
Abstract
Objective:
Digital tomosynthesis (DT) is a new X-ray-based imaging technique that allows image enhancement with minimal increase in radiation exposure. The purpose of this study was to compare DT with noncontrast computed tomography (NCCT) and to evaluate its potential role for the follow-up of patients with nephrolithiasis in a nonemergent setting.
Methods:
A retrospective review of patients with nephrolithiasis at our institution that underwent NCCT and DT from July 2012 to September 2013 was performed. Renal units (RUs) that did not undergo treatment or stone passage were randomly assigned to two blinded readers, who recorded stone count, size area (mm2), maximum stone length (mm), and location, for both DT and NCCT. Mean differences per RU were compared. Potential variables affecting stone detection rate, including stone size and body mass index (BMI), were evaluated. Interobserver agreement was determined using the intraclass correlation coefficient to measure the consistency of measurements made by the readers.
Results:
DT and NCCT demonstrated similar stone detection rates in terms of stone counts and stone area mm2. Of the 79 RUs assessed, 41 RUs showed exact stone counts on DT and NCCT. The mean difference in stone area was 16.5 mm2 (−4.6 to 38.5), p = 0.121. The mean size of the largest stone on NCCT and DT was 9.27 and 8.87 mm, respectively. Stone size and BMI did not cause a significant difference in stone detection rates. Interobserver agreement showed a strong correlation between readers and adequate reproducibility.
Conclusion:
We found DT to be a comparable imaging modality to NCCT for the detection of intrarenal stones, without a significant effect from stone size and BMI and adequate reproducibility between multiple readers. DT appears to be an ideal alternative for following patients with nephrolithiasis due to its acceptable stone detection rates, low radiation exposure, and decreased cost compared to NCCT.
Introduction
N
Digital tomosynthesis (DT) is a new technology, based on conventional X-ray tomography that may reduce both radiation exposure as well as cost of imaging during follow-up of patients with nephrolithiasis. The primary use of this new technology has been in chest radiography and breast imaging. 4 Recent reports have described the use of DT for the detection of nephrolithiasis and this imaging study has been found to be superior to kidney, ureter, and bladder radiograph (KUB) for intrarenal stone detection. 5 In addition, DT has been used during intravenous pyelography and has demonstrated improved image quality and diagnostic potential compared to standard tomograms. 6 The increase in intrarenal stone detection rates, low radiation, and reduced cost of DT make it an ideal imaging modality for the long-term follow-up of patients with nephrolithiasis.
There are currently no reports to our knowledge comparing DT to NCCT for the detection of nephrolithiasis in a nonacute setting. It has been our practice to use DT to follow our recurrent stone formers in our Stone Center as well as for the assessment of postoperative stone-free status. We therefore determined the diagnostic accuracy of DT compared to NCCT for patients seen in a metabolic Stone Center.
Material and Methods
Protocol
Following the Institutional Review Board approval, we performed a retrospective review of patients with nephrolithiasis who underwent NCCT and DT at our institution from July 2012 to September 2013.
We identified patients with renal calculi who underwent NCCT and DT using ICD9 and CPT codes at our institution. Renal units (RUs) of patients over 18 years, which underwent NCCT and DT within 6 months were selected (RU = 124). Those RUs that underwent treatment or had spontaneous stone passage were excluded, eliminating 45 RUs. We recorded the imaging time interval and body mass index (BMI) (kg/m2) for each of the 62 patients.
The studies were reviewed by two fellowship-trained endourologists (Reader 1 and Reader 2). Readers were blinded to patient identifiers and official radiology reports. The 79 RUs were divided between the two readers for independent review. Reader 1 was assigned 40 RUs, whereas Reader 2 was assigned 39. All DT images were reviewed first, followed by NCCT images, and data were entered into a database where stone count, location, burden, and maximum stone length (largest stone) per RU were recorded. Stone burden was defined as total stone area (mm2) per RU and calculated by multiplying stone length (mm) by stone width (mm). Length (mm) and width (mm) was measured in the crainocaudal and transverse dimension, respectively. Stone size was determined directly on DT images and NCCT coronal reconstructions. Location was described per stone in terms of renal calix, renal pelvis, or proximal ureter. To assess agreement between readers, 18 RUs were randomly selected from the original 79 RUs. Each reader independently evaluated the NCCT and DT for each of the 18 RUs and recorded stone count, maximum stone length, and stone location.
Imaging technique
NCCT was performed with the LightSpeed® 64-slice Volume NCCT according to our institutional stone protocol. The settings used were 120 kVp, automatic tube current modulation with a maximum of 700 mA, noise index of 17.5, and 5 mm axial and coronal reconstructions, with a pitch of 1.375:1.
A GE Definium 8000 was used to perform DT. Two scout images of the upper and lower abdomen are first collected before DT. A computer-controlled motorized tube crane moves the X-ray tube to a series of positions along a horizontal path, acquiring a projection image on a flat-panel detector at each position. Figure 1 shows the basic setup for the DT device. Following a single tomographic sweep, the flat-panel detector collects all the data and software recreates a number of coronal images at a fixed slice thickness. DT images were acquired in the anterior-posterior view at 85 kVp, 630 mA, and a 14.2° sweep angle. Approximately 17 slices per patient were obtained, with a 3-mm slice interval and 5.5 seconds of scan time.

Diagram shows DT setup with direction of X-ray tube motion. DT = digital tomosynthesis
Data analysis
Determining the mean difference in stone counts, stone area, and maximal stone length per RU compared the stone detection capability of DT and NCCT. Mean differences are presented as a mean of NCCT minus the mean of DT. A positive and negative mean difference indicates DT underestimation and overestimation, respectively. Mean differences were reported with their corresponding confidence intervals. A two-tailed paired t-test was used to assess this difference, with p < 0.05 considered statistically different. Agreement was determined using a Pearson correlation test, with −1 and +1 corresponding to complete correlation and 0 equaled to no correlation. Statistical analysis was performed using R (version 3.1.3).
Stone detection capability for NCCT and DT was estimated by analyzing mean differences in stone count and area (mm2) per RU. The effects of stone size and BMI on stone detection were also evaluated. To determine the effect of stone size, we classified RUs based on the largest stone found on NCCT per RU into the following: <5, 5–10, and >10 mm. BMI was as a continuous parameter. Mean differences were analyzed by performing a paired t-test and Pearson correlation testing. Statistical analysis was also performed using R (version 3.1.3).
Interobserver agreement was determined to measure the consistency, or conformity, of measurements made by the readers. The intraclass correlation coefficient (ICC[3,k]) was used for two-way mixed average measurements and was calculated using SPSS (version 22.0). The ICC can be interpreted as follows: 0–0.2 indicates poor agreement; 0.3–0.4 indicates fair agreement; 0.5–0.6 indicates moderate agreement; 0.7–0.8 indicates strong agreement; and >0.8 indicates almost perfect agreement.
Results
A total of 62 patients and 124 RUs were identified. We included 79 RUs that met inclusion criteria, with a mean time interval of 80.6 days between NCCT and DT (Table 1). Stone location was mostly intrarenal, except for seven proximal ureteral stones detected by NCCT and one detected by DT (Table 2).
DT = digital tomosynthesis; RUs = renal units.
Of the 79 RUs assessed, 41 (52%) showed the same number of stones in NCCT and DT. For the remaining RUs, DT showed more stones in 22 RUs and NCCT revealed more stones in 16 RUs. The mean stone count per RU on NCCT and DT was 4.27 and 4.446, respectively. The mean difference in stone count was −0.19 (−0.47 to 0.08), p = 0.160.
When evaluating stone burden, mean stone area per RU on NCCT and DT was 140.35 and 123.85 mm2, respectively, with a mean difference of 16.5 mm2 (−4.6 to 38.5), p = 0.121. Mean maximum stone length per RU was 9.27 mm for NCCT and 8.87 for DT, with a mean difference of 0.39 mm (−0.16 to 0.99), p = 0.157 (Table 3).
Although not statistically significant, there was a correlation toward a higher mean stone size difference for larger stones and a negative correlation in stone count for larger stones (Tables 4 and 5). The stone count and stone burden (area) difference were not affected by BMI and correlation was 0.06 and 0.05, for stone count and stone area (mm2), respectively (Figs. 2 and 3).
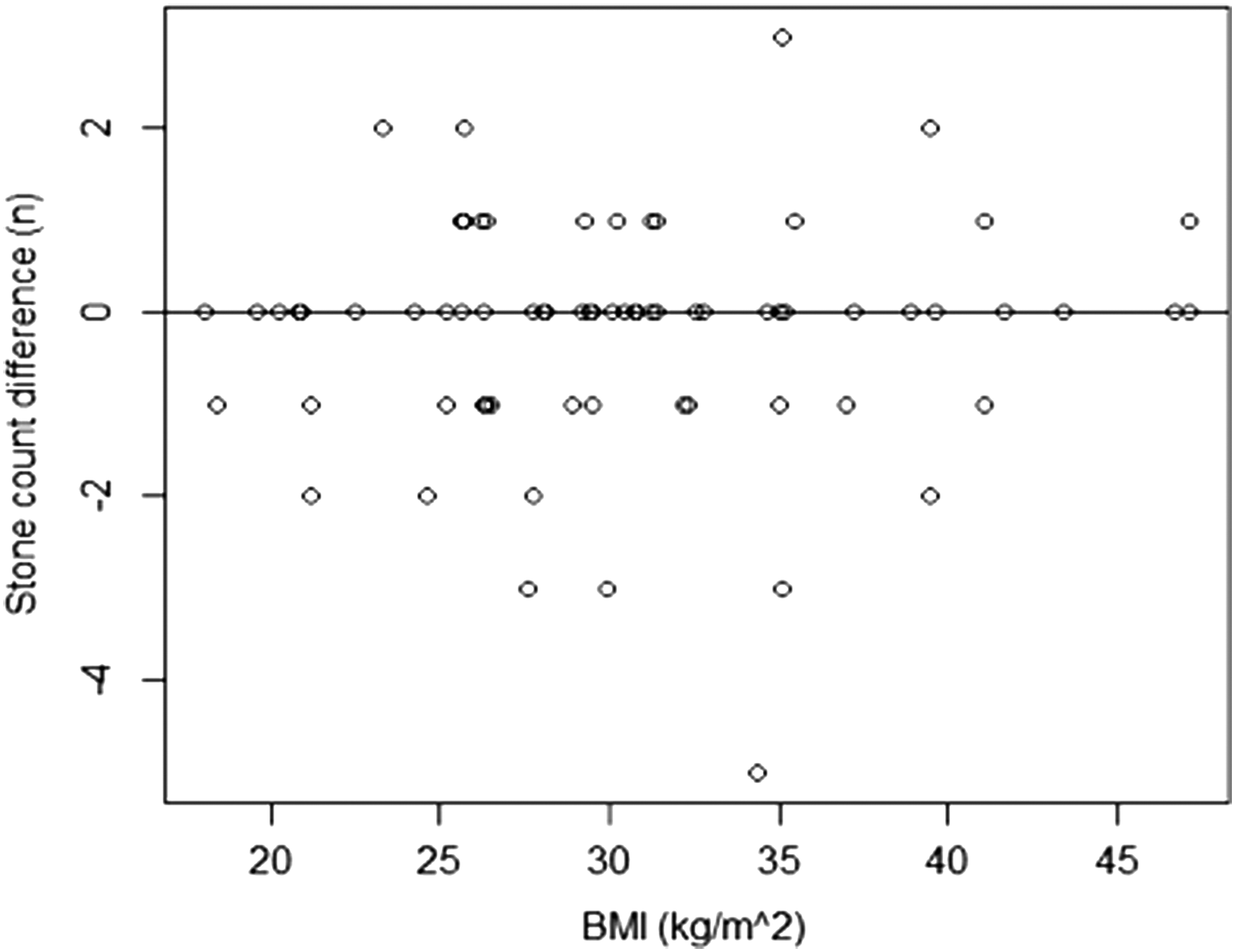
BMI effects on stone count mean difference from CT and DT. BMI = Body mass index.

BMI effects on mean stone burden difference (stone area mm2) from CT and DT.
Interobserver agreement for the 18 RUs evaluated by both readers was achieved. The ICC showed a strong correlation between readers for measuring stone size and detecting stone counts (Table 6).
ICC = intraclass correlation coefficient.
Discussion
Follow-up imaging in an outpatient setting is an essential tool to assess response to medical stone therapy, detecting both residual stone growth and new stone formation. Plain KUB with or without tomograms or renal ultrasonography is low cost, with low radiation modalities, low specificity, and low sensitivity. NCCT imaging in the outpatient setting may provide improved assessment of stone activity, with an increased cost and higher radiation dose than plain abdominal imaging or sonography.
In the past decades, there has been a widespread use of CT imaging for the assessment of renal and ureteral calculi. The increasing use of CTs in the United States, especially in the acute setting has become a cause of concern for radiation exposure to the population. 7,8 As the prevalence of nephrolithiasis continues to increase, 9 patients with recurrent nephrolithiasis are at high risk for increasing radiation exposure.
Measures to reduce the radiation exposure for these patients are critical. Proper selection of imaging studies and the use of low-dose CT have shown to decrease radiation exposure, although keeping stone detection comparable to standard CT. 10,11 Potential barriers for the use of low-dose CT in the follow-up of patients with nephrolithiasis include high cost and reported decrease in stone detection with BMIs greater than 30. 11
With DT, a series of low-dose projection images are acquired with a digital detector during a single sweep of the X-ray tube. The data is later reconstructed using computational software, which can also remove overlying structures and provide depth information about the structure of interest. 12 In comparison, conventional tomography requires multiple sweeps at different angles to focus at different depths and is associated with increased radiation exposure. 13 Postimage processing allows for reconstruction of high-resolution images at different coronal depths or high-resolution “slices,” which potentially could improve sensitivity for stone detection (Fig. 4).

Comparison between NCCT
DT may be an ideal tool for follow-up of patient with nephrolithiasis in an outpatient setting and recent reports have shown its superiority to standard KUB. 5 DT may also be useful for estimating residual stone burden following treatment. The advantages of this new imaging modality are likely due to high resolution of images, depth information, and removal of surrounding structures that hinder stone detection, including bowel gas and stool, with low radiation exposure to the patient. A recent report showed that low-dose CT was associated with more than triple the radiation exposure than DT. This study also reported that low-dose CT was eight times as expensive as DT. 13
In our study, we found that DT had similar intrarenal stone detection capability compared to NCCT. Both stone area and stone counts were similar between DT and NCCT. Maximum stone length by RU was also highly correlated by DT and NCCT. In prior studies, smaller stone size has been reported to contribute to decreased stone detection rates with DT. 5 DT had similar detection capability in terms of stone counts and burden, compared to NCCT. For larger stones, there was a correlation for DT to underdetect stones and overestimate stone size, but this effect was not statistically significant. This is likely due to irregularity in measuring large branched stones.
BMI has been previously linked with decreased stone detection rates of low-dose NCCT in obese patients. According to recent AUA guidelines, patients with elevated BMIs should undergo standard NCCT, which significantly increases radiation exposure to the patient. 11 In addition, obesity has been shown to increase radiation dose to patients from NCCT, with certain protocols delivering up to triple radiation exposure in obese compared to nonobese patients. 14 The current study evaluated the effect of BMI in stone detection rates for NCCT and DT and showed that BMI did not affect stone detection. We did not evaluate the effect of obesity on radiation exposure from DT, and further studies should be performed to evaluate this effect.
Currently, at our institution, DT images are focused on the kidney and proximal ureter, so distal ureteral stones are not visualized. In our analysis NCCT detected seven proximal ureteral stones and DT only one. This discrepancy was likely due to failure of DT to detect secondary obstruction signs, including hydronephrosis and perinephric fat stranding. Current AUA guidelines still recommend NCCT for the initial evaluation of acute renal colic, but recent investigations have challenged this recommendation. A recent study randomized patients with acute stone episodes presenting to the emergency room to undergo renal ultrasound or NCCT. 15 This investigation showed that patients who underwent an initial renal ultrasound did not have increased morbidity, including complications, return visits, or hospitalizations. These results are limited because they did not apply to a selected high-risk population and most patients eventually underwent an NCCT to assess stone size and location. Ultrasonography might be useful in select individuals, including pediatric patients, and recurrent stone formers; and combination of ultrasonography with DT might increase the stone detection rate. Nevertheless, in our stone center, we continue to perform low-dose NCCT for evaluating acute stone episodes.
Despite DT being a new technology, there was acceptable intraobserver and interobserver agreement between the readers. This finding suggests adequate reproducibility and short learning curves for DT. The potential limitations of our study include its retrospective nature and the interval of 80 days between DT and NCCT. This time interval could allow for asymptomatic passage of stones and natural stone growth. In addition, no standard or control of stone count and size was used; so imaging study sensitivities and specificities could not be accurately calculated. Although not statistically significant, there was an increase in mean stone count on DT compared to NCCT. This finding could be a result of overreading and potential stone growth since 50 of the 79 RUs underwent initial imaging with NCCT followed by DT at a later date. Despite these limitations, this is the first study to compare DT to NCCT and demonstrate equality in stone detection. Further studies are necessary to determine sensitivity and specificity of digital tomosythesis in determining stone activity in recurrent stone formers.
Conclusions
We found DT to be comparable to NCCT in detection of intrarenal stones in an outpatient setting. Stone burden and maximum stone length measurements were equivalent between studies. Variables, including stone size and BMI, had minimal effects on this correlation. DT appears to be an ideal alternative for following patients with nephrolithiasis due to acceptable stone detection rates, low radiation exposure, and decreased cost compared to NCCT.
Footnotes
Author Disclosure Statement
No competing financial interests exist.