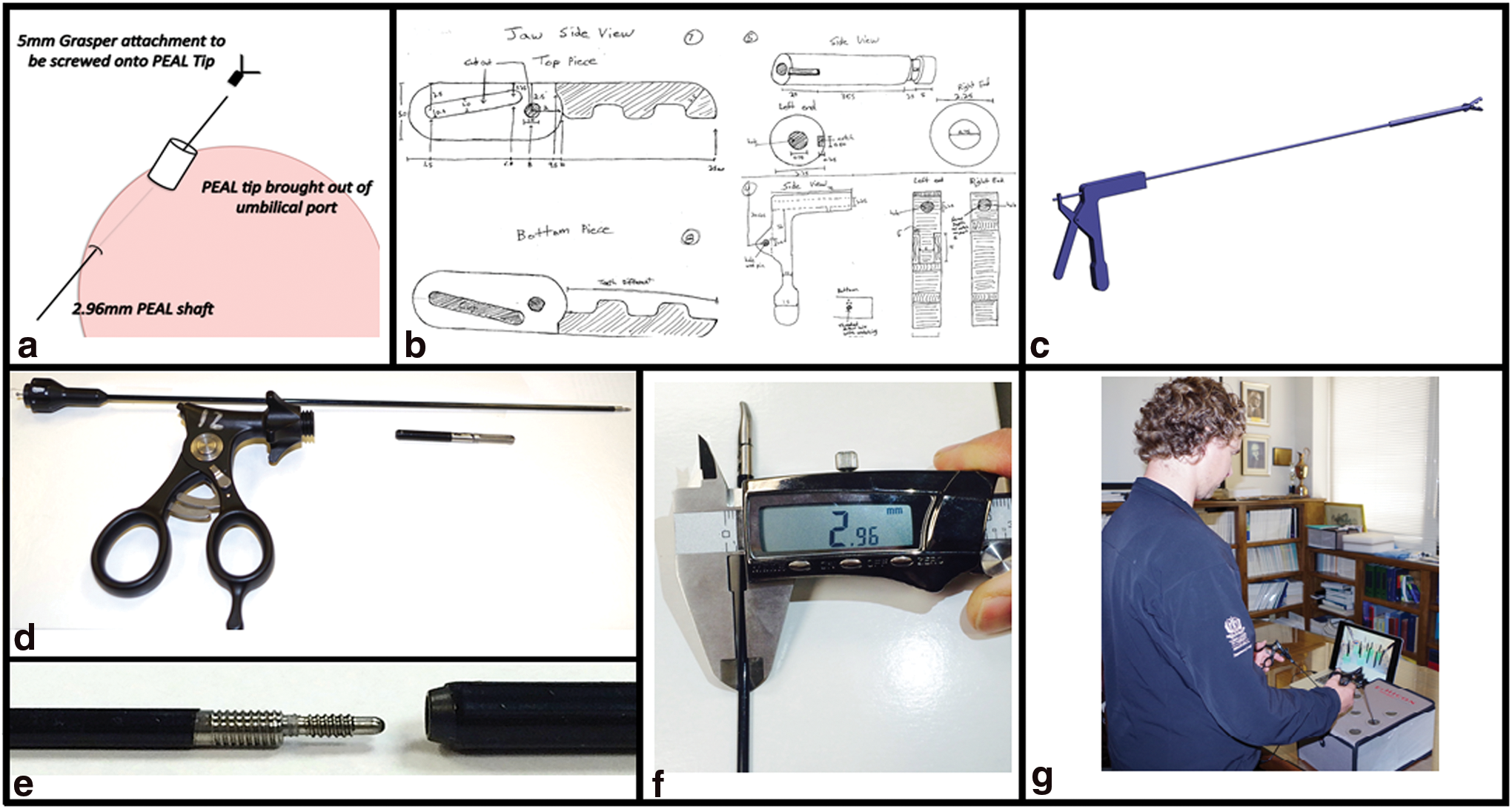
After the development of three different generations of instruments (Fig. 1b, c), Teleflex Surgical (Teleflex, Wayne, PA) manufactured an easily assembled device, and this generation of instrument was utilized for this cadaver, bench-top, and animal study. These instruments consist of three parts; a reusable handle, a disposable 2.96-mm instrument shaft, and a 5-mm disposable instrument tip that screws on to the instrument shaft (Fig. 1d–f).
Bench-top trial of PEAL tools
Due to their small size, needlescopic instruments may increase the risk for inadvertent puncture or injury of internal abdominal organs. In the first phase of this study, the forces required to pierce the capsule of fresh human cadaver liver, kidney, and spleen were tested for the PEAL fenestrated grasper and Maryland and were compared with similar 5-mm conventional laparoscopic (Silex Medical, Southington, CT) and 2-mm needlescopic instruments (Richard Wolf Medical, Vernon Hills, IL). The instruments were attached to a Mark 10 digital force gauge (maximum measurable force = 3.3 lbF) (Mark-10 Corporation, Copiague, NY), and the tip was then advanced perpendicularly into these fresh human cadaver organs until capsular perforation occurred. Each instrument tip was tested 10 times, and the means were calculated and compared using pairwise comparisons with p < 0.05 considered significant.
The second phase of this study was to assess the ease of assembly and functionality of the PEAL instruments in a bench-top model. After a short didactic session, study participants were randomly assigned one PEAL device to assemble. Participants varied by the level of laparoscopic experience and included individuals with no prior laparoscopic experience (n = 5), individuals whose only laparoscopic experience was prior use of a laparoscopic trainer (n = 5), individuals who had some operative laparoscopic experience but do not incorporate laparoscopic surgery in their current practice (n = 5), and staff surgeons who are regularly performing laparoscopic surgery in their current practice (n = 5). The time required for assembly was recorded and the ease of assembly was graded using a Likert scale (1 = easy to 10 = very difficult).
Participants were then asked to use a previously tested laparoscopic skills trainer (Ethicon TASKit 19 ; Ethicon U.S.A, Somerville, NJ; Fig. 1g) to randomly complete basic laparoscopic skill projects with both PEAL and conventional 5-mm laparoscopic tools (Stryker, Kalamazoo, MI). The skills tested included two tasks for eye/hand coordination (placing beads onto a post, transferring silicone bead wedges onto a peg board), one task for traction/countertraction (unwrapping a candy), one task testing dexterity and tissue manipulation with traction/countertraction (peeling a liquorish stick into its nine individual fibers), and one task for dissection along a plane (removing the skin from a grape). The time needed to complete these tasks, with both instrument types, was documented for each cohort and compared between the different experience levels using a Wilcoxon signed rank test with p < 0.05 considered significant.
Use of PEAL surgery for porcine nephrectomy
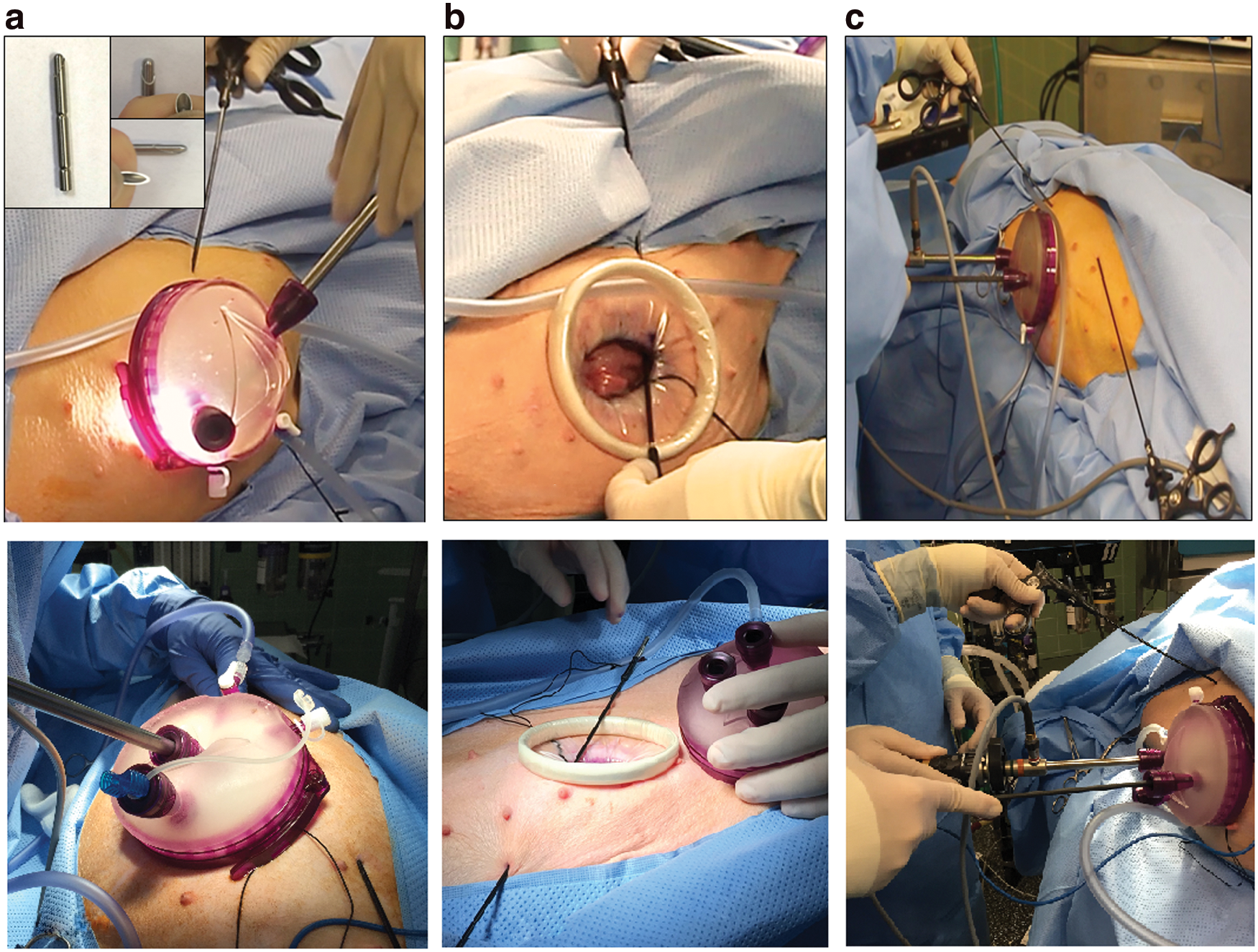
In the third phase of the study, the safety and in vivo functionality of the novel instruments were tested when PEAL left nephrectomies were performed in four female farm pigs (mean weight 32.5 kg, range 31–33) by a surgical team consisting of one fellowship-trained staff endourologist and one endourology fellow. Each pig was induced with a combination of ketamine (2.2 mg/kg), telazol (4.4 mg/kg), and xylazine (2.2 mg/kg). The pigs were intubated, anesthesia was maintained using isoflurane (2.5%–3.5%), and the abdomen was sterilely prepped and draped in the supine position. A 4 cm incision was made at the umbilicus and a gel point (Applied Medical, Rancho Santa Margarita, CA) was inserted. Carbon dioxide gas was used to insufflate the peritoneum to 15 mm Hg. Two 12-mm ports were placed through the gel point and a 10-mm 30° laparoscope was introduced. Two PEAL instrument shafts were percutaneously inserted through the abdomen 2 cm lateral to the nipple line using the detachable PEAL insertion retractable needle tip (Fig. 2a). After bringing the shafts out through the umbilical incision, two fenestrated grasping tips were attached to the PEAL shafts and brought back into the abdomen (Fig. 2b).
The dissection was performed using a 5-mm hook electrode brought in through the single-site port. One PEAL grasper was utilized to retract the bowel and pancreas medially. The second PEAL grasper was used to maintain lateral traction on the kidney and ureter, facilitating the hilar dissection. The ureter and vessels were clipped using a 5-mm clip applier (Hem-o-lok; Teleflex) also placed through the single-site port. After the kidney was completely mobilized, it was grasped with the PEAL grasper and pushed out through the umbilical incision.
On removal of the specimen, the renal fossa was inspected to confirm hemostasis. The PEAL instrument tips were brought out through the single-site port and the working device tips were removed. The shafts were retracted out of the body and the skin edges approximated with tissue glue. No suture was used to close the PEAL sites. Finally, the single-site umbilical port was closed in two layers. After 4 weeks, the animals were euthanized, skin incisions were assessed, and intra-abdominal evaluation was performed.
Operative times, mean blood loss, time required for port placement, and PEAL tool assembly were all reported. A Likert scale was completed by the surgeon, grading difficulty of instrument placement, tool assembly, hilar dissection, nephrectomy performance, and closure.
Results
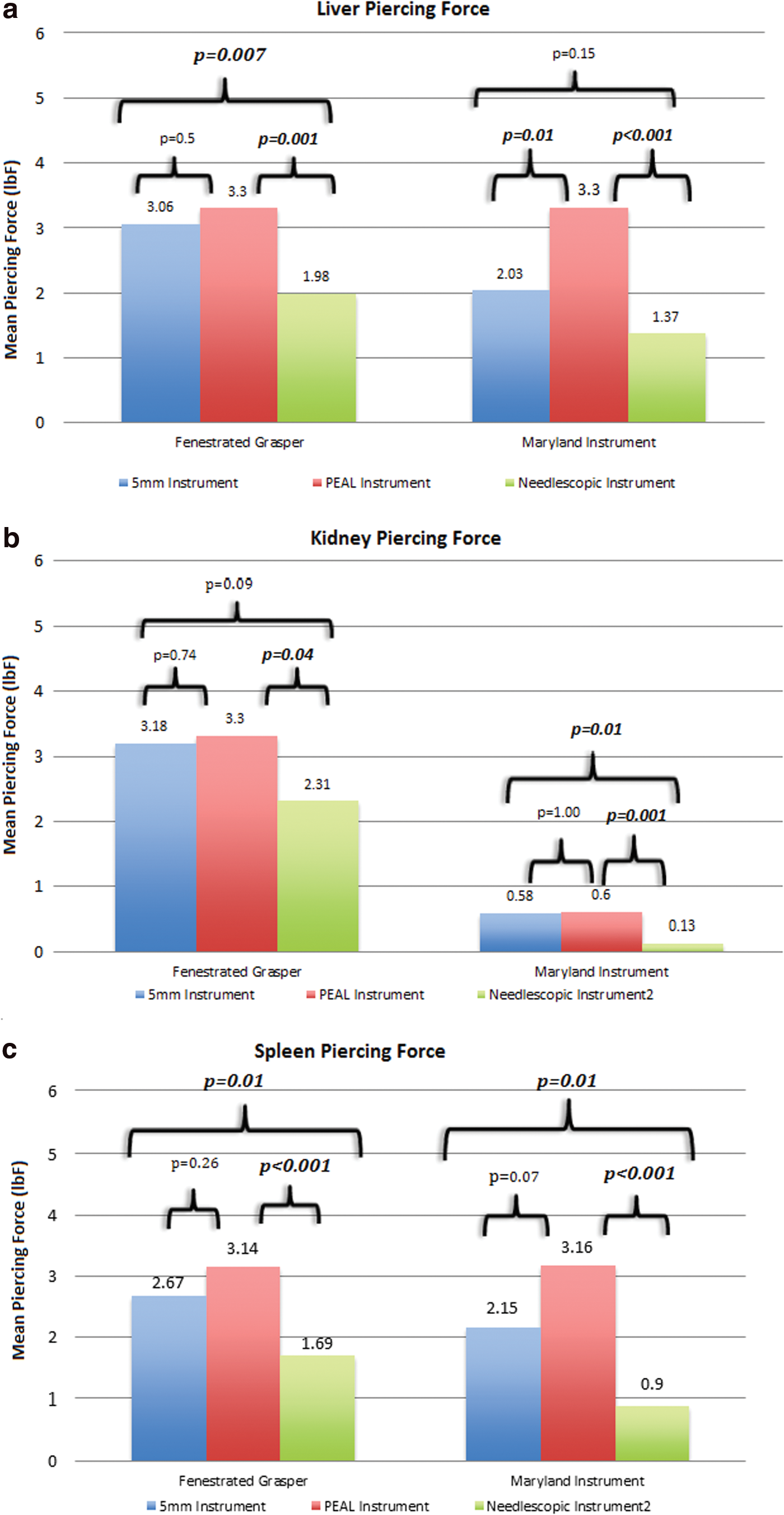
In the safety analysis comparing piercing forces of different instrument sizes in different fresh human cadaver organs, the average force required to pierce through the liver capsule was 2.55 lbF for the 5-mm tools, >3.3 lbF for the PEAL, and 1.68 lbF for the needlescopic tools (Fig. 3a). The average force required to pierce through the kidney capsule was 1.88 lbF for the 5-mm tools, 1.95 lbF for the PEAL instruments, and 1.22 lbF for the needlescopic tools (Fig. 3b). The average force required to pierce through the spleen capsule was 2.41 lbF for the 5-mm tools, 3.15 lbF for the PEAL instruments, and 1.30 lbF for the needlescopic tools (Fig. 3c). The 2-mm needlescopic tools required significantly less piercing force than the PEAL tools (p < 0.05 for each instrument, in each organ).
Piercing forces of different instruments in fresh human organs:
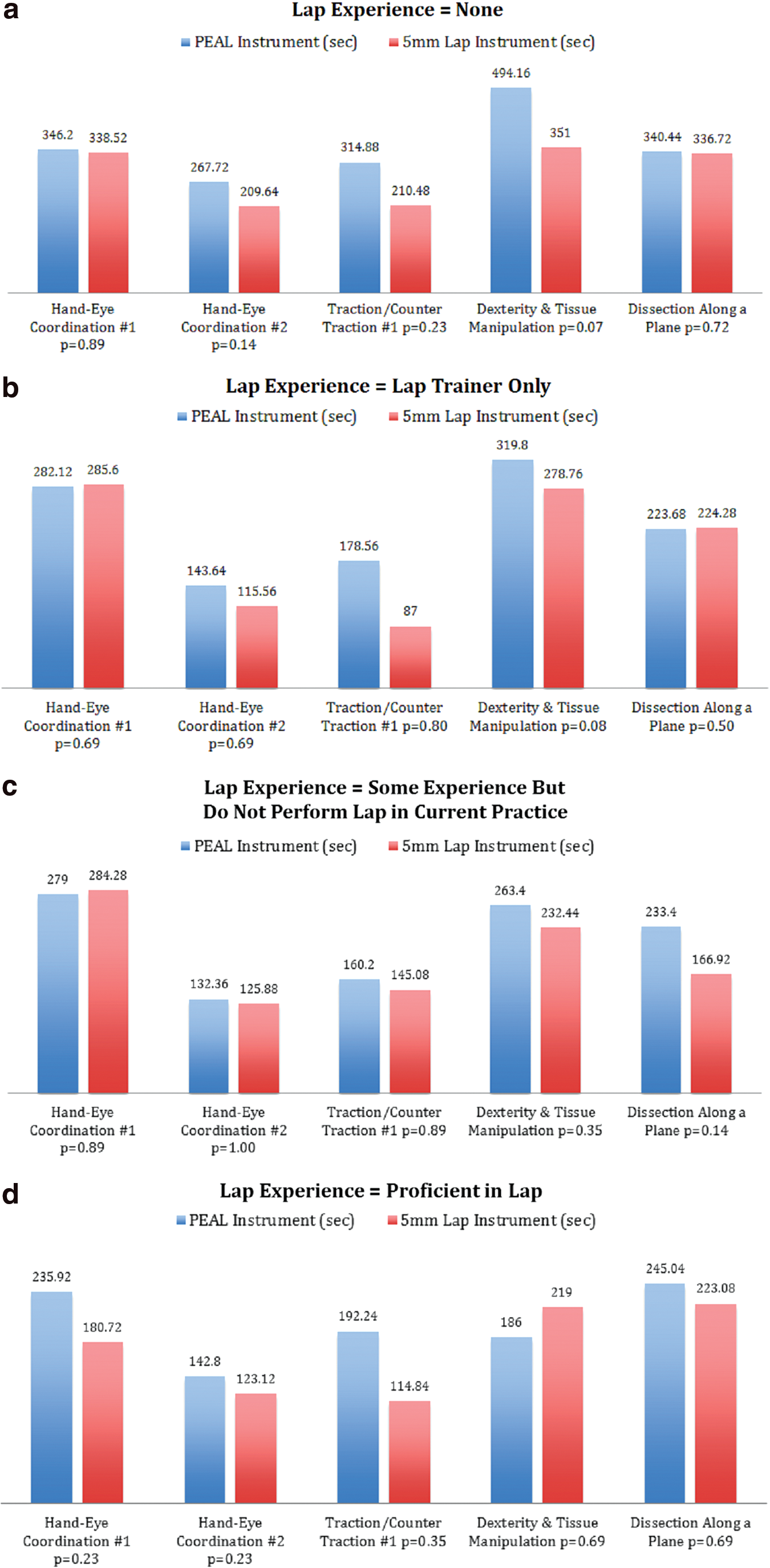
In the bench-top study comparing the assembly time and functionality of PEAL and laparoscopic instruments, the average time for assembly of a PEAL instrument was 31.08 seconds (range: 19.83–43.85). Using a Likert scale, the ease of assembly was rated as 3.25 (range: 1–6). Within each laparoscopic trainer cohort, there was no significant difference between the PEAL and conventional laparoscopic tools in the time required to complete any of the five tasks (Fig. 4a–d). However, the combined time of the experienced surgeons to complete each task was faster than those with no laparoscopic experience, thus validating the ability of these tasks to differentiate surgical skill (p < 0.05 for each task).
PEAL nephrectomy
PEAL nephrectomy was completed effectively in each of four porcine procedures. Total mean operative time was 98.25 minutes (range: 79–116), and mean blood loss was 7.5 mL (range: 5–10). Mean time required for gel point placement, percutaneous tool insertion, and assembly was 20.5 minutes (range: 18–23). The kidney was extracted intact through the single-incision site. Mean time from the start of the case until the nephrectomy was completed was 75.5 minutes (range: 60–91). There were no intraoperative or immediate postoperative complications. Furthermore, there were no malfunctions of any of the PEAL instruments. After 4 weeks, there were no infections, and the PEAL sites had excellent cosmetic results (Fig. 5). Table 1 lists the results of the four PEAL nephrectomies along with the Likert scale results measuring the ease of each of the surgical steps.

Four weeks postoperative PEAL scar, purple marking pen circumferentially surrounds area of scar, measured at 0.5 mm in diameter. Color image available online at
EBL = estimated blood loss; PEAL = percutaneous externally assembled laparoscopic.
Discussion
Laparoscopic surgery provides patients with the benefit of decreased convalescence, improved pain control, and cosmesis. 20,21 While laparoscopic surgery has advanced toward smaller and less invasive surgical approaches, the ability of the average surgeon to perform LESS and NOTES is hampered by the technical demands created by the loss of triangulation and limitations of currently available instrumentation.
Needlescopic surgery has been shown to provide excellent cosmesis; however, this technology has been reported to have technical limitations. Since the instruments are less robust, they provide weaker compression force and may make it more difficult to gain hemostasis and manipulate heavy organs. 17 Also, the small diameter of a 2-mm instrument lacks rigidity and tensile strength, and thus, they bend easily when lateral forces are applied. 17,18 In addition, the smaller instrument size makes these needlescopic instruments more likely to result in intra-abdominal injuries such as splenic, liver, or renal capsular injuries, as demonstrated in our current study where piercing forces were 50% less in the 2-mm instruments compared with the PEAL instruments.
In an attempt to simplify LESS surgery by restoring triangulation, it has been previously demonstrated that the addition of a 2-mm port adds little to the overall cosmetic impact and results in cosmesis similar to traditional LESS surgery. 16 Meanwhile, other investigators have also reported on near-scarless results with 3-mm instruments. 22,23
As we pursue a near-scarless postoperative outcome, we have conceived, designed, created, and demonstrated the feasibility of a novel laparoscopic paradigm called PEAL surgery. The addition of a 5-mm instrument tip after passing the 2.96-mm shaft through the skin provides a 5-mm instrument tip with similar functionality to conventional 5-mm laparoscopic instrumentation while maintaining a near-scarless postoperative result. Our bench-top data confirm that the maneuverability and intra-abdominal safety of the PEAL instruments are equivalent to that of standard 5-mm laparoscopic instruments.
A benefit of PEAL surgery is the possible restoration of triangulation that is lost with LESS and NOTES. Our prior porcine study comparing pure LESS to hybrid LESS, including needlescopic instrumentation, showed that restoration of triangulation to LESS simplified the procedure and reduced operative times by nearly 30%. 16 In the current study, we used a gel point umbilical port as a single-site access, and with this, PEAL surgery reduced the operative time by 37% compared with our prior LESS nephrectomies. This reduced operative time could reduce the total procedural cost. Restoration of triangulation could make hybrid-LESS easier in the obese patient and subsequently also improve intraoperative safety. Addition of PEAL instrumentation could allow for a broader application of the near-scarless goals of pure NOTES and LESS. PEAL instruments could also be used as a substitute in one or multiple ports for all types of conventional laparoscopic surgery and help reduce the overall postoperative scar formation. While our intraoperative assembly of the PEAL instruments was through a LESS port, assembly of instruments through a 12-mm port is also possible, although this was not specifically tested in this study.
While the ultimate cost of PEAL instrumentation is unknown, it is likely that the reusable handles may make this technology cost effective. Furthermore, the disposable tip and shaft will provide the lowest risk of transmission for infectious diseases and ease in processing of instruments. The reduced cost, improved safety compared with needlescopic instrumentation, and a nearly scarless cosmetic result make PEAL surgery a promising technology for minimally invasive surgery.
The early nature of these instrument prototypes is a limitation of this technique. At the time of this study, only three instrument tips were available, and subsequently, only two graspers were used in the porcine nephrectomies. The prototypes used in this study took a mean of 31 seconds to assemble in the bench-top portion of the study and although not specifically measured, the assembly time may have been even longer in the porcine nephrectomies. Another generation of instruments is being created to further simplify assembly. In addition the next generation of instruments will include a larger assortment of instrument tips, including a hook electrode, clip applier, and a variety of other instruments.
Another limitation of this study is the use of a bench-top pelvic trainer to test the functionality of the PEAL instruments in a variety of tasks. Although the pelvic trainer does not recreate all aspects of laparoscopic surgery, its use allowed us to test the basic functionality of the PEAL instruments in a completely reproducible manner that would not have been possible in an animal model.
An additional limitation to this study is the fact that this is a bench-top and feasibility study using a small cohort. Although there was no statistically significant difference between any of the measured tasks, two of the tasks (traction/countertraction and tissue manipulation with traction/countertraction) showed trends toward faster performance with the conventional instruments. It is possible that with a larger cohort, this difference could become significant. We attribute this to the early stages of the PEAL instrument and a subjective reduced grasping strength of the instrument tip when trying to grasp bulky firm objects. Currently, Teleflex Surgical the manufacturer of these instruments is creating another generation of these instruments that may overcome this reduced grasping strength.
Ultimately, these instruments could be used in several ways. One method would be to combine these instruments in a hybrid manner with LESS (as demonstrated in this study) or NOTES procedures to decrease the operative time, learning curve, and surgical complexity. Another potential application would be to decrease the invasiveness of conventional laparoscopic surgery. Initially, as the surgeon is becoming familiar with this technology, the surgeon could use one or two PEAL instruments in the place of conventional 5-mm laparoscopic instruments to decrease the invasiveness of conventional laparoscopic instrumentation. With improved surgical experience, the surgeon might replace conventional laparoscopic instruments with PEAL instruments for simple surgical procedures. Furthermore, these instruments would appear to be well-suited for pediatric applications. While the bench-top and porcine surgical cohort reported in this study is small, it demonstrates the effective application of PEAL surgery and the promise of this technology to make laparoscopic, LESS, and NOTES surgical forms easier to perform and less invasive. Ultimately, the safety and efficacy of PEAL surgery will need to be tested prospectively and in clinical applications.
Conclusion
We have described the creation and development of a novel surgical paradigm. The cadaver portion of this study demonstrates that PEAL instruments are potentially safer than needlescopic instruments since they are less likely to injure intra-abdominal organs. In addition, the bench-top study showed that the PEAL instruments performed similarly to conventional 5-mm laparoscopic tools for the five tasks tested. Finally, for the first time, our porcine model demonstrates the feasibility of PEAL instrumentation for minimally invasive nephrectomy. By incorporating larger 5-mm tips on 2.96-mm instrument shafts, PEAL surgery could provide a near-scarless result with a functional reliable instrument tip. Utilization of this technology could reduce the invasiveness of conventional laparoscopic surgery and allow the application of near-scarless approaches to a much wider patient population.
Footnotes
Acknowledgment
The authors acknowledge Teleflex Surgical for providing the Percuvance® Percutaneous Surgical System instruments used to test the PEAL surgical paradigm.
Author Disclosure Statement
Dr. D. Duane Baldwin serves as a consultant for Boston Scientific and as a lecturer for Cook Medical. At the time of the submission of this manuscript Dr. Baldwin had no intellectual property or financial relationship with Teleflex Surgical. However, at the time of page proof review Dr. Baldwin was performing a study supported by Teleflex. No other financial interests exist for any other author.