
Abstract
Objective:
Paraganglioma (PGL) is a rare type of tumor that arises from the extra-adrenal paraganglia. Laparoscopic adrenalectomy is well established for the treatment of adrenal pheochromocytomas, but laparoscopic resection of PGLs is controversial. In this study, we compared the clinical outcomes of laparoscopic and conventional open surgical procedures for PGLs. We also analyze the safety and feasibility of laparoscopic technique for renal hilar PGLs.
Methods:
A retrospective review of all patients who underwent resection of retroperitoneal PGLs from 2002 to 2014 in our hospital was performed. Twelve patients underwent open procedures, and 15 underwent laparoscopic procedures. The preoperative, intraoperative, and postoperative data were collected and analyzed.
Results:
PGLs located at the renal hilum were predominantly both in the Lap group (n = 9) and open group (n = 7). Laparoscopic procedures in 14 of 15 patients were effectively completed without conversion to open surgery; one case with renal hilar tumor was converted to open surgery because of bleeding. The baseline characteristic of the patients in each group was well equivalent with respect to patient age, gender, body mass index, and tumor size. In the Lap group, the perioperative indexes were significantly different from those of the open group (each p < 0.05), including operative time (217.36 ± 51.90 vs 175.67 ± 36.79; p = 0.029), estimated blood loss (80.71 ± 83.52 vs 172.50 ± 160.86 mL; p = 0.047), and postoperative hospital stay (5.64 ± 1.95 vs 8.58 ± 1.97 days; p = 0.001). However, the intraoperative hemodynamic parameters and intensive care unit stay days were similar in both the groups. The perioperative data of the two procedures for renal hilar PGLs were compared. The Lap group showed estimated blood loss, and postoperative hospital stay outcomes were more favorable than the open group. Other data were similar in both the groups.
Conclusion:
Laparoscopic procedure is safe and feasible in the treatment of patients with retroperitoneal PGLs. Laparoscopic resection of PGLs from the renal hilum is technically challenging. However, it is possible to safely undertake laparoscopic resection of these tumors by an experienced surgeon.
Introduction
P
Currently, surgical resection remains the only curative treatment option for patients with PHEO/PGL. PHEO was initially considered a contraindication to the laparoscopic approach due to the concern of hypertensive crisis associated with the pneumoperitoneum. However, with careful preoperative medical treatment, appropriate patient selection, intensive anesthetic management, and less tumor manipulation, laparoscopic resection of PHEO has been shown to be safe and associated with lower morbidity and improved convalescence compared with open procedures. 3 –6
PGL resection is often challenging as these highly vascular tumors are mostly located near multiple vital blood vessels. Moreover, PGL is characterized by many small vessels leading to the lesion, unlike PHEO where a definite pedicle may be identified.
For these reasons, most PGLs are still operated by using an open approach. 7,8 Operative time for laparoscopic surgery in PGL patients, however, is reported to be significantly longer compared with PHEO, suggesting increased difficulty with laparoscopic surgery for PGLs. 9 To confirm the feasibility and safety of laparoscopic resection of PGL, we reviewed our experiences with laparoscopic resection of PGL and compared the surgical outcomes of laparoscopic procedures with conventional open surgical procedures.
Materials and Methods
Patients
From July 2005 to October 2014, 15 patients underwent laparoscopic tumorectomy for PGL and 12 patients underwent open resection for PGL from March 2002 to August 2014 in our department. All laparoscopic procedures were performed by a single surgeon (W.S.), whereas open operation was performed by several surgeons in the same department. A choice between laparoscopic and conventional open procedures was based primarily on the operating surgeon's preference.
Patients' charts were reviewed to collect demographic data, patient and tumor characteristics, operative data, pathologic features, and short- and long-term postoperative outcomes. The diagnosis of suspected PGL was based on clinical, biochemical, and radiographic data. Computed tomography (CT) or magnetic resonance imaging (MRI) and occasional metaiodobenzylguanidine (MIBG) scans were employed to localize the tumors. Biochemical detection included measurement of plasma catecholamine concentration and/or vanillylmandelic acid (VMA) in a 24-hour urine collection sample. A “Renal hilum tumor” was defined as the tumor located in the renal hilum that was shown, by preoperative imaging, to be in direct physical contact with the renal artery and/or vein.
In all patients, α-receptor blocker (phenoxybenzamine; 10–60 mg/day) was administered at least 1 week before surgery, followed by β-receptor blockers if the patient had a heart rate of more than 100 beats per minute (bpm). Calcium channel blockers were added for patients whose blood pressure was not well controlled by the α-receptor and β-receptor blockers. All patients were rehydrated with colloidal and crystalloid fluid for 3 days preoperatively. Operations were not undertaken unless patients had stable blood pressure readings of 140/90 mm Hg or below and a heart rate below 100 bpm for 3 days.
All patients were intubated under general anesthesia. Invasive arterial pressure monitoring was routinely performed through arterial catheterization. A central venous catheter was placed for continuous blood pressure monitoring. When needed, pharmacologic intervention, including antihypertensive drugs (phentolamine, sodium nitroprusside, etc.) to prevent intraoperative hypertensive crisis caused by the release of catecholamines, antihypotensive drugs (epinephrine, norepinephrine, etc.), as well as rapid infusion of crystalloid and colloid liquid to rescue serious hypotension just after resection tumor, was performed by skilled anesthesiologists. According to Varon, 10 systolic blood pressure (SBP) levels >180 mm Hg and/or diastolic blood pressure (DBP) levels >120 mm Hg were considered hypertensive crises and SBP <90 mm Hg and/or DBP <60 mm Hg were considered hypotensive crises. After surgery, patients were sent to a normal ward or the intensive care unit (ICU) depending on their patient's condition.
Complications were classified and recorded according to the Clavien classification methods. 11 A biochemical evaluation was performed with urinary catecholamine 1 month postoperatively, and the patients were followed up annually with urine catecholamine and appropriate imaging.
Surgical technique
The laparoscopic procedure was performed by a lateral decubitus transperitoneal approach. First, the 10-mm troca (camera port) was inserted by a Hasson technique above the level of the umbilicus and lateral to the rectus abdominis border. An additional 10-mm troca and two 5-mm trocas were placed in an arc-like manner on either side of the camera port. The pressure of CO2 pneumoperitoneum was maintained as 10 to 12 mm Hg during operation.
Patients with paracaval lesions were placed in the left lateral position. The right colon, duodenum, and right lobe of the liver were mobilized when needed. All tumors were excised with a margin of normal tissue where possible. The vessels entering the tumor need to be clipped and divided. Care was taken to avoid excessive manipulation of the tumor or penetration of the capsule. During resection of a PGL located in the right renal hilum (Fig. 1), the ureter and the vena genitalis were identified and not resected (Fig. 1B). Careful dissection was carried out to separate the tumor from its neighboring renal artery and vein (Fig. 1C, D). Subsequently, the inferior vena cava (IVC) was carefully mobilized clockwise to expose the tumor (Fig. 1E). Lumbar veins were divided when retrocaval access was required. The dissection was continued around the solid mass until all attachments and smaller blood vessels were taken down with either the blunt or ultrasonic dissection (Fig. 1F). The surgical specimen was placed into a retrieval bag and removed by enlarging the 10-mm port site used for access.
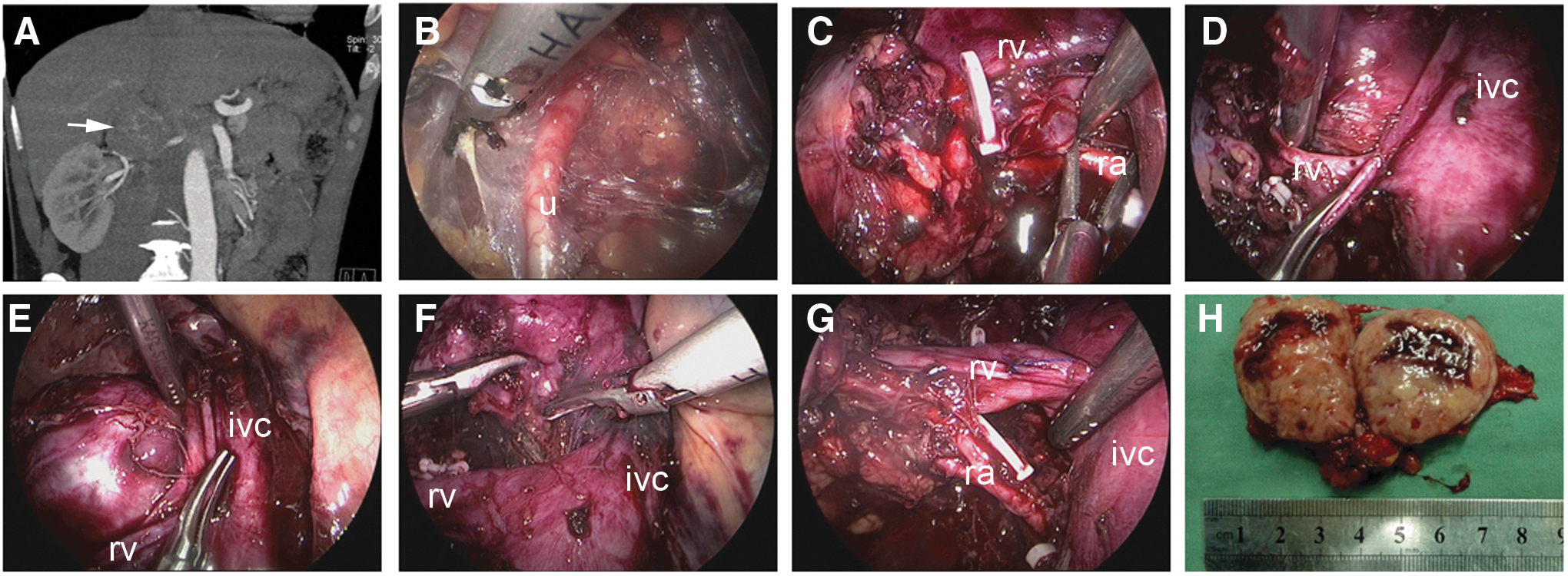
Laparoscopic resection of a paraganglioma (PGL) located in the right renal hilum.
Patients with para-aortic lesions were placed in the right lateral position. The spleen, the entire left colon, and the tail of the pancreas were mobilized using an ultrasonic dissection to expose the left kidney. The following dissection was similar to that described for paracaval lesions. Conventional open surgery was performed utilizing a subcostal or midline incision as the lesion's location dictated, and the patients were positioned supine with the flank slightly elevated.
Statistical methods
All data are presented as mean ± standard deviation. Statistical calculations were completed with SPSS version 14.0 software for Windows (Chicago, IL). Parametric data were compared using Student's t-test to determine the statistical significance, and the χ 2 test was used to compare nonparametric data. p-Value < 0.05 was considered as statistically significant.
Results
The patient characteristics are shown in Table 1. A total of 27 patients underwent resection of PGLs during the study period. These included 16 men and 11 women with a mean age of 45.1 and 49.5 years, respectively. Clinical symptoms included hypertension in 15 patients and abdominal pain in four cases. Ten cases were asymptomatic and were discovered as an incidental finding on imaging study.
Conversion from a laparoscopic to an open procedure.
HP = hypertension; IVC = inferior vena cava.
The majority of PGLs were adjacent to the renal hilum. Only one case occurred in the organ of Zuckerkandl. Of the 27 cases, 15 underwent laparoscopic procedures and 12 patients underwent conventional open procedures. Laparoscopic procedure was converted to open in one patient (Lap4) due to bleeding and massive adhesion. This patient underwent nephrectomy en bloc with the tumor. The case was excluded from the subsequent comparative analysis.
As per histopathologic examination, all the tumors were diagnosed as PGLs. In two patients (one case with conversion because of strong adhesions and another patient in the open group), the tumor presented with vascular and/or capsular invasion, which implicated malignant potential. However, there was no capsular rupture in patients with malignant potential.
Demographic and perioperative data on Lap and open groups are shown in Table 2. There was no significant difference in the set of age, gender, body mass index, or tumor size between the Lap and open groups. Operative time in the open group was significantly shorter than in the Lap group (175.67 ± 36.79 vs 217.36 ± 51.90; p = 0.029). Intraoperative blood loss was much higher with open procedures than than with laparoscopic procedures (172.50 ± 160.86 vs 80.71 ± 83.52; p = 0.047). Intraoperative hemodynamic parameters did not differ significantly between the two groups. Hypertensive crises (SBP >180 mm Hg and/or DBP >120 mm Hg) occurred with comparable proportion in the two groups (58.33% in open, 50.00% in Lap; p = 0.205). Hypotensive crises (SBP <90 mm Hg and/or DBP <60 mm Hg) also occurred with similar frequency in the two groups (16.67% in open, 21.43% in Lap; p = 0.268).
Student's t-test and χ 2 test.
BMI = body mass index; DBP = diastolic blood pressure; ICU = intensive care unit; SBP = systolic blood pressure.
Postoperative hospital stay in the open group was significantly longer than that in the Lap group (8.58 ± 1.97 vs 5.64 ± 1.95; p = 0.001). There was no difference in duration of ICU stay between the two groups (0.75 day in open, 0.93 day in Lap; p = 0.597) and no perioperative mortality rate in both groups. Complications occurred in one patient (7.14%) in the Lap group (grade 2a pneumonia effectively treated with antibiotics) and in two patients (16.67%) in the open group, which included a wound infection (grade 1), and an intestinal obstruction (grade 2a) that required gastrointestinal decompression.
Perioperative data on patients with renal hilar PGLs are shown in Table 3. Estimated blood loss was less for Lap vs open group (91.25 ± 107.36 vs 228.57 ± 193.25, respectively, p = 0.012); Postoperative hospital stay was significantly shorter in the Lap (5.88 ± 2.59) compared with the open group (9.14 ± 2.41; p = 0.008). Other perioperative data such as operative time, hypertensive crises, hypotensive crises, and ICU stay were similar in the two groups.
Student's t-test and χ 2 test.
In all the patients, blood pressure was well controlled without antihypertensive drugs after surgery. The mean (range) follow-up was 62.5 (4–152) months. One patient (open 2, Table 1) with a malignant PGL was detected to be hypertensive, with an elevated plasma catecholamine concentration and skeletal metastases, 39 months after open resection of tumor. However, none of the laparoscopic patients had clinical features or imaging evidence of recurrence. Nevertheless, in one patient with conversion (Lap4, Table 1), a paracaval recurrence (at the level of the second lumbar vertebrae) was determined on an imaging examination 18 months postoperatively, which was effectively managed by surgical resection and there was no further recurrence after the second operation.
Discussion
PGLs, the extra-adrenal counter parts of PHEOs, are rare tumors that, except for their location, have a clinical presentation similar to adrenal PHEOs. Functional PGLs can be diagnosed based on clinical presentation and laboratory examination showing elevated catecholamines and their metabolites (VMA) in the blood and urine. Nonfunctional PGLs are mostly found incidentally or through symptoms caused by compression of the surrounding organs. 12 Radiographically, PGL should be included in the differential diagnosis of any solid paravertebral or periaortic mass. With regard to sensitivity, CT and MRI have similar success in detecting PHEO/PGL. However, MRI may be preferred in patients with extra-adrenal tumors. 1 PGLs also may be imaged with functional imaging, such as PET scanning and 123I-MIBG, 13 which may help detect primary or metastatic tumors that could be missed on CT/MRI.
Laparoscopic adrenalectomy has become the preferred method for most adrenal tumors, including PHEOs. Traditionally, PGLs are resected by open surgery because of their close proximity to vital structures and high risk of malignancy (20%–30%). However, some surgeons have effectively applied laparoscopic techniques to PGLs resection. 9,14 –20 So far, the comparison analysis of the surgical results between open and laparoscopic procedures is still limited. Shen et al. 21 reported 102 patients undergoing adrenalectomy for PHEO at their institution. In that study,10 patients had PGLs (extra-adrenal PHEOs), 7 of whom underwent laparoscopic resection and 3 open but without more detailed outcomes details for the PGL patients were provided. Goers et al. 9 reported 15 cases of PGLs (9 laparoscopic, 6 open) and compared the outcomes with 62 cases of PHEOs that were resected laparoscopically; the conclusion told us that laparoscopic resection of PGLs seems to be the preferred surgical approach. Nevertheless, they did not discuss detailed benefit and shortage of laparoscopic procedure during resection of PGLs. Moreover, the study did not display the safety and feasibility of laparoscopic resection of PGLs from the renal hilum. Therefore, the major aim of this study was to report the results of our department with the context of open vs laparoscopic resection for the treatment of PGLs, particularly for tumor located in the renal hilum.
Our study showed that laparoscopic PGL excision could bring some advantages over conventional open resection, such as lesser blood loss and shorter postoperative ICU and hospital stay. In the laparoscopic procedure, the magnified laparoscopic view facilitates dealing with smaller blood vessels and fine dissection, less intraoperative hemorrhage, and a clearer operative field that minimizes direct manipulation of the tumor. PGLs are hypervascular tumors that release catecholamines when manipulated. This quality adds to the concerns for the safety of a laparoscopic approach to this disease. Laparoscopic adrenalectomy for PHEO has been shown to elevate the serum catecholamine concentration, however, to a lower concentration than seen with the conventional open procedure. 22 Although we have not included measurements of the serum catecholamine concentration, intraoperative hemodynamic parameters did not differ significantly between the two groups.
Renal hilar PGLs are in direct physical contact with important vascular structures and the viscera, which makes the resection more difficult and poses unique technical challenges. Hwang et al. 23 reported conversion to the open procedure because of technical difficulty during laparoscopic resection of renal hilar PGL. However, other authors have published much smaller case series or individual case reports on the treatment of these tumors, demonstrating the feasibility of laparoscopic resection. 14,24,25 In our series, laparoscopy was effective in eight of nine (88.9%) patients with renal hilar tumor. Conversion to open procedure was performed on one patient (Lap4) due to bleeding. The reports of laparoscopic resection of renal hilar PGL are few and, indeed, may be technically extremely difficult. From our clinical experience, we believed it is important that the dissection was maintained in a plane away from the tumor itself and to go along the surface of the renal vein, renal artery, and IVC or abdominal aorta. The vascular feeding branches were isolated and controlled with ultrasonic shears or Hem-O-lok, selected according to vessel size. Surgeons undertaking laparoscopic resection of renal hilar PGLs should be well versed at controlling bleeding if it occured. In our Lap8 patient, left renal vein impairment had more bleeding during dissection. We clamped the bleeding vessel with the left-hand instrument immediately, suctioned the field to obtain a clear view, and precisely sutured the bleeding vessel.
The main limitations of the present study were the small number of cases and the retrospective property. Considering the rare incidence of PGL, it is unlikely to develop prospective randomized trials. Also, the selection of the surgical procedure (open or laparoscopic surgery) was conducted according to the preference of the surgeon, and this would add selection bias. Nevertheless, we believe our results provide valuable insight into the value of the surgical outcome of retroperitoneal PGL.
In conclusion, our results demonstrate that laparoscopic PGL resection is safe, and offers equal chances of curing PGL, as the conventional open procedures for PGL, while offering numerous advantages such as less perioperative blood loss and shorter postoperative hospital stay. Laparoscopic resection of a renal hilar PGL is technically challenging. However, with careful medical preoperative preparation, intensive anesthetic management, and a meticulous surgical technique performed by an experienced surgeon, it is safe and feasible for laparoscopic resection.
Footnotes
Author Disclosure Statement
No competing financial interests exist.