
Abstract
Introduction and Objectives:
Which ureteral stone can pass spontaneously? It is hard to answer this question exactly. The size and location of the stone are the most important predictors. However, there is still a considerable gray zone that needs to be clarified. We try to identify the role of stone volume (SV) in the prediction of spontaneous passage (SP).
Materials and Methods:
Seventy-eight patients with a solitary ureteral stone were retrospectively evaluated. Ureter SV measurements were taken in three planes and were calculated using the following formula: V = (X) × (Y) × (Z) × 0.52. SVs, and the longest diameters (LDs) were compared between patients who passed stones spontaneously and those who needed intervention.
Results:
The SVs and LDs were significantly lower in patients who passed stones spontaneously than in patients who required intervention (41.2 ± 35.5 vs 128.1 ± 91.1 mm3, p = 0.001; 5.7 ± 1.8 vs 7.4 ± 1.7 mm, p = 0.001). The optimum cutoff values were 7.0 mm and 52.6 mm3 for the LD and SV, respectively. For those stones of ≤7 mm, the volumes of the stones that could and could not pass did not differ significantly. However, the volume of the stones >7.0 mm that could pass was significantly higher than of those that could not. SP was 30.6% for stones >7 mm; however, when we removed the stones >52.6 mm3, SP increased to 75% for stones higher than 7 mm (p = 0.001).
Conclusions:
To classify ureteral stones using only one parameter such as stone diameter may lead to heterogeneity within the group. SV may be used in addition to size to determine a more definite homogeneous group to predict SP more precisely.
Introduction
U
Stone size and location are essential in choosing between intervention therapies and the more conservative approach. 5 Prior studies using radiography have examined the relationship between the spontaneous passage (SP) of ureteral stones and stone size and location. CT has replaced IVU, but for a long time, stone characteristics evaluated with CT only took into account the stone size and location.
The ureteral stone size is defined according to its longest diameter (LD) under CT. The size assessment of the stone is commonly undertaken using axial images. 6,7 However, elongated ureteral stones have their maximal diameter in the crania–caudal direction. Therefore, assessment of the maximal dimension from axial images alone provides an estimation rather than a measurement.
Multidetector CT enables the reconstruction of coronal images. Coronal images are more accurate for assessing crania–caudal stone dimension. Recently, there have been reports on the prediction of the SP of ureteral stones using size and area calculations from coronal images performed with multidetector CT. 8 –12 These studies reported better predicting rates than studies performed using axial CT images. Coronal reconstruction also enables the calculation of stone volume (SV). However, to the best of our knowledge, there has been no study evaluating the ureteral SV in the prediction of SP. The goal of this article is to determine whether ureteral SV assessment through coronal reconstruction of the unenhanced CT of the urinary tract alters the prediction rate of SP in a clinically significant manner for patients with a solitary ureteral stone.
Materials and Methods
Initially, 211 patients admitted to a urology outpatient clinic for acute renal colic due to a solitary ureteral stone were evaluated. Of the 211 patients, 133 were not eligible for the study. Those were patients with stones greater than 1 cm (n = 9), patients with hydronephrosis grade ≥3 (n = 6), and patients with a solitary kidney (n = 3). During follow-up, 67 patients underwent extracorporeal shockwave lithotripsy (ESWL) or ureteroscopy before 4 weeks of follow-up due to pain or renal function deterioration, and 48 patients did not complete the follow-up.
The CT images of the 78 patients who completed the follow-up were evaluated retrospectively for SV calculation.
CT images were acquired using a 16 multidetector-row CT scanner (MX-16; Philips Medical Systems, Best, The Netherlands). A noncontrast scan was taken from the diaphragm to the floor of the urinary bladder with the following parameters: 120 kVp, automatic adjusted mAs, and 16 × 2 mm collimation. The image matrix size was 512 × 512 pixels. From the raw data obtained from the CT scanner, axial–sagittal and coronal reconstruction images with a 1 mm thickness were analyzed.
A ureteral stone was defined as a dense radiopaque lesion in the ureter. Noncontrast CT scan images of 78 ureter stones from 78 patients were analyzed.
The CT images were transferred in the Digital Imaging and Communications in Medicine (DICOM) format to an extended workstation (2-GHz Pentium processor with 2014 MB of random access memory) for postprocessing.
The size of the ureteral stone was defined as its LD on either the axial, sagittal, or coronal images. The transverse diameter of the stone was measured on the coronal and axial images, the anteroposterior diameter was measured using axial and sagittal images, and the crania–caudal length was measured using coronal and sagittal reconstructions. LDs were used for volume measurement.
Ureter SV measurements taken in three planes (axial, sagittal, and coronal) were calculated using the following formula: V = (X) × (Y) × (Z) × 0.52.
The location of the calculus was classified as either being above the iliac vessels (proximal ureter) or below the iliac vessels (distal ureter). Patients with stones located at the ureteropelvic and ureterovesical junction were excluded from the study.
All patients took tamsulosin 0.4 mg daily for medical expulsive therapy. All patients were prescribed to use a maximum dose of diclofenac 150 mg daily for pain relief. Patients were followed weekly for 4 weeks with a plain abdominal film of kidney, ureter, and bladder, and an ultrasonography. If required, a low-dose noncontrast CT is used. Patient who did not pass stone spontaneously in 4 weeks underwent ureteroscopy or ESWL. The exclusion criteria included patients younger than 18 years old, multiple ureteral stones, congenital urinary anomalies, previous open or endoscopic ureteric surgery, pregnancy, solitary kidney, and a hydronephrosis grade ≥3.
Statistical analysis was performed using the PASW Statistics 18.0 for Windows (SPSS, Inc., Chicago, IL). The statistical significance was set at p < 0.05. Baseline variables were described using means and standard deviations or percentages, as appropriate. The data were tested for normal distribution using the Kolmogorov–Smirnov test. The Mann–Whitney U test was used to evaluate the difference between quantitative measurements that did not have normal distribution. All frequency comparisons were made using a chi-square test. The Spearman correlation was used to determine the relationship between the SV, diameter, and SP. To identify predictors of SP, univariate and multivariate logistic regression analyses were performed for gender, age, LD, SV, and dilatation. The adjusted odds ratio values and their 95% confidence intervals (CIs) were given. A receiver operating characteristic (ROC) curve analysis was performed to find an optimal cutoff value for LD and SV.
Results
The clinical and demographic characteristics of the patients and CT measurements are summarized in Table 1. The mean age of the patients was 42.2 ± 15.3 years. The mean age of the women and men was 42.7 ± 14.6 years, ages 19–67 and 45.4 ± 14.9 years, ages 18–72, respectively (p = 0.439).
Between the proximal and distal stones.
Statistically significant difference (p < 0.05) is indicated in bold type.
LD=longest diameter; SV=stone volume.
Most of the patients (71.8%) had a stone bigger than 5 mm. The mean size of the ureter stones was 6.4 ± 2.0 mm (2.4–9.8). The mean transverse, anteroposterior, and crania–caudal stone diameters were 4.0 ± 1.6 mm (1.6–9.0), 4.3 ± 1.7 mm (1.8–8.7), and 6.4 ± 2.0 mm (2.4–9.8), respectively.
Patients with proximal calculi (n = 24) had a significantly greater mean SV than patients with distal calculi (n = 54) (96.8 ± 81.7 mm3, range 12.0–355.6 mm3 vs 69.6 ± 75.1 mm3, range 5.5–300.1 mm3; p = 0.053 [Mann–Whitney U]) as well as a greater LD than those with distal calculi (7.1 ± 1.7 mm, range 3.2–9.8 mm vs 6.1 ± 2.0 mm, range 2.4–9.7 mm; p = 0.046 [independent t-test]). In the Spearman correlation analysis, SV and LD were significantly correlated with the stone position in the ureter (volume; Spearman's rho = 0.829, p = 0.001, and LD; Spearman's rho = 0.225, p = 0.048). SV and LD were not significantly correlated with passage time (volume; Spearman's rho = 0.243, p = 0.108, and LD; Spearman's rho = 0.234, p = 0.121).
Twenty-seven patients (57.7%) had passed a stone spontaneously within 4 weeks; their SVs and LDs were significantly lower than those of patients who needed intervention (41.2 ± 35.5 mm3, range 5.5–195.4 mm3 vs 128.1 ± 91.1 mm3, range 14.5–355.6 mm3, p = 0.001 [Mann–Whitney U]; 5.7 ± 1.8 mm, range 2.4–9.7 mm vs 7.4 ± 1.7 mm, range 3.3–9.8 mm, p = 0.001 [Mann–Whitney U]). SV and LD were significantly correlated to SP (volume; Spearman's rho = 0.575, p = 0.001 and LD; Spearman's rho = 0.458, p = 0.001).
Table 2 shows univariate and multivariate analyses as predictors of SP in patients. The univariate analysis demonstrated that a lower SV and LD were associated with a higher likelihood of SP. In the multivariate analysis, only SV was a significant predictor (p = 0.009).
Statistically significant difference (p < 0.05) is indicated in bold type.
CI, confidence interval.
The ROC curves of SV (area under the curve [AUC] = 0.836) and LD (AUC = 0.767) were plotted to find the optimum cutoff points for developing an adjusted multinomial logistic regression analysis. The optimum cutoff value for SV was 52.6 mm3, and for the longest stone diameter, it was 7.0 mm. The SP rate was 81.0% and 30.6% for stones with a diameter of ≤7.0 and >7.0 mm, respectively. SP was 85% and 28.9% for stones with a volume of ≤52.6 mm3 and >52.6 mm3, respectively. The SP time was not significantly related either to SV or LD (volume; Spearman's rho = 0.243, p = 0.108 and LD; Spearman's rho = 0.234, p = 0.121).
Stones with LD >7.0 mm that had spontaneously passed had a significantly lower volume than unpassed stones (p = 0.001, Mann–Whitney U test). The volume of the stones of 7.0 mm or less that had spontaneously passed was not significantly different from that of unpassed stones (p = 0.222, Mann–Whitney U test) (Fig. 1a).

Stones that had spontaneously passed, with a volume of 52.6 mm3 or less, had similar LDs to unpassed stones. However, stones that had spontaneously passed, with a volume >52.6 mm3, had significantly lower LD than unpassed stones (p = 0.009, Mann–Whitney U test) (Fig. 1b).
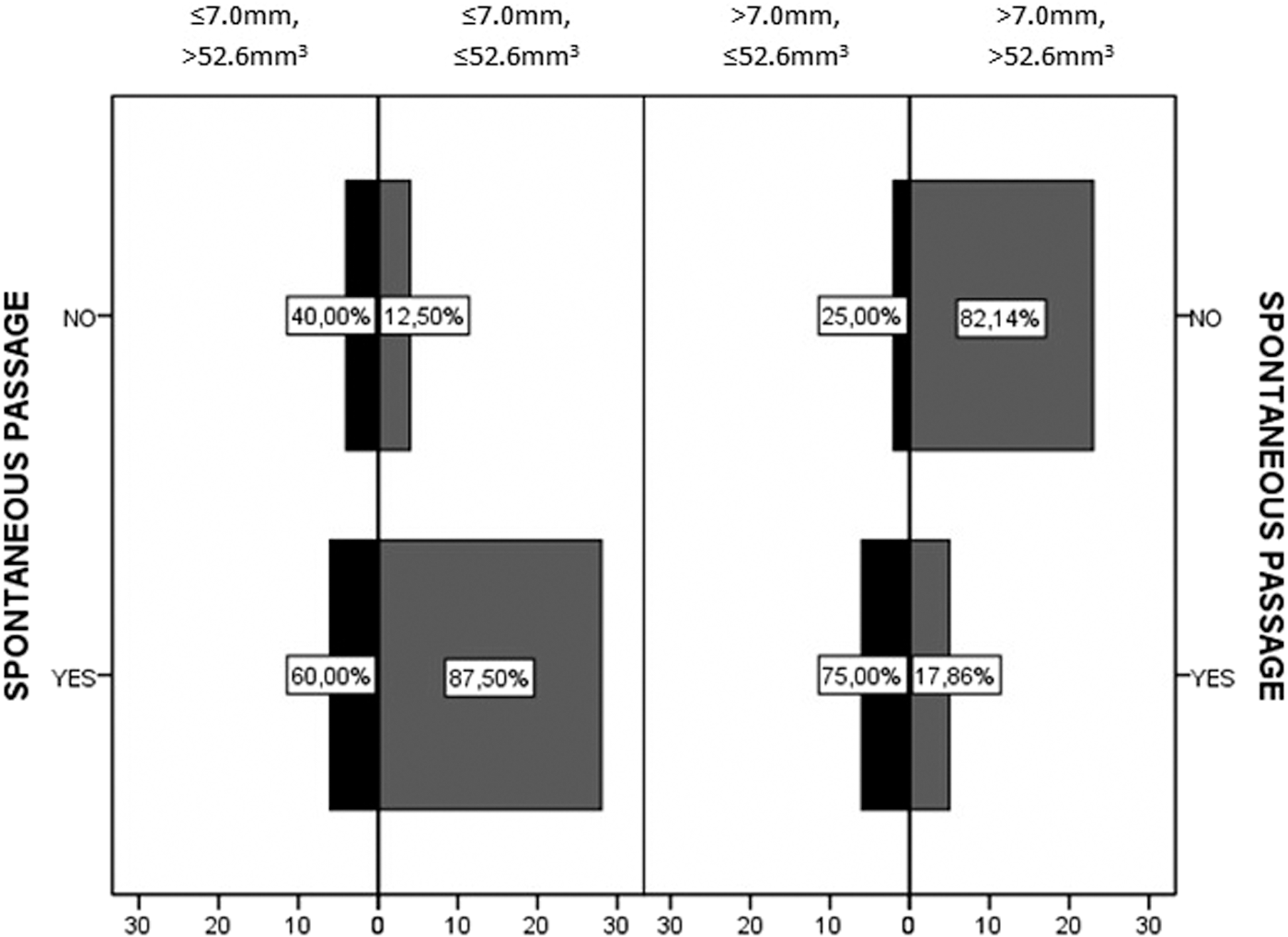
The SP rate was 81% for stones with an LD of ≤7.0 mm; SP increased to 87.5% when we used an SV of ≤52.6 mm3 in addition to a stone size of ≤7.0 mm. There was no statistically significant difference between SP of stones that had an LD and SV of ≤7.0 mm and >52.6 mm3 and of >7 mm and 52.6 mm3 (p = 0,059). SP was 30.6% for stones higher than 7 mm; however, when we removed the stones higher than 52.6 mm3, the SP increased to 75% (p = 0.001) (Fig. 2). In the multivariate analysis for SP, only SV was significantly correlated with passage (p = 0.034).
Spontaneously passed stones.
Discussion
The ureteral stone size and location are the most important factors in predicting SP. 9,12 –17 Building on the literature, we add the SV as a predictive factor in SP to the aforementioned parameters. To the best of our knowledge, no prior studies have examined the relationship between ureteral SV measured with unenhanced CT and the frequency of SP. We found a significant relationship between SV and SP.
Although various interventional techniques are available for ureteral stone treatment, waiting for SP with conservative treatment is the most preferred option in the management of ureteral stone cases. However, there is a considerable gray zone between conservative management and interventional therapy, and the decision to deliver interventional therapy is a difficult one for physicians to make. There have been many efforts to narrow this gap. Most studies have been confined to the size of the stone. 9,12 –19 A meta-analysis of the literature reported an overall SP rate of 68% for stones that are 5 mm or smaller and an SP rate of 47% for stones that are 5 mm or greater. 17 CT outcomes of multiplanar reconstructions such as SV may increase the predictability of ureteral stone SP.
Traditionally, the stone size is measured on axial CT images. Measurements of stone diameter with only axial images often underestimate the actual crania–caudal stone diameter. 9,20 Tchey et al. assessed crania–caudal stone dimensions with coronal reconstruction under CT, and they reported that stones smaller than 6 mm had an 88.7% chance of SP. 16 The SP rate for the same size of stones is lower in those studies that used only axial CT images. 15,17 We speculate that this is due to the underestimation of stone crania–caudal dimensions with axial CT images. Coronal reconstruction may contribute to the prediction of SP.
There have been further efforts to narrow the gray zone between interventional and conservative treatment, such as the measurement of stone area, using coronal reconstruction. Demehri et al. stated that the stone area might improve the accuracy in predicting SP of ureteral stones, particularly for those stones with a maximum diameter between 5 and 10 mm. 12
Coronal reconstruction of CT images enables a more accurate assessment of crania–caudal length and volumetric measurement. 9 There is no increase in the study time and exposure to ionizing radiation during coronal reconstruction.
In addition to stone size, we assessed the SV of the stones. Univariate analyses revealed that SV and LD were significant predictors of SP. However, in multivariate analyses, only SV was the significant predictor (Table 2).
Stones with an LD of ≤7.0 mm, which passed spontaneously, had lower volumes than stones that required interventional therapy; however, the difference was not statistically significant (Fig. 1a). The SP rate was 81% for stones with an LD of ≤7.0 mm; the SP increased to 87.5% when we set a volume limit of ≤52.6 mm3 in addition to a stone size of ≤7.0 mm (Fig. 2). SV did not make a significant difference in SP for stones with an LD of ≤7.0 mm.
The SP rate was 30.6% for stones with an LD of >7.0 mm when we classified the stones with an LD of >7 mm according to the SV; the SP rate increased more than twice for stones with a volume of ≤52.6 mm3 (75%).
To classify a ureteral stone using only the stone diameter may be inefficient. For example, in this study, stones greater than 7.0 mm had wide variability according to SV (Fig. 1a). To determine a more definite homogeneous group, SV may be used with size to lead to more accurate SP prediction.
To translate these findings into clinical practice, we composed two groups: (1) LD 7.0 mm or less and volume greater than 52.6 mm3 and (2) LD greater than 7.0 mm and volume 52.6 mm3 or less. The SP of the stones smaller than 52.6 mm3 but greater than 7.0 mm was 75%. However, of the stones smaller than 7.0 mm but greater than 52.6 mm3, only 60% passed spontaneously. In contrast with our classical knowledge, although the size of the stone increased, the SP rate did not decrease in patients with stones smaller than 52.6 mm3. When we also used SV to classify the stones, the size of the stones increased, but the SP rate increased in our study until the SV cutoff value.
A higher SV means a higher mass to be passed through the ureter by ureteral peristaltism. A higher SV also means a higher contact surface between the ureteral mucosa and the stone; this results in higher friction between the stone and the ureteral mucosa. 8 Due to these factors, we hypothesized that stones with high volumes require more energy to be passed through the ureter; this leads to a converse relationship between SV and SP. To address the natural history of SP in the ureter, we excluded patients with a history of previous stone passage, shockwave lithotripsy (SWL), percutaneous nephrostolithotomy (PCNL), or ureteroscopy, which may alter the passage of the stone due to inflammation or stricture.
Further clinical studies with a larger sample size are needed to clarify the role of ureteral SV in SP.
In the present study, SV has been found as an effective SP predictor of stones smaller than 1 cm. When the stones were divided into two groups according to LD, in the group of stones ≤7.0 mm, SV lost its significance. However, for stones greater than 7 mm, SV was the only significant predictor of SP.
Conclusions
Which ureteral stone can pass spontaneously? It is hard to answer this question exactly. The size and location of the stone are the most important predictors. However, there is still a considerable gray zone that needs to be clarified. Measurement of stone diameters in the coronal plane provides an exact assessment of the crania–caudal diameter, and this increases the predictability of SP. 8,16 Yet we are still a long way from accurate prediction. Determination of the ureteral SV may improve the predictive accuracy of SP, as the accuracy of SV was found to be superior to the accuracy of maximum stone size in predicting SP in this study. For stones greater than 7 mm in particular, in addition to LD, SV may be considered as a predictor and may contribute to a urologist predicting SP.
Footnotes
Author Disclosure Statement
No competing financial interests exist.