
Abstract
Objective:
For minimal invasive treatment of small renal masses, cryoablation has gained popularity. Treatment success is defined as the absence of contrast enhancement on postoperative imaging of the cryoablated lesion, but contrast enhancement does not necessarily equal treatment failure. This present study investigates the proportion of spontaneous resolutions after initial contrast enhancement in relation to cryoablation.
Materials and Methods:
Data were collected from a prospectively maintained clinical database containing all patients treated with primary laparoscopic and percutaneous cryoablation between August 2005 and December 2013. All images were evaluated with regard to preoperative aspects and dimensions used for an anatomical classification (PADUA) score, cryolesion size, contrast enhancement pattern, and tissue density.
Results:
A total of 107 patients with a biopsy-verified malignant tumor were included in the study. On postoperative imaging, 33 (31%) patients presented with contrast enhancement. Spontaneous resolution was observed in 15 (45%) patients after a mean follow-up time of 14 months. Patients with cryolesions that resolved spontaneously were found to have a less anatomical complex tumor compared to patients with treatment failure (PADUA 7.8 vs 9.5, p < 0.01). A total of seven patients with a PADUA score ≥10 and contrast-enhancing cryolesions were found to have treatment failure. No association was found among body mass index, histology, treatment modality, enhancement pattern, number of applied cryoprobes, and resolution.
Conclusion:
Postoperative contrast enhancement is commonly observed after cryoablation and a large portion of these lesions often resolves spontaneously, thus not representing treatment failure. In patients with a high preoperative PADUA score and postoperative contrast enhancement of the cryolesion, treatment failure or recurrent disease should be suspected.
Introduction
M
Partial nephrectomy is the gold standard for treating most small renal masses (SRMs), due to a comparable oncologic outcome, improved preservation of renal function, and improved overall survival. 6 However, additional minimal invasive techniques, including both laparoscopic cryoablation (LCA) and percutaneous cryoablation (PCA), offer patients additional options and are increasingly being used for treating with SRMs. 7 In contrast to partial nephrectomy, cryoablation leaves no specimen for confirmation of surgical margins, which makes the modality strongly dependent on postoperative imaging. Findings indicative of residual or recurrent tumor include new rim enhancement, internal enhancement, and increased size of the cryolesion. 8 –10
Even though postoperative contrast enhancement of the cryoablated lesion can be a disturbing discovery, it does not necessarily equal treatment failure as cancer cells have been found in <40% of these cases. 11,12 Furthermore, up to 57% of the cryoablated lesions have been shown to present contrast enhancement on the initial postoperative control computed tomography (CT) that will resolve spontaneously on the following control CT. These lesions were, therefore, falsely diagnosed as treatment failures due to the initial postoperative contrast enhancement. 13
The present study describes the technical, radiologic, and pathologic outcome of the first 107 consecutive patients with a biopsy-verified malignant pT1a tumor. The primary outcome is the proportion of patients with spontaneous resolutions after initial contrast enhancement in relation to cryoablation.
Materials and Methods
Patient identification
With approval from the Danish National Health and Medicines Authority, a review of a prospectively maintained clinical database was performed to identify patients treated with primary LCA and PCA between August 2005 and December 2013. A total of 121 patients with a biopsy-verified T1a malignant renal lesion were identified. Patients with multiple tumors treated in a single session (eight patients) and those patients who had magnetic resonance imaging (MRI) follow-up (six patients) were excluded from the study. Of the remaining 107 patients, evidence of contrast enhancement was found on the initial postoperative CT in 33 (31%) patients.
Cryoablation techniques
At our institution, all patients with a pT1a tumor are offered cryoablation as primary treatment, thus not limited to patients with low performance status or a high surgical risk. The decision of LCA or PCA was based on tumor location and proximity to thermosensitive structures such as intestine, pancreas, and the pleura sinus. The anatomical complexity of each renal mass was determined using tumor size, location, and closeness of the renal mass to the urinary collecting system. These parameters and their categorized equivalents according to the preoperative aspects and dimensions used for anatomical (PADUA) classification of renal tumors were examined. Initially, biopsies were performed intraoperatively before freezing was commenced. In August 2011, the biopsy protocol was changed to avoid unnecessary treatment of benign tumors, thus, all patients underwent an ultrasound-guided percutaneous biopsy as part of the diagnostic evaluation process before treatment.
The LCA procedure consisted of a standard three-port transperitoneal approach. Endoscopic ultrasound (Analogic BK 4-Way Laparoscopic 8666-RF) was used for tumor identification, biopsy guidance, probe placement, and monitoring of the freezing process. Tumors were treated with a double freeze–thaw cycle of 10-minute freeze, 8-minute thaw, and 10-minute freeze. A core temperature of at least minus 40°C was reached in each freeze cycle, aiming at a 5 mm margin to the tumor when anatomically possible.
A highly experienced interventional radiologist performed all the PCA procedures using ultrasound for probe placement and monitoring of the freezing process. Both procedures were performed under general anesthesia. An argon-/helium-based cryosystem (SeedNet and later Visual Ice, Galil Medical) with 17-gauge (1.47 mm) argon cryoprobes and thermo sensors was used for both modalities.
Postoperative follow-up
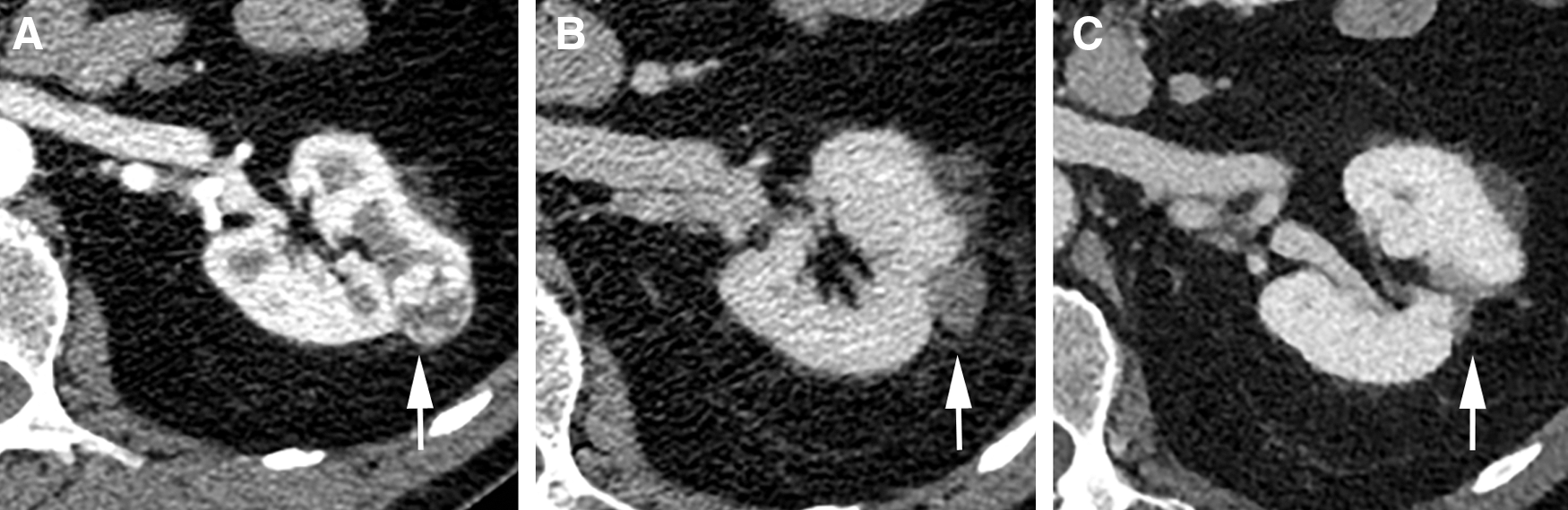
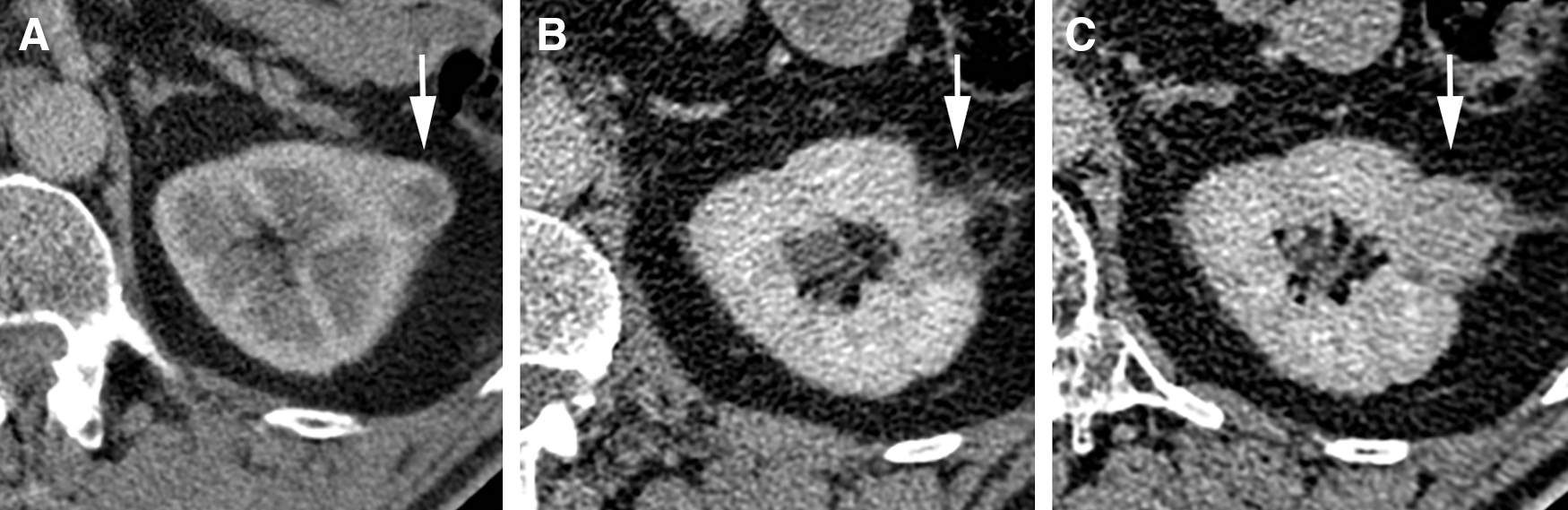
Postoperative follow-up imaging was conducted using contrast-enhanced CT (Philips Brilliance CT 64-slice /Siemens Somatom Definition AS CT 64-slice /Toshiba Aquilion One CT 256-slice). A postoperative CT, including noncontrast and postcontrast images (4 mL/second, Omnipaque 300 mg I/mL, Iohexol; GE Healthcare), in the late arterial and excretory phase was performed at an intended interval of 6 months for the first 2 years and then annually up to 5 years. The contrast volume was adjusted according to patient weight; 50–59 kg = 95 mL/60–69 kg = 110 mL/70–79 kg = 130 mL/80–89 kg = 145 mL/>90 kg = 155 mL. Senior specialists in radiology evaluated all images with regard to cryolesions size, shape, and contrast enhancement level and pattern. One experienced uroradiologist (>15 years experience, G.A.) had the overall responsibility for the evaluation of cryolesions. Size was measured as the largest diameter. Pathologic contrast enhancement of the cryolesion was defined as an attenuation level ≥25 Hounsfield units (HU), with the morphology being characterized as diffused, focal, or rim enhancement. Each cryolesion was characterized as resolved (no significant enhancement with obvious shrinkage of the ablation zone, Fig. 1), observation (stable or decreasing HU level with doubtful shrinkage of the ablation zone, Fig. 2), or failure (increasing contrast enhancement, area of peripheral irregular nodular enhancement within the ablation zone, or an increase in the size of the cryolesion, Figs. 3 and 4).

Normal course.
Spontaneous resolution.
Incomplete ablation.
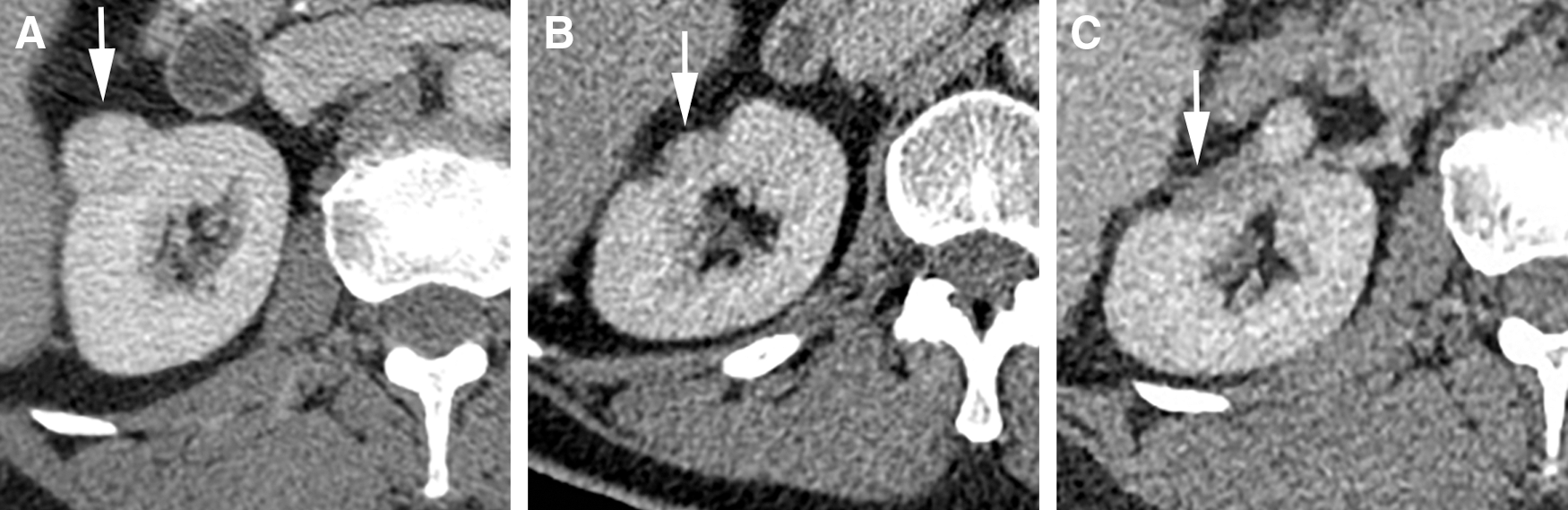
Recurrent disease.
Statistical analysis
Frequency tables were calculated for demographics, tumor, and treatment characteristics. Data are reported as the mean with 95% confidence interval (CI) or number (%). For comparison, Fischer's exact test was used. p-Values <0.05 (two-tailed) were considered significant. Data were analyzed using STATA 13 (StataCorp LP).
Results
A total of 107 patients with a biopsy-verified single malignant tumor were treated with either LCA or PCA procedures at our institution between August 2005 and December 2013. On postoperative imaging, a total of 33 patients (mean age = 64 years; mean body mass index [BMI] = 27 kg/m2; mean American Society of Anesthesiologists [ASA] class = 2; mean tumor size = 26 mm) displayed contrast enhancement. The number of patients with contrast enhancement on postoperative imaging was evenly distributed through the observation period. The remaining 74 patients with no sign of contrast enhancement were followed for a mean time of 37.2 (95% CI: 34.3–40.1) months without radiologic indication of treatment failure. Demographic baseline data are summarized in Table 1 and a patient flow chart is presented in Figure 5.
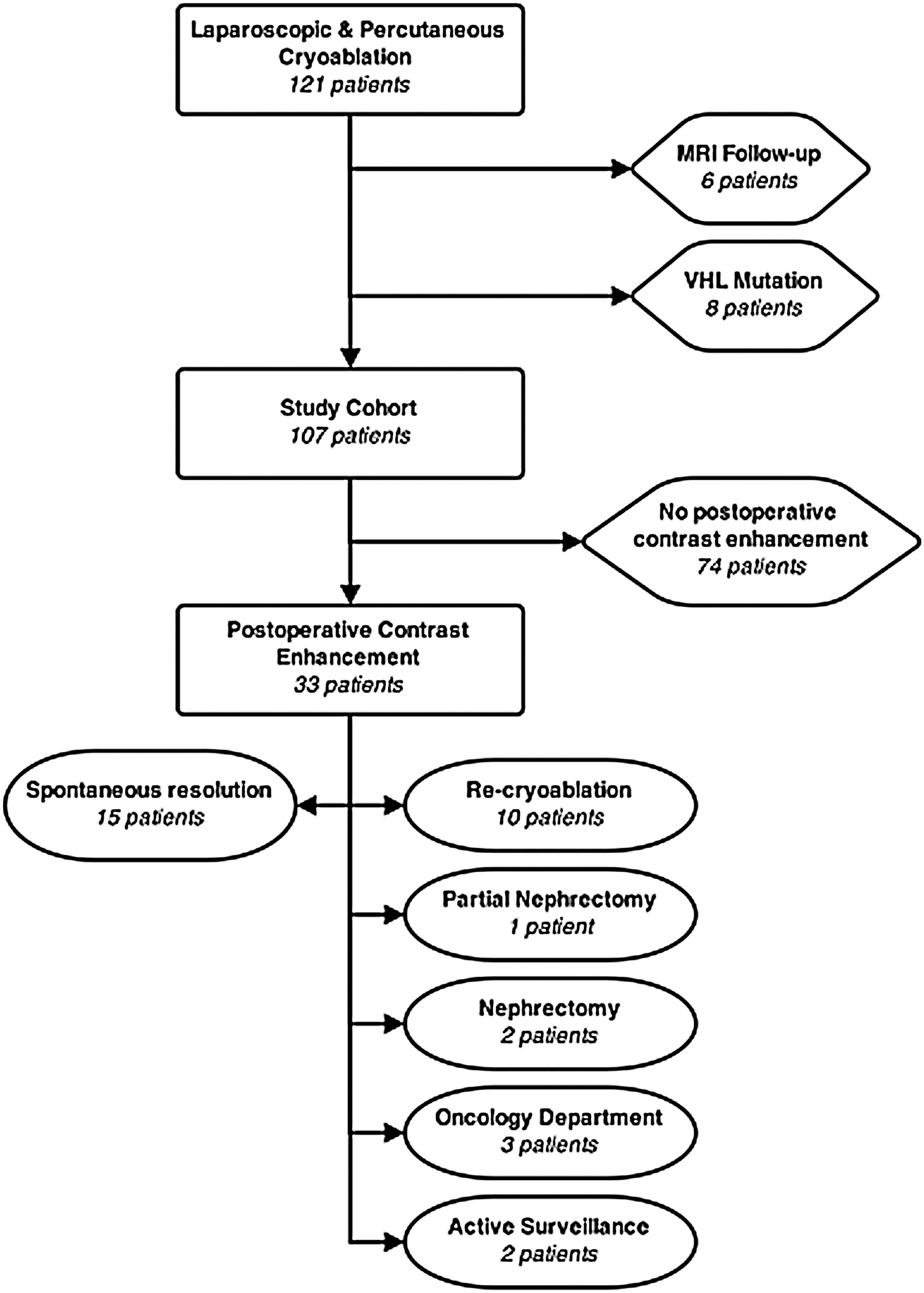
A flow chart showing the number of patients with spontaneous contrast resolution and the course of treatment for patients with salvage procedures.
ASA = American Society of Anesthesiologists; BMI = body mass index; CI = confidence interval; ECOG = Eastern Cooperative Oncology Group; PADUA = preoperative aspects and dimensions used for anatomical classification.
Spontaneous resolution of contrast-enhancing cryolesions was observed in 15 of the 33 patients (45%) after a mean time interval of 14 (95% CI: 10.7–40.1) months postoperatively. The mean follow-up time for patients in whom spontaneous resolution occurred was 49.1 (95% CI: 42.1–56.1) months. Patient age, tumor size, ASA class, and Eastern Cooperative Oncology Group performance status were all found to be significantly lower among patients experiencing spontaneous resolution compared to patients with treatment failure. No significant difference was found in either size reduction or the contrast enhancement pattern.
Patients with contrast-enhancing cryolesions that resolved spontaneously were found to have less anatomically complex tumors compared to patients with treatment failure (PADUA 7.8 vs 9.5, p < 0.01). When stratifying the PADUA classification in three groups (low, intermediate, high), we found that none of the patients (n = 7) with a high PADUA score resulted in spontaneous resolution. The mean change in cryolesion size was found to be −3.4 mm in the spontaneous resolution group compared to +2.3 mm in the treatment failure group (p < 0.01).
Patients with contrast-enhancing cryolesions that resolved spontaneously were found to have lower mean attenuation levels (HU: 27 vs 51, p < 0.01) compared to patients with treatment failure. BMI, tumor histology, contrast enhancement pattern, and number of cryoprobes used for treatment did not prove to be significantly different between the two groups. A comparison of patient, tumor, and treatment characteristics in cryolesions with spontaneous resolution vs treatment failure is provided in Table 2. When stratifying on the attenuation level at the 50% percentile(39 HU), it was found that only 13% experienced spontaneous resolution if the attenuation level of the cryolesion exceeded 39 HU compared to 39% with lower attenuation levels (p = 0.004).
HU = Hounsfield units.
A total of 10 patients (29%) underwent recryoablation of the enhancing cryolesion after a mean time of 13.5 (95% CI: 8.0–18.9) months following initial cryoablation. Biopsies were obtained in relation to the reablation procedure, and RCC was confirmed in 9/10 patients. The biopsy from the last patient was unsuited for analysis. Additional salvage procedures consisted of one partial nephrectomy and two nephrectomies, histology confirming RCC in all three cases. A total of three patients were referred to oncologic treatment after LCA treatment. Two of these patients had a nephrectomy several years before cryoablation due to clear-cell carcinoma and were later found to have metastasis to the pancreas and incomplete ablation (too fragile for anymore surgery), respectively. The last patient referred to oncologic treatment was found to have incomplete ablation, but was too fragile for any surgery.
Two patients are still unresolved and considered as active surveillance patients. The first patient continues to have high HU values (50–60 HU) in the cryolesion, but with limited discrepancy between noncontrast and postcontrast images. Furthermore, the cryolesion remains unchanged in size. The second patient developed focal enhancement (30–40 HU) in relation to the cryolesion and was biopsied with a negative result. Both patients are followed closely and await the next CT.
Discussion
Our findings confirm that initial contrast enhancement after cryoablation of SRMs is a common finding. A large percentage of these enhancing cryolesions are likely to resolve spontaneously without need of retreatment. Our results also indicate that for those enhancing cryolesions with an initial PADUA score ≥10, residual unablated tumor or recurrent disease should be considered.
Findings indicative of residual or recurrent disease include new nodal or rim enhancement, internal enhancement, and increase in size of the cryolesion. 9 Stein et al. described a series of 32 cases (72% biopsy proven RCC), in which five cases (16%) displayed contrast enhancement at 3 months, three of which persisted at 6 months. One case continued to display enhancement at 9 months, at which point a partial nephrectomy was performed. The following pathology examination demonstrated no recurrent cancer. 11 Beemster and colleagues studied the phenomenon of rim enhancement within a series of 25 cryolesions (44% biopsy proven RCC) and found that 20% of lesions displayed contrast enhancement after 3 months. The enhancement was found to disappear spontaneously up to 6 months after ablation. 14 Another study, although MRI-based, found that 39% had initial enhancement and that spontaneous resolution occurred within 3–14 months. 15 A recent study by Tsivian et al. analyzed 172 procedures (no histology information provided) and found that 17% had contrast enhancement on follow-up CT. Spontaneous resolution was noted in 57% of the cases with no association between the enhancement pattern and resolution. 13 Our findings support the claim that contrast enhancement is a common observation after cryoablation and was experienced in 31% of the cases in this study. The process of evaluating cryolesions is a challenging task and it requires extensive experience to distinguish a residual unablated tumor from an effective ablation. Observation of postoperative rim enhancement is often not a sign of residual unablated tumor or recurrent disease, but a common finding that should be followed and is not necessarily a cause for concern. HU-levels from 15 to 20 have been suggested, but none has gained broad acceptance. 16 In this study, enhancement ≥25 HU was applied to define significant contrast enhancement. Interpreting differences in the reported outcomes across studies require careful consideration of confounding variables that might account for the differences, making comparisons complex.
Effectively treated cryolesions are expected to decrease in size over time due to cellular breakdown and phagocytosis. 17 In this study, we found that enhancing cryolesions that resulted in spontaneous resolution showed an average decrease in diameter of 3.4 mm, whereas cryolesions requiring reablation in average increased by 2.3 mm. Other groups have reported on the general development of cryolesion size and also found a mean reduction in cryolesion size during follow-up. 14,18 Our findings support this claim, but we did see examples of residual unablated tumors that exhibited a decrease in size.
Classification systems, such as the PADUA classification and radius, exophytic/endophytic, nearness, anterior/posterior, and location (RENAL) nephrometry indices, were originally designed to aid the selection process of renal tumors suitable for nephron-sparing surgery based on anatomical complexity. 19 –21 A recent study by Lagerveld et al. concluded that the RENAL score and not the PADUA score was associated with a higher risk of intraoperative complications in relation to LCA. 22 Schmit and colleagues reviewed 751 renal tumors treated percutaneously with either cryoablation (57%) or radio frequency ablation (43%) and found that the RENAL score could predict treatment complications as well as treatment efficacy following ablation. 23 In this present study, we found a significant increase in anatomical tumor complexity quantitated by the PADUA score in cryolesions with contrast enhancement that did not resolve spontaneously. When considering only the most complex tumors with a high PADUA score (≥10), it was found that none of these cryolesions resulted in spontaneous resolution. A plausible explanation for this could be that probe placement is likely to be more challenging in tumors with a complex anatomical location, thus increasing the risk of incomplete ablation. Furthermore, a centrally located tumor resulting in a higher classification score will often be more exposed to warm blood flow, giving thermal protection to cells in the vicinity of the cryolesion (the heat pump effect).
Throughout the last decade, minimal invasive laparoscopic and percutaneous ablation techniques have emerged as alternatives to surgical resection of T1a renal tumors, with cryoablation being among the most extensively investigated approaches. Following cryoablation, a contrasted image is always obtained to assess the adequacy of treatment. An effective outcome is commonly based on the absence of contrast enhancement on postoperative cross-sectional imaging of the cryolesion and an absence of tumor growth and subsequent contraction of the cryolesion. 15,24 While absence of contrast enhancement is indicative of a favorable outcome, residual enhancement (particularly peripheral rim enhancement) is a common finding and does not necessarily represent treatment failure. These residual enhancements can persist for months. 14,15,17 A few studies have used postoperative biopsies to determine treatment success, but these remain controversial and no study in particular has targeted contrast-enhancing lesions, thus limiting the knowledge about causes and impact hereof. 12,25,26 Traditionally, renal biopsies have played a limited role in the management of SRMs—thus, many publications on renal cryoablation cannot account for the malignant nature of the material. Numerous studies have shown renal biopsy to be a safe procedure and both the American Urological Association and European Association of Urology now endorse biopsy before ablation therapy. 10,27,28
In this current study, spontaneous resolution was observed in 45% of the patients with enhancing cryolesions. Median time to spontaneous resolution was 12 months (3–45). One patient, in whom spontaneous resolution was observed as late as 45 months after treatment, is likely to be an outlier. Due to nonappearance of the patient, a CT was not performed between 22 and 45 months and data were kept in the analysis for completeness. Otherwise, the maximum observed time to spontaneous resolution was 36 months. We found that a diffuse enhancement pattern was predominant in both the first and the second follow-up CT. No distinct enhancement pattern was observed in either the third or fourth follow-up CT. In line with the study by Tsivian et al., we did not find any association between the enhancement pattern of the cryolesion and the final outcome (spontaneous resolution vs treatment failure). 13
Of the 33 cases with postoperative contrast enhancement, we found that only 13% experienced spontaneous resolution if attenuation levels increased to more than 39 HU. This finding is in accordance with the results found by Tsivian et al., who reported that only one of seven lesions (14%) enhancing >35 HU experienced spontaneous resolution. 13 In general, the phenomenon of postoperative contrast enhancement within cryolesions is not fully understood and needs further investigation. Zhu et al. studied the phenomenon on MRI in a rabbit model and found abnormal tubules, congestive vessels, vascular granulation tissue, inflammation, and dilatation of small vessels. 29 Similar changes could also be present and, thereby, contribute to contrast enhancement in patients. The question still unanswered is, why do only some and not all cryolesions display contrast enhancement on initial postoperative imaging? One could speculate that tumor heterogeneity (i.e., cellular morphology, gene expression, metabolism) plays a role in how cryolesions behave in regard to postoperative imaging. 30
Based on our results, early aggressive retreatment of postoperative contrast-enhancing cryolesions found on initial short-term follow-up CT imaging with a tumor PADUA score <10 should be avoided.
At our institution, we rarely commence retreatment within 12 months of primary treatment, unless the initial follow-up CT detects convincing contrast enhancement consistent with residual unablated tumor and/or convincing recurrent disease. A protocol to biopsy lesions suspected for residual unablated tumor or recurrent disease has been started but the results are too preliminary for conclusions.
The present study is limited to being a single-center design with relatively few patients. Both LCA and PCA procedures have been included in the analysis, thus limiting the knowledge of each modality. In addition, no biopsies were taken from patients in whom spontaneous resolution occurred, thus limiting the knowledge of this group of patients. Future research should include longer follow-up time to investigate the course of cryolesions with spontaneous resolution as well as the phenomenon of delayed enhancement. Further investigation is also warranted into the significance of PADUA score in relation to treatment outcome and contrast-enhancing cryolesions, and more knowledge on the correlation between pathology and imaging would likely yield a greater understanding of contrast-enhancing cryolesions.
Conclusion
Contrast enhancement appears to be a frequent finding on initial CT following LCA or PCA of SRMs, which potentially could represent residual unablated tumor or recurrent disease. This phenomenon gives rise to diagnostic challenges because spontaneous resolution is commonly observed during follow-up in the first 12 months after treatment. In tumors with a PADUA score ≥10 and postoperative contrast enhancement >25 HU, residual unablated tumor or recurrent disease should be suspected.
Footnotes
Acknowledgments
The Danish Cancer Society, Karen Elise Jensen Fonden, and A.P. Møller Fonden have kindly supported the project financially. The results were presented, in part, at the 12th International Kidney Cancer Symposium, Chicago.
Author Disclosure Statement
No competing financial interests exist.