
Abstract
Purpose:
Laparoscopic trocar-site hernias (TSH) are rare, with a reported incidence of 1% or less. The incidence of occult radiographically evident hernias has not been described after robot-assisted urologic surgery. We evaluated the incidence and risk factors of this problem.
Materials and Methods:
A single-institution retrospective review of robot-assisted urologic surgery was performed from April 2009 to December 2012. Patients with preoperative and postoperative CT were included for analysis. Imaging was reviewed by two radiologists and one urologist.
Results:
One hundred four cases were identified, including 60 partial nephrectomy, 38 prostatectomy, and 6 cystectomy. Mean age was 58 years and mean body mass index (BMI) was 29 kg/m2. The cohort was 77% male. Ten total hernias were identified by CT in 8 patients, 2 of which were clinically evident hernias. Excluding these two hernias, occult port-site hernias were identified radiographically in seven patients. Per-patient incidence of occult TSH was 6.7% (7/104), and per-port incidence was 1.4% (8/564). All hernias were midline and 30% contained bowel. Eight of the 10 occurred at 12 mm sites (p = 0.0065) and 3 of the 10 occurred at extended incisions. Age, gender, BMI, smoking status, diabetes mellitus, immunosuppressive drug therapy, ASA score, procedure, blood loss, prior abdominal surgery, and history of hernia were not significant risk factors. Specimen size >40 g (p = 0.024) and wound infection (p = 0.0052) were significant risk factors.
Conclusion:
While the incidence of clinically evident port-site hernia remains low in robot-assisted urologic surgery, the incidence of CT-detected occult hernia was 6.7% in this series. These occurred most often in sites extended for specimen extraction and at larger port sites. This suggests more attention should be paid to fascial closure at these sites.
Introduction
T
According to Tonouchi and colleagues, the implementation of bladeless radially dilating trocars has reduced the incidence of postoperative hernias, but controversy surrounds the need to close the fascia on ports smaller than 12 mm. 4 A qualitative systematic review performed by Helgstrand and colleagues found that overall incidence of clinical hernias after laparoscopic surgery ranged from 0% to 5.2%, most often in port sites greater than 10 mm and in the periumbilical region. 5 Recent literature describing clinically evident port-site hernias in robot-assisted urologic surgery has found an incidence of 0.4% and 0.66%, again with a predilection for periumbilical 12 mm ports 6,7 Some investigators, however, have raised concern over clinically silent intrafascial hernias that conceal the true incidence of this concerning complication—potentially delaying intervention in affected patients. 7
In this study, we describe the incidence of both clinical and occult trocar-site hernias in robot-assisted urologic surgery using pre- and postoperative radiologic data. In addition, we outline the patient and surgical risk factors that contribute to their development.
Materials and Methods
A retrospective chart review of patients undergoing robot-assisted urologic surgery at the University of Virginia Health System between April 2009 and December 2012 was performed. Inclusion criteria identified all patients over the age of 18 who underwent robot-assisted partial nephrectomy, robot-assisted radical prostatectomy, or robot-assisted radical cystectomy. Of the extracted cases, a cohort was identified, for which both preoperative and postoperative abdominal CT data were available for the review. All patients were included regardless of specimen extraction site, port extension, and closure technique. Five to six port sites were generally used for the procedures, including two 12-mm nonbladed trocars (Ethicon Endo-Surgery, Cincinnati, OH), three 8-mm robotic da Vinci trocars (Intuitive Surgical, Sunnyvale, CA), and one 5 mm assistant port (Ethicon Endo-Surgery) (Fig. 1). All ports were established using longitudinal incisions. Fascia was routinely closed on 12 mm ports using a 0-polyglactin suture with or without the Carter-Thomason device (Cooper Surgical, Trumbull, CT). Use of the Carter-Thomason device was performed under direct vision to insure closure and was performed at the surgeon's discretion, based on patient factors, including body mass index (BMI). Fascia was not routinely closed on 8 or 5 mm ports. Skin was closed on all ports with 4-0 poliglecaprone in a subcuticular manner. Port-site hernias were diagnosed retrospectively based on identification of clear fascial defects on the cross-sectional CT scan by a single radiologist. A second radiologist independently reviewed the cases, and a urologist served as a third opinion for the single disagreement. In addition, clinically evident port-site hernias were identified using a chart review of postoperative visits. Hernias were further classified by size, contents, and trocar site. Abstracted data included patient demographics, BMI, prior abdominal surgery, preexisting comorbidities, immunosuppression, smoking status, preoperative hernia status, American Society of Anesthesiologists (ASA) score, port selection, extension, and closure, blood loss, specimen size, and postoperative signs and symptoms. Univariate and multivariate regression analyses were performed to identify those patient and surgical characteristics that were statistically significant predisposing factors for trocar-site herniation. Statistical analysis was performed with SAS 9.4 statistical software.
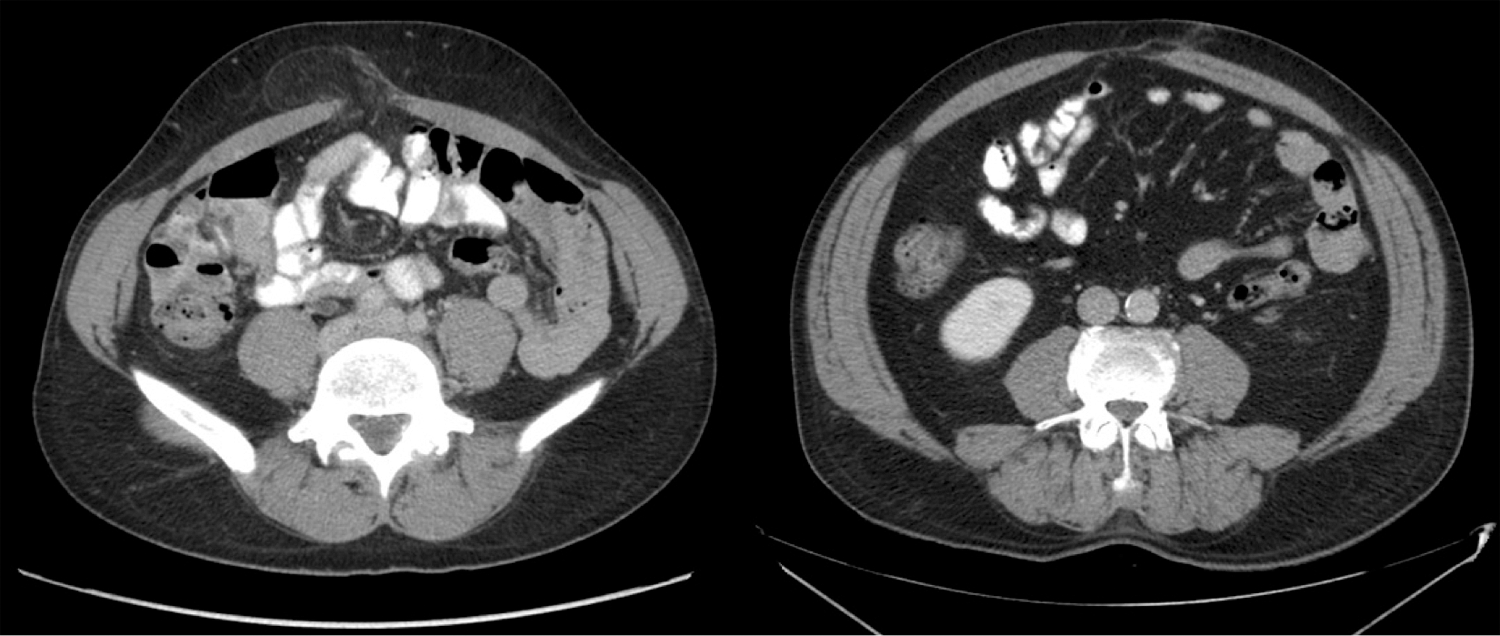
Representative CT images from this study of a symptomatic lower midline port-site hernia (left) and a clinically silent periumbilical port-site hernia (right) in two partial nephrectomies.
Results
Inclusion criteria identified 104 patients whose demographics are outlined in Table 1. The mean age was 58.1 years (range 33–76) and the majority of patients were male (76.9%). The mean BMI was 29.1 kg/m2 (range 19.9–48.0). Partial nephrectomy accounted for 57.7% of included cases, prostatectomy 36.5%, and cystectomy 5.8%. Indication for the postoperative CT scan was routine postoperative surveillance in the partial nephrectomy patients. The postprostatectomy and postcystectomy patients had indications, including incidental (for nonurologic problems), nausea, and abdominal pain. No CT scans were performed for suspected hernia. Mean interval from date of surgery to imaging was 337 days.
BMI = body mass index.
A total of 8 (7.7%) patients with 10 port-site hernias were identified. Two patients had clinical hernias; however, one of these patients had a total of three hernias, one was clinically evident, and two were radiographically occult. Therefore, 6.7% (7/104) of the patients in the study had radiographically occult hernias that were not detectable on physical examination. Details of these patients are shown in Table 2. Two patients (25%) required surgical repair, one of which was repaired laparoscopically with recurrence and eventual open revision. Seven of 10 hernias contained fat, while 3 contained bowel—2 of which were not identified clinically. Figure 1 contains examples of hernias detected in this study.
M = male; F = female; Inf. = inferior; PN = partial nephrectomy; RP = radical prostatectomy; Sup. = superior.
Figure 2 shows the location of each hernia based on surgery and port size. Among the trocar-site hernias that occurred after partial nephrectomies, four occurred around the 12 mm umbilical port sites, while two additional hernias occurred at 8 mm supraumbilical and infraumbilical robot arm sites. All hernias occurring after radical prostatectomy occurred around the 12 mm umbilical port sites.
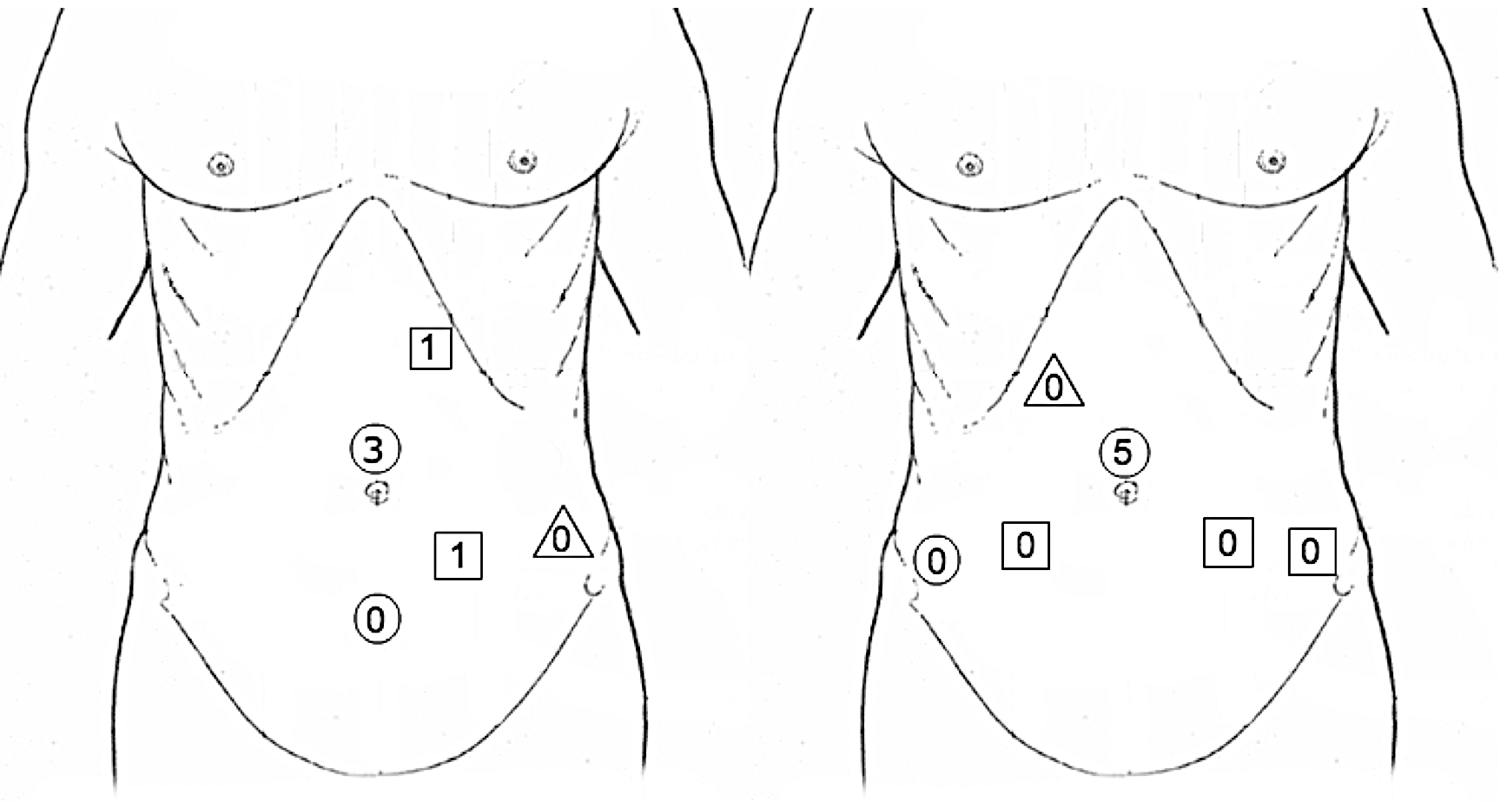
Trocar placement for left robot-assisted partial nephrectomy (left) and robot-assisted total prostatectomy or cystectomy (right). All partial nephrectomies have been converted to left for ease of representation. Circles represent 12 mm ports, squares represent 8 mm robot arm ports, while triangles represent 5 mm assistant ports. The number of radiographically detected hernias at each site is noted within the corresponding shape.
On a per total port analysis (Table 3), of 10 total hernias across 564 total ports (overall incidence 1.8%), none occurred in 104 five millimeter ports, two occurred in 252 eight millimeter ports, and eight occurred in 208 twelve millimeter ports. Three hernias occurred at sites where the incision had been extended to facilitate specimen extraction. The incidence of hernias in 12 mm ports was found to be statistically significant (p = 0.0065) for all hernias, but when calculated only for occult radiographically evident cases, hernias in 12 mm ports were no longer statistically significant (p = 0.11).
In the case–control analysis (Table 4), only postoperative incision infection (p = 0.004) and specimen size >40 g (p = 0.024) were found to have a statistically significant association with trocar-site hernia. All other extracted variables did not affect the incidence of hernia formation in this cohort. In addition, multivariate regression analysis was performed, but small sample size limited the study power to the extent that univariate analysis was deemed sufficient.
Discussion
Laparoscopy robot-assisted urologic surgery has numerous benefits over open procedures—faster recovery, less pain, and better aesthetic outcome. 1 TSH has been shown to be a potential complication with an incidence between 0% and 5.2% as reported by a systematic review of surgical literature. 5 Multiple investigators have attempted to determine whether the incidence of TSH is reduced with bladeless trocars 8,9 or fascial closure. 8,10 –12 This study did not seek to evaluate those factors as all 12 mm sites in our cohort were established using bladeless radially dilating trocars and closed at the fascial level.
Known risk factors for herniation include surgical variables (trocar size and location, closure at the fascial level, operative time) and patient characteristics (diabetes, malnutrition, smoking). 5,13 Accordingly, all 10 hernias in this cohort occurred at a midline location with 8 of the 10 occurring at 12 mm ports. The increased frequency around the midline may be due to the lack of abdominal wall musculature. In addition, specimens are often retrieved through the larger midline ports, which can result in widening of the fascial defect, or even necessitate extension of the incision. As with direct positioning injury, 14 robotic surgery might specifically predispose patients to trocar-site herniation over traditional laparoscopic techniques due to robot arm movement, patient slippage, and lack of haptic feedback leading to unrecognized excessive fascial tension and incision widening. In our cohort, 3 of 10 hernias were at sites extended for specimen extraction and specimens larger than 40 g resulted in a statistically significant increase in TSH. We recommend paying special attention to fascial closure at port sites used for extraction, especially if extended. In addition, future studies may undertake a comparison of specimen extraction at midline and off-midline ports to better characterize this predilection. Finally, it is well characterized that wound infection in open surgery predisposes to the development of incisional hernia, 15 and in our cohort, both patients who suffered from wound infections developed trocar-site hernias. Greater clinical suspicion for TSH in these patients is warranted.
Previous studies on TSH only report clinically evident hernias, which are more likely to present early with overt symptoms of bowel or omentum entrapment. 7 Late-onset hernias present more often with nonspecific pain, nausea, or generalized discomfort—symptoms that may not lead to clinical detection. 4,7 This study quantified the incidence of clinically silent hernias detected through postoperative imaging. In this cohort, only hernias in two patients were detected clinically (1.9%), while six patients were identified as having hernias on imaging alone (5.8%). Of those six clinically occult hernias, two contained bowel, a condition that often requires surgical repair. Although we do not recommend routine postoperative imaging in all patients undergoing urologic robot-assisted surgery, radiographically detected trocar-site herniation is an underrecognized clinical entity and care should be paid to fascial closure in patients at risk.
Several shortcomings for this study exist: the cohort was relatively small (n = 104) and the analysis was retrospective. In addition, there was a variable time interval between surgery and postoperative imaging, which could have resulted in the detection of hernias that were progressing toward clinical evidence. A single imaging series, however, would not be able to differentiate between stable and evolving hernias. Most significantly, this was a retrospective study using a cohort of convenience—we selected only those patients who underwent the robotic surgical procedures and had appropriate follow-up imaging. The majority of the cohort is represented by patients having partial nephrectomy, since our practice is to get routine CT follow-up in the first year after surgery. The postprostatectomy and postcystectomy patients in our cohort had other clinical issues that warranted CT imaging, but were not imaged in a systematic manner. This is concerning for sampling bias, as postoperative complications requiring imaging might also predispose to trocar-site herniation.
Conclusions
In our cohort, the incidence of clinically evident trocar-site hernias (1.9%) fell within the range of values reported in a systematic review of surgical literature (0%–5.2%), 5 but when clinically occult hernias detected by postoperative imaging are included in our analysis, the incidence rises to 7.7%. Factors identified in this study as contributors to trocar-site herniation were postoperative incision infection (p = 0.005) and specimen size >40 g (p = 0.017).
Footnotes
Acknowledgment
Study received institutional review board approval.
Author Disclosure Statement
No competing financial interests exist.