
Abstract
Objectives:
To evaluate if thulium laser enucleation of bladder tumor (ThuLEBT) offers any advantage over monopolar resection of nonmuscle-invasive bladder cancer (NMIBC) without increasing complications.
Patients and Methods:
From February 2012 to September 2013, 58 patients (41 males and 17 females) newly diagnosed with having a single papillary bladder tumor more than 1 cm in diameter were selected for this prospective study on ThuLEBT. A similar historical cohort of 61 patients who underwent traditional monopolar resection (TURB-T) of NMIBC (Group B) was used to compare the two procedures.
Results:
Mean tumor diameter in the ThuLEBT group was 2.5 cm (range 0.5–4.5). Mean operative time was 25 minutes (range 12–30). Re-resection and cold cup biopsy of the tumor base (in 90 days) were negative for bladder cancer (BC) persistence or recurrence in all patients with NMIBC treated with ThuLEBT. In Group B, seven patients were found with disease persistence. In eight cases of TURB-T patients, no detrusor muscle was identified, while it was always easily identified in the ThuLEBT group. No patient in Group A experienced obturator nerve reflection intraoperatively and no bladder perforation was evidenced in dome-located neoplasm; when involved, ureteral meatus was sharply excised without subsequent postoperative evidence of distortion. No significant intraoperative or postoperative bleeding occurred in all but one patient in the two groups.
Conclusions:
ThuLEBT may represent a potential alternative to TURB-T, which nowadays is considered the standard for diagnosis and treatment of NMBIC. In our study, ThuLEBT allowed accurate reporting of neoplastic depth invasion, suggesting the possibility to avoid a second-look resection at 90 days. All the different intravesical sites of the BC may be enucleated with the thulium laser, which offers advantages over the monopolar energy, especially when the tumor is located in the lateral bladder wall, at the bladder dome, or in the perimeatal zone.
Introduction
T
Surgical accuracy is paramount to the safety and efficacy of TURB-T, but technical and procedural considerations may also have an impact on outcomes. A second resection may improve staging and tumor removal, 2 particularly where the primary procedure was affected by multiple tumors, large tumor bulk, bleeding during resection, bladder perforation, patient habitus, or anesthetic risk, or if the patient has high-risk bladder tumor, T1 tumor, multiple high-grade Ta tumors, or carcinoma in situ.
The standard TURB technique involves piecemeal resection of the tumor, which runs counter to established oncological principles of removing the tumor intact as the piecemeal approach liberates tumor cells into the bladder. In view of this issue and of the high rate of recurrence, several studies have examined the feasibility of a modified TURB to provide en bloc resection of the specimen based on the established oncological principle of dissecting through normal tissue.
The researched final results are to allow en bloc sculpting and resection of the tumor. We describe a technique of bladder tumor en bloc enucleation with a new double-wavelength thulium laser enucleation of bladder tumor (ThuLEBT). During cutting activity of the Multipulse Tm+1470 Thulium laser, diode and thulium laser work together, mixing their effects at the same time. This offers the possibility of a planned hemostatic enucleation through the bladder musculature and of a very efficient coagulation of the bed of resection. Results were compared with a historical control group treated by conventional TURB-T.
The aim of the article is to evaluate if this planned deep enucleation offers a more precise pathological tumor stage without increasing the risk of bladder perforation, pros and cons of the laser procedure with respect to tumor location and size, and its impact on the risk of tumor persistence at 90 days after re-resection with cold cup biopsy of the previous tumoral area.
Patients and Methods
From February 2012 to September 2013, 58 patients (Group A: 41 males and 17 females) newly diagnosed with having a single papillary bladder tumor more than 1 cm in diameter were selected for this prospective study on ThuLEBT. Mean patient age was 71 years (range 35–86). Exclusion criteria were multiple or recurrent nonmuscle-invasive bladder cancer (NMIBC), suspect of locally advanced BC (cT2 or higher) at CT examination, and/or distant metastases. A similar historical cohort of 61 patients who underwent monopolar resection of NMIBC (Group B) by the same surgeon from April 2011 to February 2012 was used to compare the two procedures (Table 1).
ThuLEBT = thulium laser enucleation of bladder tumor; TURB-T =transurethral resection of bladder tumor.
Preoperative evaluation included clinical history, physical examination, ultrasound examination of the bladder, flexible cystoscopy, and urine cytology. Abdominal computed tomographic scan was performed only in selected cases. All patients signed an informed consent.
TURB-T was performed according to the European Association of Urology (EAU) guidelines. ThuLEBT was performed with the patient in the lithotomy position under spinal anesthesia, with physiologic saline as continuous irrigation. A 600-nm laser fiber introduced in the working element of a 26F continuous flow resectoscope (Olympus, Hamburg, Germany) was used. The fiber was connected to the Multipulse Tm+1470 Thulium laser (Multipulse Tm+1470; Asclepion, Jena, Germany), equipped with a 1940-nm thulium laser, and an associated 1470-nm diode laser (Raman module). Laser was used in the continuous wave setting at 30 W with a thulium frequency of 50 Hz during the enucleation and switched to the 1470-nm diode laser during coagulation by a foot pedal. Procedural steps (Figs. 1 and 2) included first a circumferential tattooing incision around the tumor with a safety margin of normally appearing mucosa of ∼5 mm. After that the resection proceeded toward the deeper layers of the bladder wall (down to the adventitial layer), combining the laser incision with the blunt dissection of the resectoscope tip. The resection through the bladder wall was more superficial along the peripheral part of the tumor and proceeded deeply toward the adventitial plane, moving from the periphery to the center of the tumor base to enucleate the tumor. The tumor, along with its base, was retrieved in one piece through the resectoscope sheath, or sometimes by removing the entire resectoscope from the urethra, using a thick loop and engaging the fragment between the beak of the instrument and the thick loop. When the tumor size was >3 cm, it was necessary to incise longitudinally and/or across the lesion and the bladder wall at the base into two or more parts. This operation was performed before completing the resection, with the neoplasm still in situ, to reduce the risk of tumor cell scattering. After resection, the tumor base was uniformly coagulated using the 1470-nm diode laser in the pulsed-wave setting at 20 W. A 20F Foley catheter was inserted after the procedure with irrigation for 12 hours. The enucleated specimen was sent for histopathologic examination. The 2009 TNM classification and the 2004 World Health Organization grading system were used for histopathologic examination.

Main steps of ThuLEBT (illustrations courtesy of Dr. Migliari): tattooing
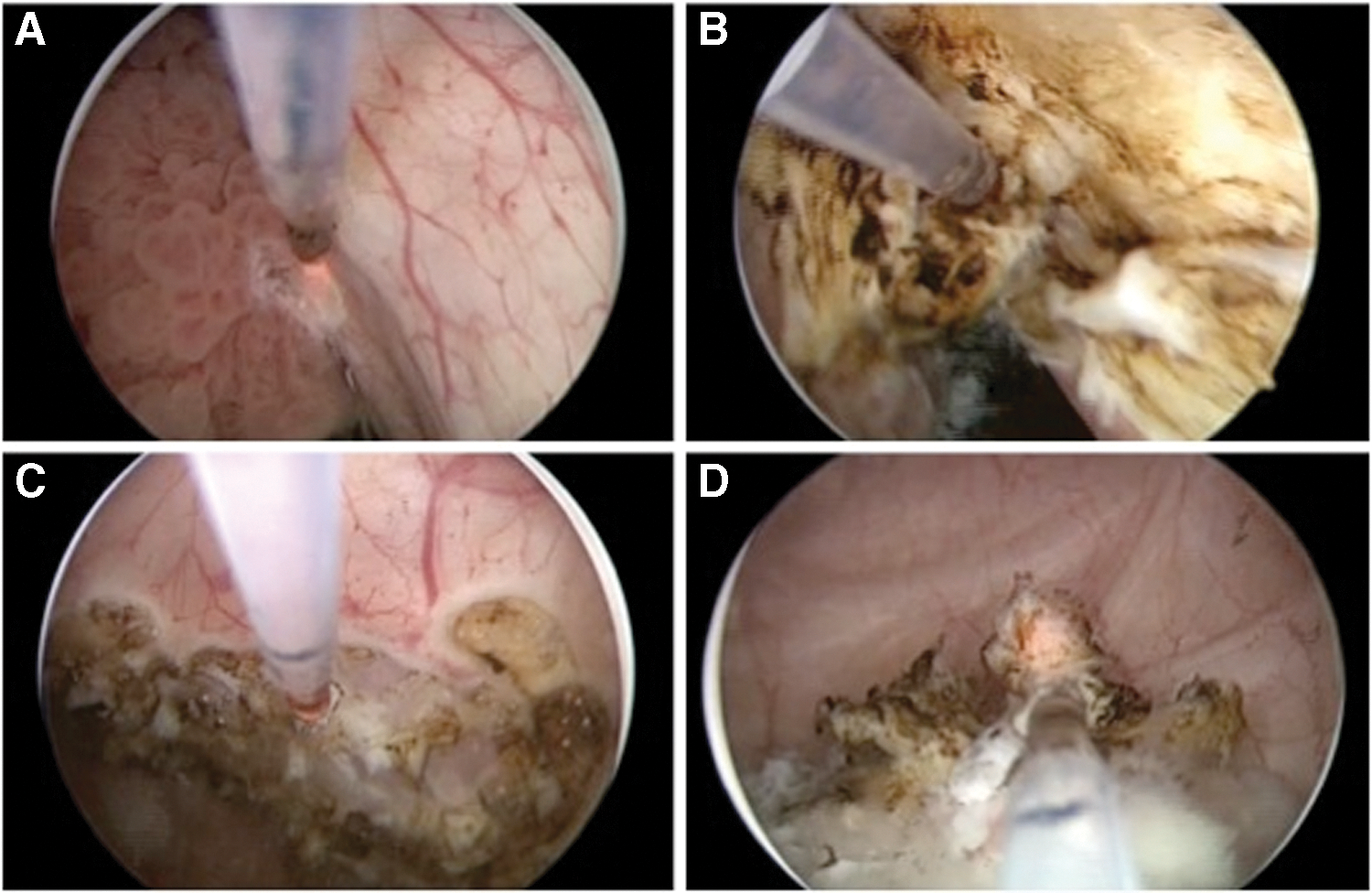
Thulium laser enucleation of a bladder dome tumor (intraoperatory view): tattooing
According to our research protocol, a second-look resection, preceded by a cold cup biopsy of the tumoral area, was performed within 90 days (see Results section) in Group A NMIBC patients and results were compared with the similarly treated historical Group B (conventional TURB-T). Statistical analysis was performed using the chi-square test. The p-value considered to be statistically significant was <0.05. Clavien–Dindo analysis of complications was adopted.
Results
Mean tumor diameter of the removed neoplasm in Group A was 2.5 cm (range 0.5–4.5). The neoplasms as much as 4.5 cm had a narrow base of implant. Figure 3 shows the depth of thermal damage induced by the laser energy on the bladder neoplasm base of implant.
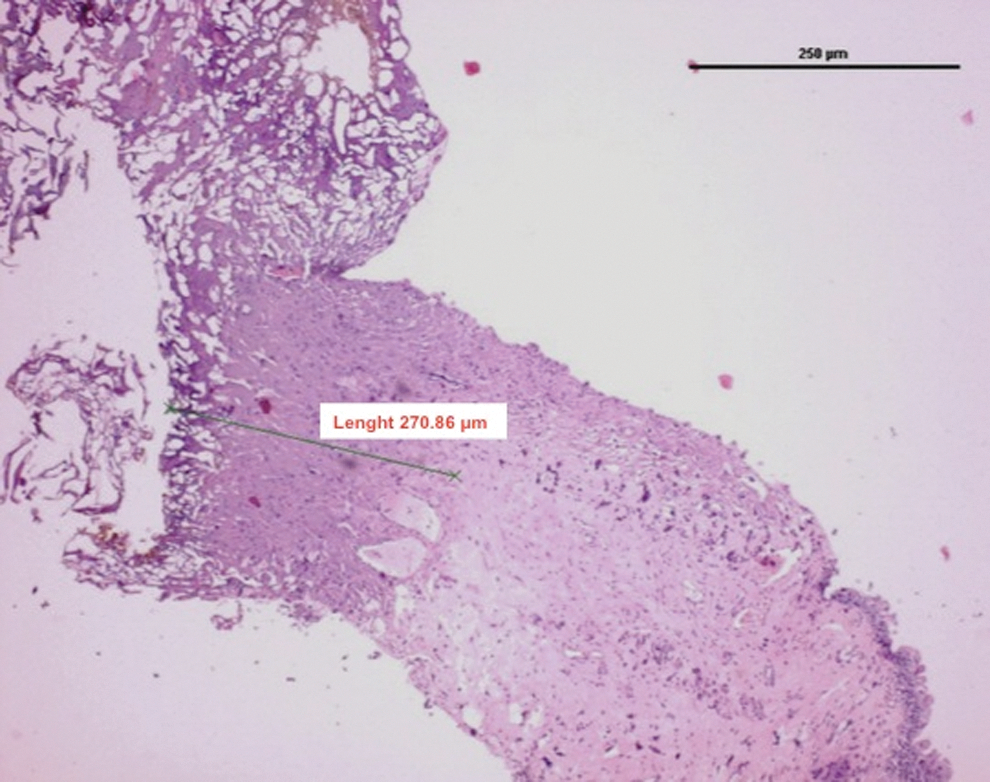
Histological aspect of the laser-induced thermal damage in a bladder neoplasm.
The neoplasms were located on the trigone (16 cases, 7 of them close to the ureteral meatus [UM]), left lateral wall (15 cases), right lateral wall (11 cases), posterior wall (14 cases), and bladder dome (12 cases). Mean operative time was 25 minutes (range 12–30). No patient experienced obturator nerve reflection intraoperatively. No significant intraoperative or postoperative complications occurred (Table 2).
According to the Clavien–Dindo classification for surgical complications, no complications occurred in Group A (Grade I), while two patients in Group B (TURB-T) required blood transfusions (Grade II) and one patient in Group B required an endoscopic hemostasis (Grade III).
In patients with papillary lesion covering the UM, after placing a nitinol guidewire into the meatus using the same laser fiber operative support, BC was removed in two cases enclosing the meatus itself, while in the remaining cases, UM was saved with great precision. In no cases was ureteral stenting necessary.
Mean catheterization time was 28 hours (range 24–32) in Group A and 38 (range 29–48) in Group B. Mean hospital stay was 47.5 hours (range 36–96) and 58.5 hours (range 40–98), respectively, in Groups A and B. Pathologic results in Group A showed urothelial carcinoma with stage Ta low grade in 30 patients (56.4%), T1 high grade in 23 patients (32.7%), and T2 high grade in five patients (10.9%). Apart from the neoplasm covering the UM, histopathologic evaluation demonstrated that the bladder detrusor was provided in all cases in Group A, while it was absent or not valuable (due to thermal artifacts), respectively, in five and three Group B patients. Re-resection and cold cup biopsy of the tumor base (in 90 days) was negative for BC persistence or recurrence in all patients with NMIBC treated with ThuLEBT, while positive tumor ground biopsies were found in seven of Group B patients. In three of them, there was an upstaging from Ta to T1, and in one case, from T1 to T2. After a mean follow-up of 20 months (range 13–25), we found recurrences in 12 of 58 patients (20.6%) of Group A, without progression in tumor grade. All recurrences were not at the primary resection site. The 18-month recurrence-free survival was 90% among patients with primary Ta BC and 76% in the group of patients with primary T1 BC. (p=ns). The risk of recurrence was similar to historical Group B TURB-T control.
Four of 12 patients with bladder neoplasms >3 cm who underwent splitting of their BC during resection had T2 high-grade BC and, consequently, underwent cystectomy. We had two recurrences at follow-up among the remaining eight patients who needed splitting during primary resection and five recurrences among the 46 patients who did not need tumor splitting. The difference was not statistically significant (p=0.6). In Tables 1 and 2 are reported the clinical features of historical control group (Group B) patients.
Discussion
Herr in 2005, after a previous report on the value of a second transurethral resection in evaluating bladder cancer patients, described residual rates of 15% to 53% at the second TURB and upstaging rates of 4% to 29% with muscle invasion. 3 In many cases that are upstaged after the second resection, it is apparent that muscle was not present in the original resection. The quality and result of the initial transurethral resection through a wire loop (TURB-T) strongly determine the patient's prognosis. An unshakeable principle of the surgical treatment of cancer is to dissect through normal tissue and to remove the tumor with a negative margin. Moreover, it has been demonstrated that TURB-T does affect the volume of viable tumor cell released during tumor resection in animals: conventional TURB-T released 620% more tumor cells than neodymium laser irradiation of the tumor. 4 Several studies have examined the feasibility of various en bloc resection techniques. Ukai et al. 5,6 described the technique almost 15 years ago, using a J-shaped needle electrode, while Saito 7 was the first to present results on a holmium:YAG laser en bloc resection of the tumor. Wolters et al. 8 adopted en bloc tumor enucleation as described by Ukai et al. using a thulium laser to perform the mucosal incision and were able to demonstrate detrusor muscle in all cases, proposing the potential for exact staging at the time of initial TURB-T.
Positive histopathological results were reported in conjunction with laser en bloc resection of bladder cancer. Lowering of thermal damage improved pathohistological staging. 9 Particularly, the application of thulium:yttrium-aluminum-garnet (Tm:YAG) showed precise cutting, thus avoiding tumor damage and this may contribute to explain the higher T1 NMBIC discovered in the ThuLEBT group if compared with the TURB-T historical cohort.
During cutting activity of the Multipulse Tm+1470 Thulium laser that we used, diode and thulium lasers work together, mixing their effects at the same time (this is a peculiarity of this laser). The clear and precise cutting effects of the thulium laser are related to its 1940 nm wavelength with ∼0.2 mm depth of thermal damage. The 1470-nm diode laser is readily absorbed by water, allowing for low-char hemostatic tissue removal with a thermal damage of about 0.4 mm. The mixed effects of the two lasers simultaneously seal off the blood vessels to minimize bleeding during cutting. Diode laser energy alone is activated during pure coagulation.
A further potential benefit of using the laser enucleation of the tumor over conventional wire-loop resection is that en bloc enucleation improves specimen orientation, making histological reporting more straightforward. The technique appears to allow accurate reporting of depth invasion, 10 and we also confirm that re-resection and cold cup biopsies of the tumor base in the ThuLEBT group did not alter the diagnosis or stage in any patients, confirming previous data. This means that as ThuLEBT allows accurate reporting of depth invasion, the need to restage bladder tumor at 30 to 90 days may be reevaluated.
Besides tumor size, one of the major drawbacks for laser en bloc resection has been the intravesical tumor localization. Several research groups excluded tumor resection at the bladder dome wall, which implicated the risk of peritoneal damage. 11,12 We do not agree with them as in our experience ThuLEBT was more easily and precisely conducted than monopolar TURB-T. The absence of bleeding allowed us to improve visualization of the different planes during anterior bladder wall enucleation, and as thermal injury due to thulium laser wavelength is only 0.2 to 0.4 mm in depth, the risk of transparietal thermal damage of the neighboring tissue (i.e., ileal loops) is negligible. Of great interest was also the possibility to sculpture the UM, avoiding the charring induced by monopolar energy in case of meatal bladder cancer. Even if seven cases are few, no distortion or stenosis of the meatus was evidenced at 90-day reevaluation of the tumoral area. Overall, six meatal BC cases treated by TURB-T resulted in one meatal stenosis. The absence of obturator kicks in patients with lateral wall neoplasm is another advantage of the laser energy evidenced by some authors. 12 –14 Comparing conventional TURB-T with Thulium laser en bloc resection of bladder tumors, a significant reduction of obturator nerve reflex-related bladder perforations was evident. Overall, eight obturator nerve stimulations resulted in three bladder perforations using conventional TURB-T in our experience.
Even if another drawback of en bloc resection is the fear of the complications due to the deepness of the treatment, to date, complications in conjunction with en bloc resections in literature have been described in only four of a total of 459 patients. This makes an overall complication rate of 0.7%, of which all complications had not been life-threatening. Intra-, peri-, or postoperative bleeding was rare in laser en bloc resections. This confirms the known powerful hemostatic effect of Tm:YAG laser, which led to a reduction in postoperative bladder irrigation time in comparison with conventional TURB.
Tumor size was also not a problem in our experience. While Nagele et al. extracted tumors as much as 2 cm, 15 Fritsche et al. performed en bloc resection for as much as 7.5 cm, showing that en bloc resection of tumors >4.5 cm is possible. 16 In our experience, although resecting tumors >3 cm, R0 resection was achieved in all our cases.
In addition, en bloc resection using monopolar current showed good results. 5 –7 In three of the initial four reports, all specimens were R0 and included detrusor muscle. However, in Ukai's second case series, 93% of the 90 patients revealed negative control biopsies from the tumor ground, 6 and of the remaining seven patients with positive tumor ground biopsies, five patients hat a pT2 tumor and two patients had a minimum pT1 tumor in the final histopathology. In addition, using this technique, the pathologic interpretation was limited in one of 11 tumors due to crush injury of a very small lesion, 17 and in five of 11 tumors, interpretation of detrusor muscle was not possible because of electrocautery injury. Finally, in spite of a decreased recurrence rate reported within the ThuLEBT group in comparison with conventional TURB-T, the significance level was not reached.
Conclusions
En bloc laser enucleation of bladder tumors is an interesting potential alternative to TURB-T, which nowadays is still considered the gold standard for diagnosis and treatment of NMBIC. The feasibility of laser en bloc enucleation without the risk of perforation has been demonstrated. All the different intravesical sites of the BC may be enucleated with the thulium laser, which offers some clear advantage over the monopolar energy, especially when the tumor is positioned in the lateral bladder wall or in the bladder dome or in the perimeatal zone. One advantage of the Multipulse Tm+1470 Thulium laser is that it allows for minimal transmural coagulative necrosis (about 0.2 mm) reducing the rate of perforation and extravasation and leaving a sharp boundary between the necrotic tissue and the surrounding tissue. A further potential benefit of ThuLEBT over conventional wire-loop resection is that it allows for accurate reporting of depth invasion, opening the way to reevaluate the need for restaging the bladder tumor at 90 days. Even if the recurrence rate was lower in the ThuLEBT group, the assumed oncologic benefits cannot be concluded from the available data in terms of recurrences as they are extremely heterogeneous with an obvious selection bias.
Footnotes
Acknowledgment
Dr. Roberto Migliari drew the anatomical pictures describing the ThuLEBT procedure.
Author Disclosure Statement
No competing financial interests exist.