
Abstract
Objective:
To evaluate the oncological and functional outcomes of primary cryotherapy in men with clinically localized, high-grade prostate cancer.
Subjects and Methods:
We included all men with biopsy Gleason score ≥8, localized (cT1-2) disease with a serum prostate-specific antigen (PSA) ≤50 ng/mL from the Cryo On-Line Data (COLD) registry. The primary outcome was biochemical progression free survival (BPFS) as defined by the Phoenix criteria (nadir PSA +2 ng/mL). Secondary outcomes of continence (defined as strictly no leak) and potency (able to have intercourse) were patient reported. Factors influencing BPFS were evaluated individually using Kaplan Meier and in a multivariate model using Cox regression.
Results:
Altogether, 300 men were included for analysis. The median follow-up was 18.2 months (mean 28.4) and median BPFS was 69.8 months. Based on Kaplan-Meier analysis, the estimated 2- and 5-year BPFS rate was 77.2% and 59.1%, respectively. Neoadjuvant hormonal therapy was administered to 41% of men and this tended to occur in men with larger prostates, likely as a technical consideration for downsizing before cryosurgery. At multivariate analysis, the presence of Gleason score 9 or 10 (Hazard Ratio [HR] 1.9) and a posttreatment PSA nadir of ≥0.4 ng/mL (HR 5.7) were the only significant variables associated with biochemical progression using Cox regression. Complete continence was noted in 90.5% of men and potency in 17% of men at the 12-month follow-up. The incidence of rectourethral fistulae and urinary retention requiring intervention beyond temporary catheterization was 1.3% and 3.3%, respectively.
Conclusion:
Primary cryotherapy appears to be effective and safe in the community setting for high-grade, clinically localized prostate cancer in the short term.
Introduction
P
The Cryo On-Line Data (COLD) registry, a platform for academic and community urologists to gather cumulative data to advance the awareness and science of prostate cryoablation through evidence-based medical outcomes, currently includes over 6000 patient records from 44 active sites. We report, in this article, early outcomes of men with high-grade (Gleason ≥8) and localized (cT1-2) prostate cancer undergoing primary whole-gland cryotherapy from the COLD registry.
Subjects and Methods
The COLD Registry is supervised by a scientific board of urologists, and an independent audit of the scientific data is conducted yearly at randomly chosen centers to ensure the accuracy of data. Although industry sponsored (HealthTronics, Austin, TX), all registry data collection was performed by an independent research company (Watermark Research Partners, Indianapolis, IN). All participating sites that were required to do so, had approval from their institutional review board (IRB) before submission of any data to the registry database. A global IRB protocol has been in place since 2006. 7,8
We queried the COLD registry for all patients with high-grade (Gleason ≥8), localized (cT1-2) prostate cancer undergoing primary whole-gland cryotherapy. Men with serum prostate-specific antigen (PSA) levels ≥50 ng/mL were presumed to have micrometastatic disease and were excluded from this analysis.
Biochemical progression-free survival, with progression defined by the Phoenix criteria (PSA nadir +2 ng/mL), is an accepted surrogate endpoint after whole-gland cryotherapy and this was used as our primary endpoint. 9 Nadir PSA was defined as the lowest PSA attained after treatment. Secondary outcomes included continence, erectile function, and complication rate. Incontinence was defined as any leak reported by the patient to the physician at the 12-month visit after primary whole-gland cryoablation. Pad-use information was also recorded. Potency was defined as the ability to have sexual intercourse with or without erectile aids, determined by the physician at the 12-month visit after primary whole-gland cryoablation. The data were independently entered and verified by Watermark Associates. Complication outcome measures analyzed were the incidence of retention and rectourethral fistula formation.
Statistical analysis was performed using Stata 13.1 (Statacorp, College Station, TX). Factors, including age, race, prostate volume, initial PSA, Gleason score, clinical stage, the use of hormonal therapy, nadir PSA, and the time to nadir PSA, were evaluated for impact upon biochemical progression-free survival in a univariate and multivariate fashion. Univariate analysis was performed using Kaplan-Meier analysis and Cox proportional hazard estimation. Multivariate analysis was performed using a Cox proportional hazard model, including all clinically and/or statistically significant univariate factors, achieving a model of best fit using backward elimination of insignificant variables. The model was then tested for assumptions of proportionality, with a final valid model being selected for clinical interpretation. Fine-Gray analysis was also performed to assess the impact of competing risks (death) on the hazard of developing biochemical progression.
Results
A total of 332 patients were identified from the registry and 300 with available follow-up data were included for analysis. The median follow-up time was 18.2 months (range 0.3–211 months) with a mean of 28.4 months. The median biochemical progression-free survival time was 69.8 months (95% CI 60.1–102.2).
The demographics of the cohort are reported in Table 1. In brief, the mean age of the cohort at diagnosis was 73.2 years and median PSA was 6.85 ng/mL. All the tumors were otherwise clinically localized with a Gleason score ≥8 as per our selection criteria. Of the cohort, 122 patients (40.7%) received neoadjuvant hormonal therapy. The data on duration of neoadjuvant hormonal therapy were only available for 66 patients, which was a median of 4 months (mean 5.9 months, range 1–48 months). An additional 47 (15.7%) patients received adjuvant hormonal therapy after treatment for an unrecorded duration. The specific formulation of hormonal therapy used was unavailable.
Data from only 259 men available for analysis.
PSA = prostate-specific antigen.
The mean PSA nadir reached after treatment was 0.40 ± 1.14 ng/mL, with a median time to nadir of 3.1 months (range 0.3–99.1). Of the cohort, 42% (n = 126) of patients reached a nadir that was undetectable (less than 0.02). The use of neoadjuvant hormonal therapy was associated with improved odds of achieving an undetectable nadir PSA (OR 1.7, 95% CI 1.09–2.81).
The 2- and 5-year biochemical progression-free survival rates based on Kaplan-Meier analysis were 77.2% (95% CI 70.9%–88.3%) and 59.1% (95% CI 50.2%–66.9%), respectively. At univariate analysis, an initial PSA of >5 ng/mL was found to be significantly hazardous to biochemical progression-free survival at HR 1.9 (Fig. 1). A Gleason score of 9 or 10 also conferred an additional risk compared to a score of 8 (HR 1.7) (Fig. 2). Posttreatment PSA nadir was an important predictor of biochemical progression-free survival: every 0.1 ng/mL increase in the PSA nadir conferred an additional 4.5% risk of hazard (HR 1.04, 95% CI 1.03–1.06). A dichotomization at PSA nadir 0.4 ng/mL was used for further analysis, based on best fit in the final multivariate model. Men with a PSA nadir ≥0.4 ng/mL predicted poorer biochemical progression-free survival compared to those with a PSA nadir of <0.4 ng/mL (HR 5.5) (Fig. 3). Age, prostate volume (only 259 data available for analysis), clinical stage, neoadjuvant hormonal therapy use, duration of neoadjuvant therapy and adjuvant hormonal therapy use were not significant in influencing biochemical progression-free survival at univariate analysis.
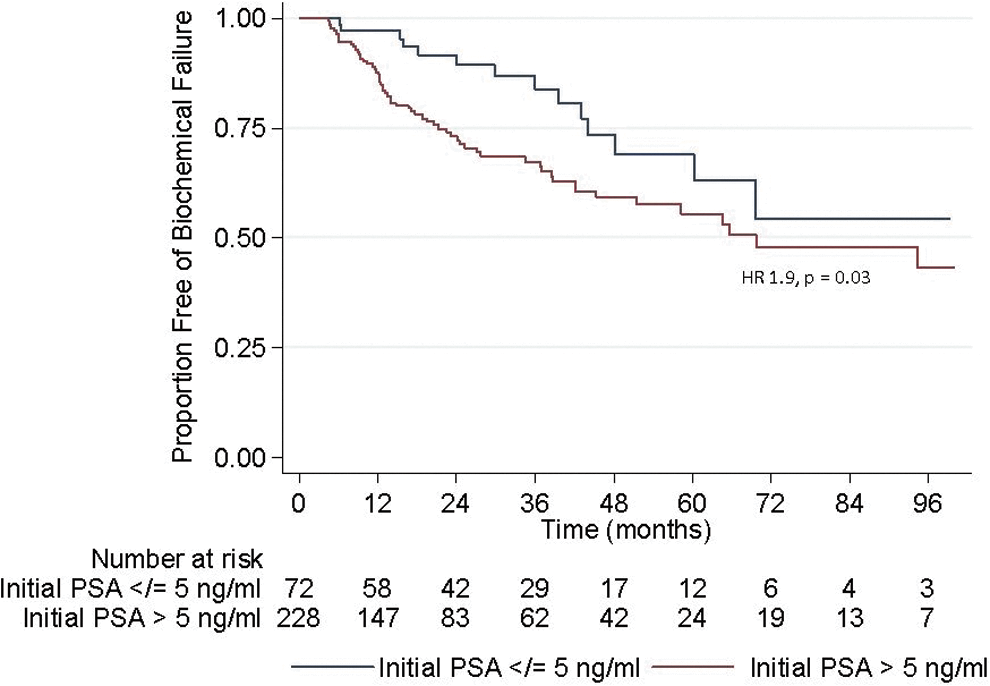
Biochemical progression-free survival (BPFS) stratified by initial PSA: HRs for initial PSA >5 compared to baseline (PSA ≤5). 95% CI, 95% confidence interval; HR, hazard ratio; PSA, prostate-specific antigen. Color image available online at

BPFS stratified by Gleason score: HR of having Gleason score 9 or 10 to Gleason score 8. Color image available online at
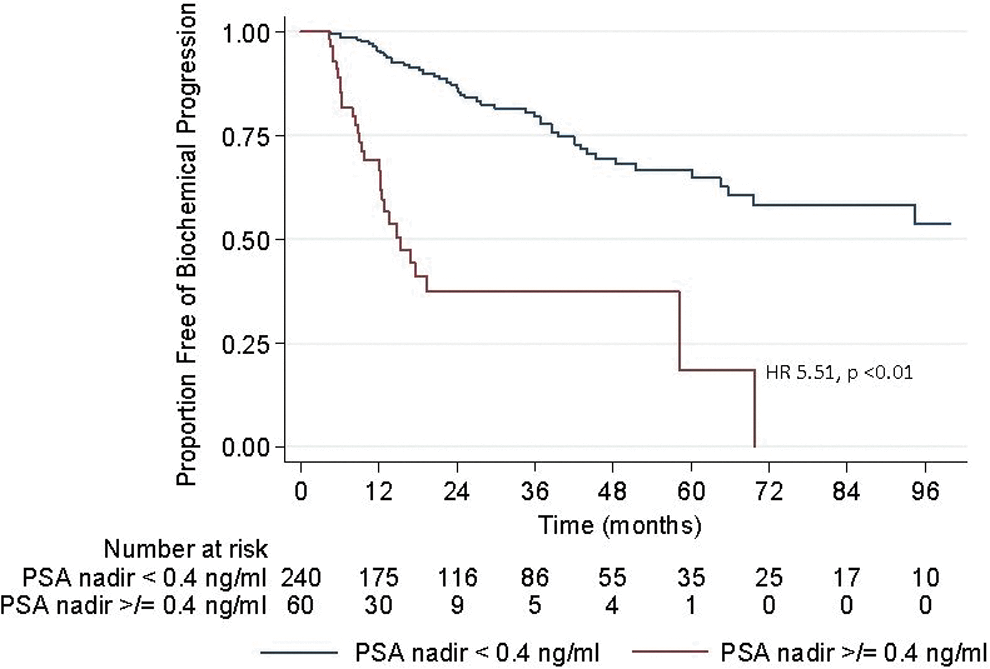
BPFS stratified by posttreatment PSA nadir: HR reported for PSA nadir ≥0.4 is compared to baseline (PSA nadir <0.4). Color image available online at
At multivariate analysis, the significant factors in the final Cox model were the Gleason score and posttreatment PSA nadir (Table 2). Variables found to be of threshold significance for testing at univariate analysis such as initial PSA and the use of neoadjuvant or adjuvant hormonal therapy were not significant in influencing biochemical progression at multivariate analysis.
Multivariate analysis using Cox regression: insignificant variables removed from final Cox model not shown here (initial PSA value, use of neoadjuvant hormonal therapy, and use of adjuvant hormonal therapy).
95% CI = 95% confidence interval; HR = hazard ratio; p = probability due to chance.
The 12-month patient-reported continence rate in our series was 90.5% of 285 men with available continence data. Of the 27 men (9.5%) who had incontinence at 12 months, 15 reported having a small leakage not requiring pads, 9 reported the use of 1–2 pads per day, and 1 man used 3–4 pads per day. The details of two men were not accounted for. The potency rate at 12 months was 16.5% (n = 36 men) of 218 men with available data. Of these ∼28% (8 men) were able to have intercourse without the use of medications or adjunct devices.
Urinary retention occurred in 9.7% of men (n = 29) within 12 months of treatment. Of these men, the majority resolved after a short duration of urethral catheterization. Four men required prolonged, clean intermittent self-catheterization, five men required other outpatient manipulation, and one man underwent formal transurethral resection of the prostate. The rate of rectourethral fistula formation was 1.3% (n = 4).
Discussion
Occult metastatic disease is more often present in men with high-grade tumors than in men with low-grade cancer. However, the experience with radiation and surgery suggests that a significant proportion of men with high-grade disease can achieve long-term disease-free survival with local therapy alone. Irrespective of treatment modality, it is logical that oncological control depends on complete eradication of prostate cancer cells. To assess the oncological efficacy, we used the Phoenix definition (nadir PSA +2 ng/mL), an accepted outcome measure after whole-gland cryotherapy, for biochemical progression. 9 In this series, the 2- and 5-year biochemical progression-free survival (BPFS) rates were 77% and 59%, respectively. Cryotherapy induces local tumor ablation through multiple pathways, including mechanical cell destruction by the formation of ice crystals, tissue necrosis, and the induction of apoptosis through metabolic, vascular, and immune pathways. 10 We found PSA nadir to be the most important factor predicting biochemical progression in our cohort, with a lower PSA nadir correlated with less risk of biochemical progression. A PSA nadir threshold of 0.4 ng/mL for predicting time to biochemical progression was highly significant statistically (p < 0.01), with a clinically significant effect size (HR 5.7), and this builds upon earlier findings from an overall analysis of the COLD registry series. 11
The impact of PSA nadir on biochemical progression is similar to findings in radiation studies. 12 The PSA nadir persists in significance at a longer follow-up and emphasizes the importance of complete cell-kill, particularly in this high-grade, clinically localized setting. The techniques for achieving this are well-described such as the use of appropriate cryotherapy probe positions and two successive freeze-thaw cycles. 13 In contrast, another COLD registry report on outcomes in cT3 disease only described poorer BPFS, likely representing the effects of incomplete cancer ablation or an established disease already well beyond the confines of the gland. 14
Cryotherapy is similar to radiation therapy in that both are nonextirpative in nature and, while direct comparison is not possible, it would be informative to briefly review here the results of radiation therapy in the high-risk setting. The two radiation trials with the highest proportion of high-risk patients were the Dutch trial (54%) and the Medical Research Council (MRC) RT01 trial (43%). The Dutch trial, using American Society for Radiation Oncology (ASTRO) criteria, reported a 5-year freedom from failure rates of 52%. 15 The MRC RT01 reported a 5-year BPFS of 61% to 70% using a definition similar to the Phoenix criteria. 16 In both trials, neoadjuvant hormonal therapy was administered to all men, with the Dutch trial further randomizing men to short course (3–6 months) vs long course (3 years). In contrast, in the present series, only 40.7% of men received neoadjuvant hormonal therapy with 45.3% of men receiving any form of peritreatment hormonal therapy, and this may partly explain the slightly lower biochemical progression-free rate. Neoadjuvant hormonal therapy is characteristically utilized in men with large prostates before cryotherapy to reduce prostate size that facilitates sufficient overlapping ice coverage of the prostate, thereby decreasing the likeliness of incomplete ablation. While the use of neoadjuvant hormonal therapy was 1.7 times more likely to achieve an undetectable nadir PSA, we were unable to find any association of the use of perioperative hormonal therapy with biochemical progression at multivariate modeling. This may be due to the present study being underpowered to detect the effect or insufficient granularity in the hormonal therapy data pertaining to duration of use.
As the reference treatment, it would also be pertinent to briefly discuss the outcomes of prostatectomy in this arena, although direct comparison is not at all possible due to different cohort compositions with prostatectomy cohorts typically, including significant proportions of T3 disease, definitive local staging with prostatectomy, and different definitions of recurrence. 9,17 In a high-risk radical prostatectomy, cohorts consisting of 84% to 90% clinically localized disease, Bastian et al. reported a 5- and 10-year BPFS of 40% and 27% (Johns Hopkins cohort, n = 220) and a 5- and 10-year BPFS of 32% and 28% (the Shared Equal Access Regional Cancer Hospital [SEARCH] database, n = 149). 18 Donohue et al. reporting on 238 men with high-risk cancer from the Memorial Sloan Kettering Cancer Center (MSKCC) prostatectomy cohort, in whom 89% were clinically localized, found a 5-year BPFS of 51% and 10-year BPFS of 39%. 19 Walz et al. reported a 5-year BPFS of 35.4% for men with Gleason score ≥8, 80% being clinically localized. 20
In terms of safety, cryotherapy for high-grade prostate cancer had acceptable rates of side effects and complications in our series of registry patients. The continence rate was 90% at 12 months, comparable to that of prostatectomy and radiation. 21,22 Moreover, our criterion for continence is strictly no leak, whereas most series report social continence. Only 3.3% of men in our cohort were using 1 or more pads per day at 12 months. While the reported rate of stricture requiring intervention ranges from 0.9% to 2.2% after prostatectomy and up to 7.2% after radiation, only 2.6% of men in our series required procedures for retention. 22,23 The most serious complication, rectourethral fistula, occurred in 1.3%. Our overall 12-month potency rate was 16.5%, attributed, in part, to nearly half the men in the cohort receiving perioperative hormonal therapy. The rates of these side effects/complications appear favorable, especially considering that men with high-grade disease typically have a nonnerve-sparing prostatectomy or high doses of radiation plus androgen deprivation. 24
While informative, there are several limitations with which this study must be interpreted. First, our series has significant loss to follow up, resulting in the relatively short median follow-up duration of 18.2 (mean 28.4) months. The risk of noninformative censoring is thus high. However, we felt it important to include all information as is, rather than limit analysis to those with s follow-up of more than 12 to 24 months, to provide a representative analysis of the cohort. A sensitivity analysis, limiting analysis to greater than 3 or 6 months of follow-up, was performed (Supplementary Annex A; Supplementary Data are available online at
Second, the COLD registry is a database contributed to largely by community urologists. While the advantage of this is the real-life picture of how contemporary cryotherapy is conducted, for scientific purposes, the lack of a formal protocol may result in significant heterogeneity. For instance, while it is known who received neoadjuvant or adjuvant hormonal therapy, there is no indication of why these were administered, the type of hormonal therapy used, or a standard duration of use. We did not find a significant difference in recurrence rates between those who received hormonal therapy and those who did not. The data suggest that neoadjuvant hormonal therapy tended to be given to men with larger prostates (mean 42 mL ±18 vs 31 mL ±10), consistent with the practice of hormonal downsizing for large glands. Another deficiency in standardization is with regard to the type of imaging used for local staging and metastatic workup. This information was not available in the registry.
Third, the registry captures overall trends, and certain details of interest were not available for analysis. It would have been useful to have the initial biopsy information and tumor location available for analysis in relation to outcomes. Fourth, while biochemical progression is known to precede metastasis followed by death both in men treated with prostatectomy and radiation, we did not have a sufficiently long follow-up to analyze these outcomes meaningfully. 25,26 In the series, 10 men died, 3 sometime after biochemical progression and 7 men without biochemical progression (median 16.9 months, range 10.0–134.0). The causes of death were not known, but competing risk analysis did not value-add to the Cox model findings. Finally, we did not have sufficient, completed standardized questionnaires that led to our functional outcomes being patient-reported and physician-recorded, and this may limit their interpretation.
This report offers important information regarding early outcomes in the largest series of men undergoing whole-gland cryotherapy for high-grade, clinically localized prostate cancer. We feel that future prospective investigation should involve standardized protocols, the comparison of whole-gland cryotherapy to other treatment modalities, and the use of imaging for treatment planning.
Conclusion
Cryotherapy is a viable choice for patients with high-grade, localized prostate cancer with acceptable short-term oncological and functional outcomes. In our cohort, completeness of prostate cancer ablation, as determined by postprocedure PSA nadir, appears to be the most important factor in determining BPFS.
Footnotes
Author Disclosure Statement
Drs. K.J.T., A.E., and M.L.C. have nothing to declare. Drs. T.J.P., R.W.G., V.M., A.E.R., and J.S.J. have served on the COLD registry advisory board in this past year. Dr. T.J.P. s. Dr. J.S.J. has consulted for Cook and Healthtronics.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.