
Abstract
Objective:
Traditionally, fluoroscopy or ultrasound (US) or both are used for guiding tract creation during percutaneous nephrolithotomy (PCNL). However, the use of fluoroscopy inevitably incurs radiation exposure, which should be cut down as much as possible in view of its potential adverse effects on health: both deterministic effects and stochastic effects. Conventional US guidance, being radiation free, can serve the purpose, but it is difficult to visualize the needle tract during screening without a needle-guiding system fixed to the transducer, and hence, there is a lack of predictability and sense of security. The objective of this study is to assess the feasibility of using US with navigation system (USNS) to solve the above problems.
Patients and Methods:
In 2014, we performed PCNL on 18 patients with USNS guidance. During the puncture step, the magnetic field-based navigation US could help visualize the position of the needle tract in relation to the target calix. The procedure was done in free hand without the usage of needle-guiding system attached to the transducer. Needle deviation could be detected and adjusted immediately to achieve precise puncture.
Results:
Of the 18 patients, 83.3% (15/18) of them had their punctures effectively done with a single attempt. Three puncture procedures were performed by two urologic trainees without any previous USNS experience. The mean fluoroscopy time during dilatation was 74.6s, with no radiation at all during the puncture step. The stone clearance rate was 72.2%, with 66.7% (12/18) being tubeless procedures. The mean length of hospital stay was 4.8 days. No immediate complications related to the puncture procedure were found.
Conclusions:
USNS can provide radiation-free guidance for tract creation in PCNL. It is predictable, precise, reliable, and safe. Most importantly, the technique is easy to learn, particularly for urologists who are new to PCNL.
Introduction
P
Materials and Methods
In 2014, we prospectively performed PCNL with USNS guidance in 18 patients presented with renal stones. The US machine with the built-in navigation system (MyLab Twice by Esaote, Milano, Italy) is shown in Figure 1. The machine is connected to a US transducer, a magnet, and an electronic puncture needle separately. There are two sensors in the system: one inside the electronic needle and one attached to the US transducer as in Figure 2. Under the magnetic field created by the magnet placed close to the operative field in the prone position, the US can visualize the exact position of the needle tract in relation to the target renal calix on the screen. The size of the electronic needle is 16-gauge with outer metal sheath for passage of guide wire. When puncturing along the renal plane in a longitudinal cut, the US screen will show the green outline of the needle and the predicted trajectory in the yellow line. (Fig. 3) If the needle is out of the plane of the ultrasound transducer, all the green and yellow signals will disappear. Hence, immediate fine adjustment of the needle is allowed until the target calix is reached. With retrograde blue-dyed physiologic saline flushing through the ureteral catheter placed beforehand, the solution will come out through the sheath once the needle together with the sensor is removed. The hydrophilic guide wire is then passed through the remaining sheath for subsequent tract dilatation under fluoroscopic guidance similar to the conventional PCNL.

US machine with navigation system from Esaote. US = ultrasound.
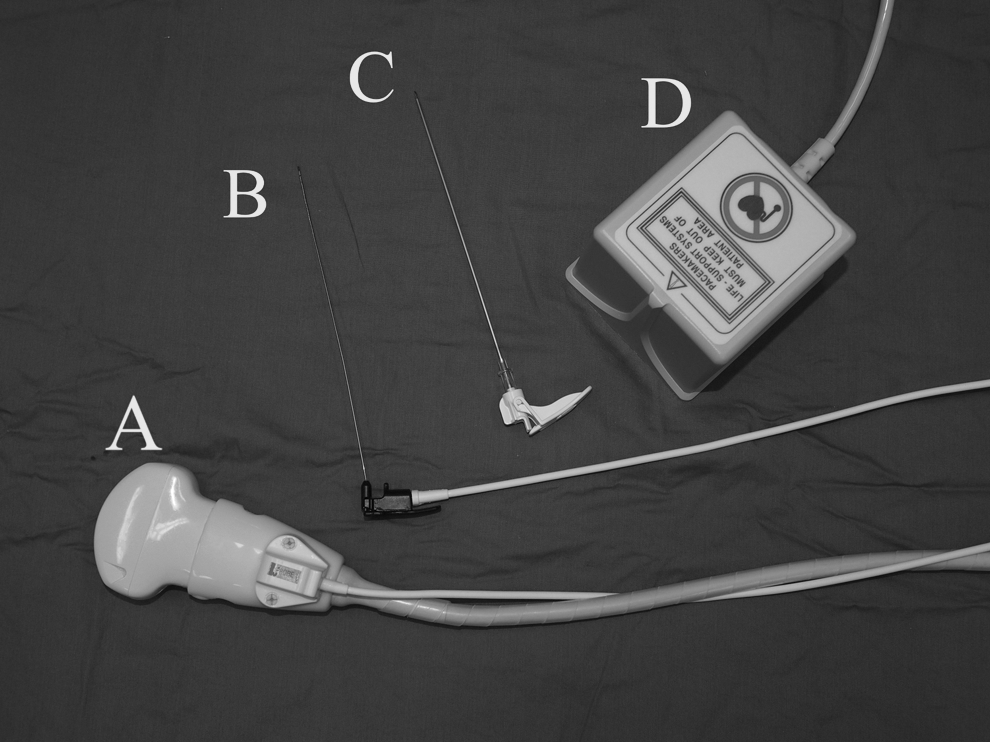
Basic accessories.

Ultrasonic view of needle position (“needle shaped” outline is the actual needle outline; “straight line from the tip of needle outline” is the predicted trajectory) and intraoperative view of percutaneous nephrolithotomy puncture along the same plane of US transducer.
All the punctures were done by a single surgeon who is either a specialist or a trainee under the same specialist's supervision. The specialist mainly used X-ray or X-ray plus US simultaneously as guidance in previous PCNL. Patient's demographic data, including sex, age and comorbidities, stone size, Hounsfield unit, and position, were collected. The stone size is defined by the maximal dimension of the largest stone in preoperative plain CT or intravenous urogram. The degree of hydronephrosis was also assessed. Fluoroscopy time was measured to reflect the amount of radiation exposure. The stone clearance status and complications were assessed as well. Stone clearance is defined as the achievement of a clinically insignificant stone fragment of size 4 mm or below by the postoperative kidney, ureter, and bladder radiograph, as all the stones are radiopaque. The continuous data are presented in mean ±1 standard deviation (range) and the categoric data in percentage. Student's t test will be used to compare the pre- and postserum hemoglobin and creatinine level. SPSS version 18 was used to analyze the data.
Results
The mean stone size in the series was 2.3 cm (1.0–7.5 cm), and stone position included a single pole to full staghorn (Table 1). Concerning the puncture, 15 cases were done by a single specialist and 3 were by 2 trainees who had minimal experience with conventional US-guided puncture in PCNL and were completely new to USNS. No fixed needle-guiding system was used in all cases. The two trainees were able to make effective punctures in a single attempt only. Overall, 15/18 (83.3%) of the punctures were achieved in one single attempt, while the remaining 3/18 (16.7%) were achieved by two attempts. Concerning the issue of radiation exposure, no radiation was used during the puncture step at all. The mean fluoroscopy time for tract dilatation was 74.6 seconds. Other results are shown in Table 2. Although there was a statistically significant drop in serum hemoglobin level, it was clinically not significant. In this series, one Clavein III complication (5.6%) was identified. The patient was readmitted for hematuria due to secondary hemorrhage and found to have pseudoaneurysm by angiogram. Highly selective embolization was performed effectively in this case. Otherwise, only one Clavein I complication (4.3%) was found among the rest cases.
DM = diabetes mellitus; HT = hypertension; IVU = intravenous urogram; SD = standard deviation.
PCNL = percutaneous nephrolithotomy; SWL = extracorporeal shockwave lithotripsy; USNS = ultrasound with navigation system.
Discussion
Several studies have reported that outcomes of PCNL are highly associated with the puncture step. 2,6,7 An ideal renal access allows an optimal working angle for complete stone removal and facilitating handling of surgical instruments while minimizing the risk of bleeding and complications such as injury to the kidney and contiguous organs. 7 Both fluoroscopy and conventional US have problems as guidance in PCNL. The former involves radiation, which can create adverse health effects: deterministic effects and stochastic effects to humans. 8 This is an important issue to address as patients suffering from nephrolithiasis are unavoidably exposed to significant radiation during both diagnostic and therapeutic phases. A study reported that the amount of radiation exposure for a patient presented with a primary acute stone event was estimated to be 29.7 mSv from diagnostic imaging over a 1-year period. The majority of this radiation was from CT imaging, and each patient underwent a mean of 1.7 CT scans in the period. Twenty percent of patients were exposed to greater than 50 mSv, which exceeds the recommended 1-year maximal occupational radiation exposure set by the International Commission on Radiation Protection (ICRP). 9 Another study analyzed surgeons' radiation exposure in PCNL, where the mean doses to a urologist's eyes, fingers, and collars were measured as 26, 33.5, and 48 μGy per procedure, respectively. The mean effective dose per procedure for a urologist was 12.7 μSv. 10 Despite the fact that the amount of radiation exposure during the PCNL procedure seems to be minimal while referring to the ICRP recommended occupational dose limit of 20 mSv per year, it will be a real concern when the number of PCNL procedures increases with time. 11,12
Conventional US is the best alternative way of guidance. However, it may be technically difficult due to the poor visibility of the needle during screening. 13 As a result, there may be discrepancy between the actual needle position and the target site. Fast to and fro movement of the needle for a few millimeters is of widespread use as a means for localization of the needle tip. This maneuver can cause microtraumatization of the parenchyma and inadvertent injury of arteries leading to hematoma formation. 14 –16 Although the needle position can be predictable with a needle-guiding system fixed to the transducer, the angle of entry into the caliceal system is limited. A study revealed that the learning curve for PCNL surgical competence is estimated to be 60 cases. 6 In our series, three punctures were effectively done by two trainees who have minimal experience in using conventional US and no experience in USNS. All can be achieved with one attempt suggesting that the learning curve is unlikely to be a major issue when using USNS. However, for an experienced surgeon in US-guided PCNL, the added benefit is not known.
Huber et al. reported the first experimental study on electromagnetic tracking for percutaneous renal access in 2011, and Rodrigues et al. reported the first in vivo study on electromagnetic tracking for percutaneous renal access using a pig model. 17,18 Menhadji reported a similar tracking technology in patients undergoing renal mass biopsy using a different design of transducer, which can be carried out in an office setting. The design and the simple setting can potentially be used in creating tract during PCNL. However, the angle of entry was limited at 0°, 15°, and 30° only by the transducer design. 19,20 For our method described, there is an improved degree of freedom in choosing the angle of entry and this electromagnetic tracking technology can potentially be a great help in guiding PCNL puncture in patients with complex stone anatomy. Although one case was readmitted for pseudoaneurysm, it is unlikely to be related to the method of guidance chosen. In general, it is at least as safe as conventional guidance methods. A study reported that electromagnetic systems may be susceptible to environmental interference in the operating room. 21 We experienced no interference so far that would hamper the tracking information.
Conclusions
USNS can provide a feasible alternative way of guidance for tract creation in PCNL. It makes the puncture step absolutely radiation free and minimizes the radiation exposure to the patient, the surgeon, and the surrounding supporting staff. Moreover, it is highly predictable, precise, reliable, safe, and allows complete freedom of needle placement. Most importantly, the technique is easy to learn, particularly for urologists who are new to PCNL or with limited experience on the US-guided PCNL. However, for better evidence to be shown, a prospective randomized controlled trial is required to compare it with conventional guidance methods in future.
Footnotes
Author Disclosure Statement
No competing financial interests exist.