
Abstract
Introduction:
The gold standard treatment for upper tract urothelial carcinoma (UTUC) is radical nephroureterectomy (RNU). The role of endoscopic resection is limited to low-risk patients. In this study, we present our 30-year experience in the endoscopic management of UTUC.
Methods:
In this retrospective study, we identified 141 patients who underwent percutaneous UTUC resection. Demographic and clinical data were collected, including tumor characteristics, bacillus Calmette–Guérin (BCG) and mitomycin use, tumor recurrence, progression to RNU, and overall survival (OS), and compared in univariate and multivariate analyses.
Results:
Median follow-up was 66 months. Recurrence occurred in 37% of low-grade patients and 63% of high-grade (HG) patients, with a median time to recurrence of 71.4 vs 36.4 months, respectively. Grade was the only predictor of recurrence (HR 2.12, p = 0.018). The latest time to recurrence occurred after 116 months of surveillance. RNU was avoided by 87% of patients. Age, imperative indications for endoscopy, a history of bladder cancer, and tumor stage and grade were predictors of OS; however, in multivariate analysis, grade and stage lost significance. BCG and mitomycin did not protect against recurrence, progression to RNU, or death over resection alone.
Conclusion:
Percutaneous management of UTUC allows for renal preservation in the majority of patients with resectable disease. Patients with HG tumors are more likely to experience recurrence, but are not at an increased risk of death. Intraluminal BCG and mitomycin continue to have a limited adjuvant role to resection. Recurrence may occur many years following initial resection and therefore prolonged surveillance is advised.
Introduction
U
Despite the temptation to derive conservative treatment algorithms for UTUC akin to transurethral resection for noninvasive bladder cancer, these are in fact two distinct diseases. European guidelines allow the conservative management of UTUC for tumors that are low grade (LG), small (<1 cm), unifocal, and do not appear infiltrative on imaging. 1 Unfortunately, 60% of patients with UTUC present with invasive disease, compared to 15% to 20% of those with bladder cancer. 3 Radical nephroureterectomy (RNU) is the gold standard treatment for UTUC, given its aggressive nature and advanced presentation. 4 However, the associated surgical comorbidities compounded with diminution of renal function give surgeons a pause to consider nephron-sparing alternatives, especially in patients with lower-risk tumors.
In 2009, we presented our institutional experience with the percutaneous resection of UTUC. 5 We showed that tumor grade was the strongest driver in overall survival (OS), but were not able to demonstrate a significant benefit of adjuvant bacillus Calmette–Guérin (BCG) following endoscopic resection. Since then, we have added a significant number of patients and longitudinal follow-up allowing for this comprehensive 30-year experience with the percutaneous resection and endoscopic surveillance of UTUC. Our aim is to definitively identify risk factors for recurrence, progression to RNU and OS, and better define the role of endoscopy in the primary management of UTUC.
Materials and Methods
In this IRB-approved retrospective analysis, patients who underwent endoscopic and management of UTUC from 1985 through 2014 were included. A total of 244 patients were identified with an initial diagnosis of UTUC. The final cohort consisted of 141 patients who underwent percutaneous UTUC resection of renal or proximal ureteral tumors after excluding four with metastasis on presentation, one who was lost to follow-up, and 98 who underwent RNU for endoscopically unresectable disease or patient preference. The earlier cohort of patients was originally described in Rastinehad's 2009 study on the efficacy of BCG in UTUC. 5 Through an extensive archive review, 10 additional patients from that era were identified along with 42 new patients since 2006.
Tumors were classified as low or high grade (HG) according to the WHO grading criteria. 6 Earlier cohort patients designated as grade 1 or 2 using the WHO 1973 system were reclassified as LG, and grade 3 were reclassified as HG for the purposes of this study. Patients without muscularis involvement were staged as noninvasive, while those with muscle invasion were staged as having invasive disease.
Imperative indications for conservative management included solitary kidney, bilateral disease, creatinine clearance <30 mL/minute by Cockroft Gault, and those considered too frail to tolerate RNU. All others were categorized as elective candidates for endoscopic management.
The details of our percutaneous resection techniques have been previously described. 7,8 Following resection, a 12F nephrostomy tube was placed for antegrade instillation of BCG. Our protocol for BCG administration has also been previously described. 5 During periods of BCG shortage, mitomycin C (MMC, 40 mg in 40 mL of sterile water) was instead used in 20 patients and administered using a similar technique. Following an induction course, those without evidence of disease underwent surveillance urine cytology and cystoscopy every 3 months for 1 year, semiannually for the second year, and annually thereafter. Flexible ureteroscopy and renoscopy were performed 3 months following initial resection and if there was no evidence of disease recurrence, every 6 months for the first 3 years and then annually thereafter. Cross-sectional imaging was obtained following resection and annually if other studies remained negative.
Disease recurrence was defined as tumor in the ipsilateral kidney or ureter following complete initial resection. Tumors in the contralateral kidney or bladder were considered to be de novo disease to help differentiate the risk of localized vs bladder recurrence in the setting of endoscopic management. For patients no longer being followed by our clinic and without survival records documented in the hospital chart, the Social Security death index (SSDI) was used for OS. Given the ambiguity of death certificates and SSDI with regard to the cause of death, a cancer-specific survival analysis was omitted.
Continuous parameters were compared using the Student's t-test, and differences across categorical variables were determined using a chi-squared test. Kaplan–Meier analyses with univariate and multivariate Cox proportional hazards models were used for predictors of survival. All data were analyzed using STATA/IC 11.0 (Statacorp, College Point, TX).
Results
Review of our UTUC database revealed 141 patients, managed from 1985 to 2014, eligible for analysis. Patient demographics are presented in Table 1 and are stratified by grade. Sixty-eight patients had imperative indications for percutaneous tumor resection. Imperative indications included surgical risk (44%), solitary kidney (43%), bilateral disease (9%), and renal insufficiency (7%).
BMI = body mass index; RNU = radical nephroureterectomy.
The initial biopsy specimen at the time of resection was adequate for grading in 137 patients (97%) and staging in 119 patients (84%). Of the pathologically assessable specimens, 47% were HG. In addition, 79% of patients were confirmed to have noninvasive (cTa or cT1) disease. Multifocality was present in 17% of patients.
Patients with HG pathology on initial diagnosis were more likely to have imperative indications for percutaneous tumor resection (HG 63% vs LG 37%, p = 0.003). There was also a correlation seen with HG disease and a more advanced stage (p < 0.001). We found no change in the proportion of HG patients undergoing percutaneous tumor resection in the early vs later study periods (p = 0.71). The remaining demographic variables were similar across grades.
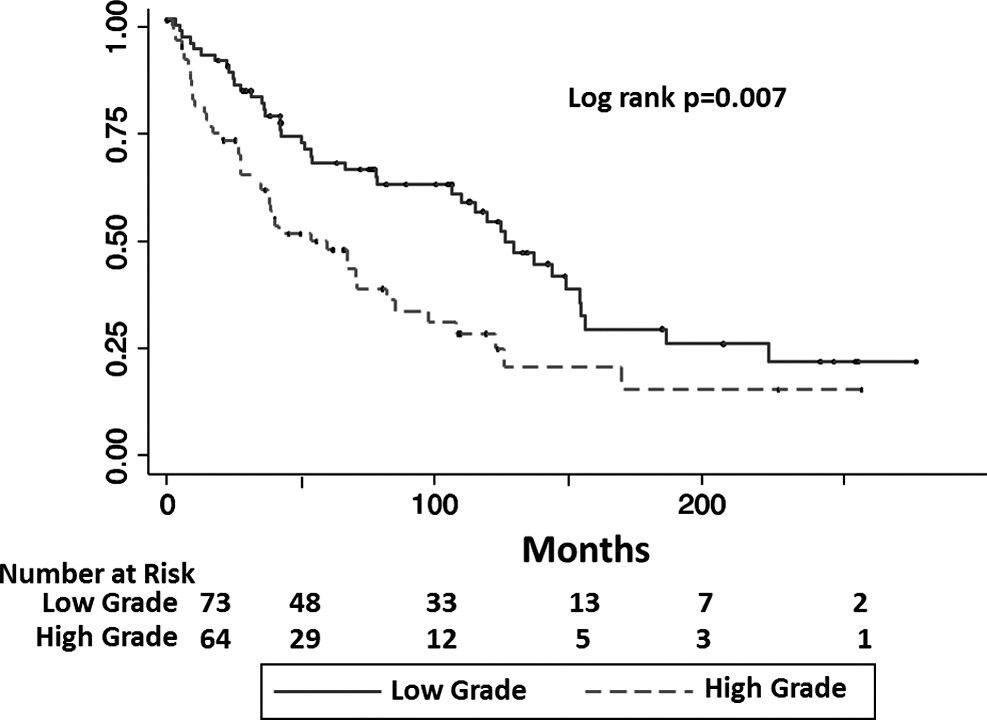
Median follow-up for this series was 66 months (mean 76.9 month, 3–280). Recurrence was endoscopically confirmed in 50 (35%) patients. When stratified by the initial biopsy grade, recurrence occurred in 27% of patients with LG disease compared to 44% of those with HG (p = 0.045). The median recurrence-free survival (RFS) was 71.4 months for LG vs 36.4 months for HG disease (Fig. 1). A Cox proportional hazards model (Table 2) revealed the advanced grade to be a significant predictor of RFS (HR 2.12, p = 0.018). Outside of tumor grade, there were no other predictors of RFS, including BCG (p = 0.85) and MMC (0.52). The latest UTUC recurrence occurred at 116 months, nearly 10 years following the initial diagnosis of UTUC.

Kaplan–Meier curve of recurrence-free survival stratified by tumor grade.
BCG = bacillus Calmette–Guérin; MMC = mitomycin C.
Overall, 122 patients (87%) preserved their affected kidney during the course of follow-up and 19 patients progressed to RNU. Of the patients without imperative indications for endoscopic management, 57 (83%) avoided nephroureterectomy. Similarly, 61 (90%) patients with imperative indications avoided RNU.
The median age at presentation was 73 years (mean 71 years). Over the course of this 30-year study, 85 (60%) patients had died. Age (HR 1.05), an imperative indication for endoscopic management (HR 1.83), grade (HR 1.81), and invasive (>T2) stage (HR 2.25) were predictors of OS (Table 3). The median survival was 126 months for LG vs 59.6 months for HG disease (Fig. 2). Although a potential confounder, there was not a statistically significant difference in patient age at diagnosis stratified by grade (LG 70.1 years old, HG 73.1 years old, p = 0.10, Table 1). Patients with a prior history of bladder cancer had a lower 5-year (50% vs 61%) and 10-year (19% vs 44%) survival. However, the development of de novo bladder cancer following UTUC diagnosis was not a predictor of earlier death. In multivariate analysis, age (HR 1.06, p < 0.001), an imperative indication (HR 1.75, p = 0.02), and a preexisting history of bladder cancer (HR 1.78, p = 0.035) were predictors of OS, but grade and invasive stage were not.
Kaplan–Meier curve of overall survival stratified by tumor grade.
Discussion
The management of UTUC remains complex and challenging. UTUC is far more likely than bladder cancer to be invasive at presentation and accordingly RNU is the gold standard treatment of UTUC. 1 However, patients with UTUC often present in their 70's or 80's with moderate comorbidities and an increased surgical risk. In addition, RNU has been shown to increase the risk of chronic kidney disease (CKD), which itself is associated with death. 9 –11 The nephron-sparing endoscopic option for low-risk disease is enticing, but the lack of randomized trials has limited a quality stratified treatment protocol guiding physicians as to when nephron-sparing endoscopic management vs RNU is appropriate. European guidelines for UTUC treatment limit endoscopic management to patients with LG, small unifocal tumors. 1
In this study, we provided our comprehensive 30-year experience with the percutaneous tumor resection of UTUC within the kidney and proximal ureter. Our cohort includes 141 patients, many with multifocal HG tumors and without imperative comorbidities precluding RNU. These extended criteria along with a median follow-up of over 5 years have allowed us to identify risk factors for recurrence, progression, and survival, with the hopes of expanding the limits of endoscopic management.
Studies have suggested that multifocality is a risk for poor overall prognosis. 12,13 However, these findings were either extrapolated from RNU series or did not achieve significance in patients undergoing endoscopic management. 12,14,15 The 24 patients (17%) in our series with multifocal disease were not at an increased risk of recurrence, progression, or death. It is conceivable that patients with multifocal tumors are harder to achieve a complete resection, especially when approached retrograde or by an inexperienced endoscopist. Residual disease subsequently progresses or is misinterpreted on follow-up as a recurrence, rather than multifocality, itself a marker of more aggressive disease. An inherent bias of our series may be that patients with multifocal disease and a significant tumor volume were deemed endoscopically unresectable, counseled toward RNU, and excluded from this study. Ultimately, multifocality for which a complete resection is achievable should not be a contraindication to percutaneous tumor resection.
Over half (52%) of the patients treated elected conservative management without an imperative indication, but rather a personal preference to avoid radical surgery. Patients with imperative indications have been shown to have increased recurrence rates and lower OS following percutaneous tumor resection. 16 By definition, these patients would have been better served with RNU due to high-risk pathology at presentation or have progressed to a higher-risk disease and were not able to have an appropriate RNU. Interestingly, we did not find imperative indications alone to be a risk factor for recurrence or progression to RNU. However, imperative indications against radical surgery were ultimately an independent risk factor for death. Again, imperative indications against RNU (CKD and poor surgery risk) likely act as a surrogate for patients with multiple serious comorbidities and an overall higher risk of noncancer-related death. It is notable that 90% of our imperative patients were able to preserve their affected kidney and renal function, with a median survival of 59.6 months after diagnosis.
The roll of BCG in the UTUC treatment algorithm is unclear. Retrospective series have shown 73% to 91% reductions in progression to RNU after BCG in the setting of upper tract carcinoma in situ (UT-CIS). 17 –19 However, the success of BCG with UT-CIS may be inflated if conversion of a positive to negative cytology is considered a complete response due to the imperfect sensitivity of urine cytology. Alternatively, adjuvant BCG patients with papillary tumors (Ta/T1) have not demonstrated a reduced risk of recurrence and progression, or improved survival. 5,17,18 In this present study, 61% of patients received BCG following their initial resection. Relative to those who received no intraluminal therapy, we found no difference in RFS, progression to RNU, or OS even after controlling for grade and stage. Our findings and the available literature support limiting BCG to primary treatment in patient with UT-CIS, with no benefit following resection of papillary UTUC to prevent recurrence, progression, or death.
In our previous publication, tumor grade was associated with decreased OS, but was not able to significantly predict subsequent recurrence or progression. 5 The larger number of patients with HG disease (45%) and longer follow-up in the present study demonstrate that tumor grade is indeed a significant predictor of recurrence (HR 2.06), with median RFS of 3 years for HG vs nearly 6 years for LG. In addition, HG disease continues to predict decreased OS (Fig. 2). However, when controlling for age, imperative indications, and a history of bladder cancer, tumor grade loses significance (Table 3). Our findings suggest that patients with advanced age, medical comorbidities, or a history of bladder cancer should not be denied conservative management if they have HG UTUC. They would additionally benefit from preserved renal function to remain eligible for platinum-based chemotherapy in the event of advanced urothelial carcinoma. 11,20
Perhaps the most important questions when deciding on appropriate treatment is to consider what is lost by electing endoscopic management over immediate RNU. A meta-analysis of eight case-controlled studies found no difference in cumulative cancer-specific survival (CSS) or OS between endoscopic resection vs RNU, although overall quality of evidence was poor with significant heterogeneity. 21 Moreover, the studies suggesting poorer OS for endoscopically managed patients were all plagued with selection bias as endoscopic patients were older and had worse performance status than those undergoing RNU. 22 Subset analysis of the remaining studies showed a favorable RFS for patients with HG disease undergoing RNU with no difference for LG. 21,23 –25 An important point to consider is that even though patients undergoing endoscopic management may have a moderate likelihood of recurrence, these recurrences can frequently be managed endoscopically without RNU. Our latest recurrence occurred nearly 10 years after resection illustrating the need for lifelong surveillance. The low probability of disease progression spares most patients the risk and consequences of radical surgery, and in the event of delayed RNU, no difference has been shown in CSS or OS. 26
Several limitations of this study should be mentioned. Preeminently, its retrospective nature limits us to capturing and reporting on patients who were felt at the time to be eligible for percutaneous tumor resection imparting a selection bias. In addition, certain tumor characteristics have more recently gained appreciation as predictors of prognosis in the literature such as tumor size and multifocality. These details were not prospectively recorded for all patients and could not be included in our analyses. Grading of urothelial cancers had changed near the midpoint of this series, which required converting grades 1 and 2 into LG and grade 3 into HG for the purposes of comparison. Without a centralized rereview of all earlier specimens, grade 2 tumors may have been inadvertently downgraded and have skewed results. 27 Our study included patients who underwent an initial percutaneous resection of an upper tract tumor primarily, including tumors located in the renal calyces and pelvis, or proximal ureter. Our findings may not be applicable to mid- or distal ureteral tumors accesses through a retrograde approach. Last, surgical technique, instrument quality, and cross-sectional imaging utilization have progressed over the 30-year span of this study. Coupled with a progressive appreciation for the role, minimally invasive surgery in urologic oncology and the cumulative experience our institution has acquired during this time, there is considerable heterogeneity in the management of patients with UTUC in this study.
Conclusion
In this large series spanning three decades of experience, we confirm that UTUC tumor grade continues to be an independent predictor of disease recurrence; however, age, medical comorbidities, and a preexisting history of bladder cancer are the ultimate drivers of OS. Adjuvant BCG does not mitigate the risk of recurrence, RNU, or death regardless of tumor grade. Nephron-sparing endoscopic resection continues to be an increasingly relevant choice for the management of patients with UTUC by allowing nearly 90% of patients to avoid RNU and preserve renal function. However, patients electing percutaneous tumor resection should undergo prolonged surveillance given the risk of late recurrences.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.