
Abstract
Objective:
To compare the operative outcomes of obese patients undergoing laparoendoscopic single-site (LESS) retroperitoneoscopic adrenalectomy or standard laparoscopic (LAP) retroperitoneoscopic adrenalectomy.
Methods:
Between September 2011 and April 2015, 51 obese patients underwent LESS retroperitoneoscopic adrenalectomy and their operative outcomes were compared with 65 obese patients who underwent standard retroperitoneoscopic adrenalectomy by the same surgeon. In the LESS group, a single-port access was positioned in the lumbar incision. The standard retroperitoneal adrenalectomy technique was performed with a combination of conventional and curved LAP instruments. The following parameters were adopted: patient demographics, surgical details, perioperative complications, postoperative outcome data, and short-term outcomes.
Results:
The LESS group was comparable with the LAP group in terms of total operative time (70.4 ± 21.3 vs 65.5 ± 24.8 minutes, p = 0.26), hospital length of stay (5.7 ± 1.2 vs 6.1 ± 1.5 days, p = 0.12), and incidence of complications (4/51 vs 5/65, p = 0.98) for patients with similar baseline demographics. The LESS group had significantly shorter surgical incisions (2.8 ± 0.3 vs 5.3 ± 0.6 cm, p < 0.0001), lower in-hospital analgesic requirement (7.6 ± 3.3 mg morphine equivalent vs 10.5 ± 6.2 mg, p = 0.003), and significantly superior scar satisfaction score (9.3 ± 0.7 vs 7.6 ± 1.4, p < 0.0001) than the LAP group. Although estimated blood loss was greater in the LESS group (28.1 ± 10.6 vs 16.9 ± 7.2 mL in the LAP group, p < 0.0001), <50 mL overall blood loss was not clinically significant. During a mean follow-up of 20.2 months, no recurrences or deaths were documented in either group.
Conclusions:
In properly selected patients, LESS retroperitoneoscopic adrenalectomy for obese individuals is technically feasible and safe in experienced hands, offering perioperative outcomes comparable with those of the conventional multiport approach, but with a superior cosmetic outcome.
Introduction
L
Consolidating multiple ports within a single skin incision means that LESS complements and expands the benefits of standard laparoscopic (LAP) surgery, including a much better cosmetic outcome, and lower incidences of wound infection and hemorrhage. Although LESS surgery may have even greater advantages in obese patients, performing LESS adrenalectomy in obese patients presents many technical challenges to the surgeon.
Substantial experience and refinement of the LESS technique are needed for it to be performed safely and effectively in obese patients. 8 –10 It is still not known whether the purported advantages of LESS adrenalectomy mean that it is a better option than standard LAP surgery in obese patients. The purpose of this study was to compare the perioperative outcomes of obese patients undergoing LESS retroperitoneoscopic adrenalectomy or standard LAP retroperitoneoscopic adrenalectomy.
Patients and Methods
Conduct of this retrospective study was approved by the ethics committee at Xiangya Hospital, Central South University, Changsha, Hunan Province, China. Written informed consent was obtained from all study participants. Between September 2011 and April 2015, 116 obese patients (49 men and 67 women) with a body mass index (BMI) >30 kg/m2 with benign adrenal tumors underwent surgical treatment at our institution. Of these, 51 underwent LESS retroperitoneoscopic adrenalectomy and 65 underwent standard retroperitoneoscopic adrenalectomy. All procedures were performed by the senior surgeon (X.C.), and in all cases, the diameter of the tumor was <4.0 cm. Patients were excluded from this study if they had bilateral adrenal tumors or there was a high suspicion of malignancy.
All patients were evaluated preoperatively by computed tomography or magnetic resonance abdominal imaging. The clinical characteristics of the patients are shown in Table 1. Data collected included patient demographics, surgical details, perioperative outcomes, and short-term patient satisfaction. Postoperative complications were graded using the Clavien–Dindo classification system. 11 A score on the visual analog pain scale (VAPS) (0–10; with 10 corresponding to the most intense pain) was recorded every 24 hours after the operation until discharge. Analgesic use from arrival in the postanesthesia care unit to discharge was analyzed using the mean morphine-equivalent doses. We administered a questionnaire 1 month postoperatively to assess the surgical scar satisfaction score (1–10) for each patient.
LESS = laparoendoscopic single-site; LAP = laparoscopic; BMI = body mass index; ASA = American Society of Anesthesiologists.
Operative technique
For conventional retroperitoneal LAP adrenalectomy, the patient was placed in the lateral decubitus position. The procedure was generally performed with three ports. A 2-cm transverse skin incision was made below the tip of the 12th rib. Vascular forceps were used to bluntly dissect the muscular layer and lumbodorsal fascia, and the retroperitoneal space was accessed using finger and balloon dissection. Then, under the guidance of the forefinger extending into the retroperitoneal space, a 10-mm trocar was placed 2 cm above the superior border of the iliac crest in the mid-axillary line to accommodate the camera, and a 5-mm trocar was placed approximately at the intersection of the anterior axillary line and subcostal margin of the 12th rib. Another 10-mm trocar was inserted into the retroperitoneal space through the initial incision, and the skin incision was closed by two towel clamps. After pneumoperitoneum was established with an intraretroperitoneal pressure of 12 to 14 mm Hg, the standard retroperitoneal adrenalectomy technique was performed.
The operative technique for LESS retroperitoneoscopic adrenalectomy has been described in our previous report. 6,7 Briefly, the patient was placed in the lateral decubitus position with appropriate flexion after induction of general anesthesia. A transverse skin incision of 2.5 to 3.0 cm was made along the lower margin of the 12th rib in the mid-axillary line. Vascular forceps were used to bluntly dissect the muscular layer and lumbodorsal fascia, and the retroperitoneal space was accessed using finger and balloon dissection as described previously. 12 A single-port access (Shikonghou, Hangzhou Tonglu, China) was then positioned in the lumbar incision. After pneumoperitoneum was established by CO2 at a pressure of 12 to 14 mm Hg, the standard retroperitoneal adrenalectomy technique was performed with a combination of conventional and curved LAP instruments (Fig. 1).

A single-port access site (Shikonghou, Hangzhou Tonglu, China) was positioned in the lumbar incision. After pneumoperitoneum was established by CO2 at a pressure of 12 to 14 mm Hg, the standard retroperitoneal adrenalectomy technique was performed with a combination of conventional and curved laparoscopic (LAP) instruments. Color images available online at
We routinely dissected and removed retroperitoneal fat and some excess perirenal fat to provide good visibility and expand the limited working space. Retroperitoneal fat and adjacent tissues outside Gerota's fascia were routinely dissected and removed through the inferior tube. Gerota's fascia was opened longitudinally and part of the flank pad surrounding the upper pole of the kidney was cleared away. Then, we exposed the upper pole of the kidney and dissociated the perirenal fat to expose the adrenal tumor. The adrenal vessels were clamped with Hem-o-lok clips (Teleflex, Athlone, Ireland) and divided or directly transected using a harmonic scalpel. After resection, the excised tumors were captured in a custom-made LAP bag and retrieved through the incision or removed directly through the inferior tube when tumors were small enough (Fig. 2). A rubber drain was left in situ through the incision when necessary.

After resection, the excised tumors were captured in a custom-made LAP bag and retrieved through the incision, or smaller tumors were removed directly through the inferior tube. Color images available online at
Statistical analyses were performed using SPSS version 20.0 (SPSS, Chicago, IL). Data are expressed as mean ± standard deviation (SD). Statistical analysis was performed using the chi-squared test for proportions and the Mann–Whitney U test for continuous variables. A p < 0.05 was considered statistically significant.
Results
Baseline demographic characteristics were broadly comparable between the groups with respect to patient age, sex, tumor size, laterality, BMI, and American Society of Anesthesiologists (ASA) physical status class (Table 1). Surgery was performed in all 51 patients undergoing LESS retroperitoneoscopic adrenalectomy; conversion to an open procedure or standard laparoscopy was not necessary in any case. Two patients in the LESS group needed an additional 10-mm trocar to be placed without extension of the incision, one because of a tear in the peritoneum and one owing to difficultly exposing the tumor. Retroperitoneal LAP was successful in all 65 patients; conversion to open surgery was not necessary in any case.
Table 2 summarizes the intraoperative and postoperative outcomes. The mean operative time was slightly longer in the LESS group, 70.4 ± 21.3 minutes, compared with 65.5 ± 24.8 minutes in the LAP group, but this difference was not statistically significant (p = 0.26). Although estimated blood loss (EBL) was greater in the LESS group (28.1 ± 10.6 mL compared with 16.9 ± 7.2 mL in the LAP group, p < 0.0001), at < 50 mL, overall blood loss was not clinically significant and no patient in either group required a blood transfusion. Two cases of pheochromocytoma in each of the two groups were managed without any undesirable hemodynamic fluctuations.
EBL = estimated blood loss; VAPS = visual analog pain scale.
The LESS group had significantly shorter surgical incisions (2.8 ± 0.3 vs 5.3 ± 0.6 cm, p < 0.0001), lower in-hospital analgesic requirement (7.6 ± 3.3 mg morphine equivalent vs 10.5 ± 6.2 mg, p = 0.003), and significantly superior scar satisfaction score (9.3 ± 0.7 vs 7.6 ± 1.4, p < 0.0001) than the LAP group. There was no significant difference in the time to resumption of oral intake (p = 0.22), length of hospital stay (p = 0.12), VAPS (p = 0.12), or the incidence of complications (p = 0.98) between the groups.
Complications occurred in four patients in the LESS group: there was one case of intraoperative peritoneal tear, two cases of postoperative subcutaneous emphysema (a grade I complication), and one case of postoperative pyrexia (a grade II complication). In the LAP group, one case of intraoperative peritoneal tear, two cases of postoperative subcutaneous emphysema, and two cases of postoperative wound infection (a grade II complication) that required treatment with oral antibiotics were documented. All complications were treated conservatively. During a mean follow-up of 20.2 months (range, 3–46 months), no recurrences or deaths were documented in either group.
Discussion
To the best of our knowledge, this is the first study to have compared the outcomes of LESS surgery with standard LAP surgery for adrenalectomy in obese patients. We found that outcomes are broadly comparable in this patient population. This is of clinical significance as many surgeons still adopt a cautious attitude toward performing LESS surgery in obese patients. Transperitoneal LESS surgery is reportedly a safe and feasible approach to adrenalectomy 11,13,14 ; however, most surgeons tend to select slim patients for this type of surgery. Arslan et al. 15 compared different surgical techniques for LAP and found that operation time, EBL, transfusion rate, and duration of hospital stay were less for the retroperitoneal group compared with the transperitoneal group, but there was no difference in the incidence of postoperative complications. They suggested that the retroperitoneal approach, especially with the patient in the prone position, could be a promising method for adrenalectomy in selected patients. Zhang and colleagues 16 compared LESS with standard retroperitoneoscopic adrenalectomy, including nine patients with a BMI > 30 kg/m2, and encountered no difficulties during port placement or dissection in any of the obese patients. Balogh et al. 17 have also recommended the use of a posterior retroperitoneoscopic approach for the management of adrenal masses in morbidly obese patients.
We also consider retroperitoneoscopic LESS adrenalectomy to be more advantageous in obese patients compared with transperitoneal approaches. First, in the lateral decubitus position with flexion, gravity causes abdominal wall adipose tissue to fall away from the operative side, and the resulting tension thins the remaining subcutaneous fat, facilitating insertion of the single-port device. Careful patient positioning with adequate padding of pressure points is particularly important. Second, the retroperitoneoscopic approach with the incision below the 12th rib allows a shorter route and better angle of approach to the adrenal masses compared with the transperitoneal technique, which may make it easier to dissect the adrenal gland and adrenal vein. Third, retroperitoneoscopic access does not require retraction or mobilization of the intraperitoneal organs, which may decrease the risk of organ injury and bowel-related complications.
Although the median operative time was similar between the two groups in our study, it is clear that intraoperative visualization, exposure of key landmarks, and control of bleeding are even more challenging in the obese patient undergoing LESS surgery compared with the standard procedure. Several studies have shown that excess visceral fat in the obese patient could be an obstacle to finding and maintaining the required dissection plane during the procedure. 8,9,18 Ersöz and colleagues 19 consider that manipulation of fatty tissues to gain access to deeper areas is particularly difficult in the obese and concluded that the amount of retroperitoneal fat is most closely associated with operative time in cases of LAP.
We suggest that the retroperitoneal fat lying outside of Gerota's fascia should routinely be dissected and removed, along with some of the excess perirenal fat, to achieve good visibility and expand the limited surgical field, especially in LESS procedures. Dealing with excess fat is often time-consuming; however, the single-port access that we used differs from the TriPort (Olympus, Tokyo, Japan) as its multichannel section can easily be removed from the tube. This modification allows excised adipose tissue, and even the tumor, to be removed quickly, thus shortening the operative time (Fig. 2).
Another advantage of the single-port platform is that the tube can be easily deformed to fit through the incision. When we encountered unexpected intraoperative difficulties during LESS procedures, we inserted an additional 10-mm trocar to the right of the single-port access through the original incision without needing to extend it (Fig. 3). Although it was inserted through the same incision, the additional trocar and the single-port access had two separate exports in the retroperitoneal cavity. This has some advantages. First, the ability to add the additional trocar without extending the incision retains the cosmetic advantage of LESS procedures. Second, it prevented gas leakage from the pneumoperitoneum caused by having two separate exports in the retroperitoneal cavity. Third, inserting a standard straight instrument through the additional trocar using the dominant hand reduces external clashing of instruments.

The tube of the single-port access could easily be manipulated to fit through the incision. When we encountered unexpected intraoperative difficulties during the laparoendoscopic single-site procedures, we inserted an additional 10-mm trocar on the right side of the single-port access through the original incision without extending the incision. Color images available online at
Meticulous hemostasis is necessary when undertaking LESS surgery in obese individuals as damaged vessels may retract and be hard to locate in the excess fat. Before adopting the LESS technique for adrenalectomy in obese patients, we had undertaken over 300 cases of LAP surgery on obese patients and dozens of LESS adrenalectomies in patients of normal weight, which abbreviated the learning curve.
Zhang and colleagues 20 are of the opinion that the thick abdominal wall interferes with and restricts the manipulation of surgical instruments in obese patients. The port that was used has a flexible and durable tube, which we chose instead of the TriPort retracting sleeve. This modification may help to retract wounds and effectively increase the size of incision that can be used to introduce other instruments at the same time. It also protects wounds from fascial tears or skin maceration when sharp instruments are introduced through the incision. Nonetheless, some gas leakage may also occur from the junction of the port when the instruments were lying approximately parallel to the abdominal wall owing to the need to manipulate them. Thus, further modifications of this port will be necessary.
Afaneh and colleagues 8 undertook a retrospective study comparing the outcomes of LESS donor nephrectomy with LAP donor nephrectomy in the obese population. Their results showed that there was no significant difference between the two groups in the length of the operation, EBL, complication rate, or length of hospital stay. Similarly, we found no significant difference in analgesic requirements, complication rate, or short-term convalescence between the two groups. These results may be explained, first, by the broadly comparable operation time of the two groups. Second, although LESS adrenalectomy has a shorter skin incision, internally its operative procedures, techniques, and scope are similar to those of the traditional LAP. Although in our study the LESS group had a statistically significantly higher EBL than the LAP group, mean blood loss was <50 mL in both groups, which we would argue was not clinically significant. In fact, intraoperative blood loss was negligible in all patients apart from two in the LESS group, who developed wound errhysis owing to fat saponification and lost 230 and 290 mL of blood each. These cases explain the higher mean EBL in the LESS group in our study.
The superior cosmetic outcome of LESS surgery is regarded as the main benefit of the procedure; patient satisfaction is higher, especially among younger patients and those with benign diseases. 21 It is recognized that the transperitoneal approach through the navel also had cosmetic advantages, but satisfaction with the cosmetic results of the retroperitoneal approach had not been studied. Evaluation of postoperative cosmetic advantage is a challenge owing to the lack of a reliable objective scale. Variations in patients' expectations and educational level and potential observer bias lead to difficulties in assessing cosmetic outcomes. In our series, the incision lengths are significantly shorter and the mean scar satisfaction score was higher in the LESS group than the LAP group. Our experience is that adrenal tumors <4.0 cm in diameter may be the most appropriate for LESS surgery as the tumor can be completely removed through a 2.5 to 3.0 cm incision without enlargement of the incision or morcellation, ensuring the optimum cosmetic outcome with single-port surgery (Fig. 4).
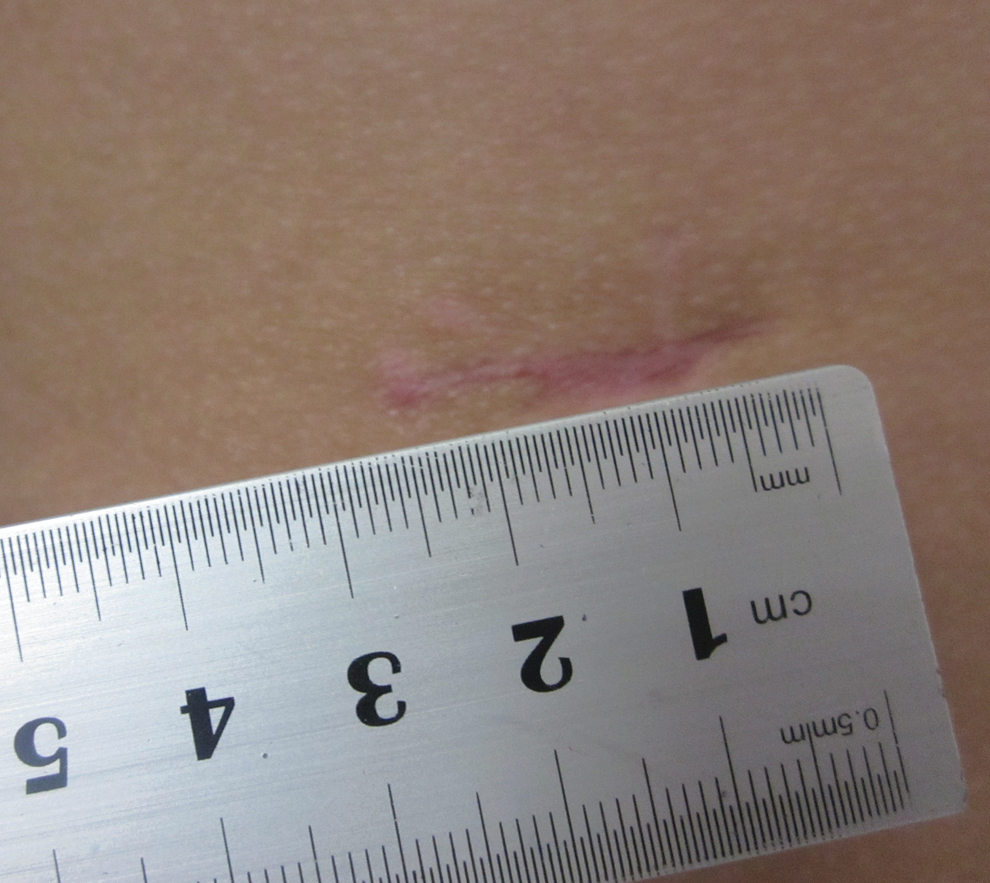
Incision of a 37-year-old man on the 45th postoperative day. Color images available online at
Although our results are encouraging, our study had several limitations. First, the distribution of adipose tissue differs greatly between individuals. 22,23 Patients' body composition, such as retroperitoneal fat area, is thought to be a more relevant factor influencing the technical difficulty during surgery than BMI. Several groups have reported that the visceral fat area is a more reliable parameter than BMI in predicting surgical outcomes after LAP. 18,24 Second, the perioperative outcomes of LESS retroperitoneoscopic adrenalectomy in obese patients might be influenced by laterality. We plan to undertake a study to examine the influence of visceral fat area, especially retroperitoneal fat area, and the side of the adrenal lesion on outcomes after LESS adrenalectomy. Finally, ours was a single-center retrospective study with a moderate sample size, and there may have been a selection bias as patients were not randomized to the study groups. Accordingly, prospective, randomized comparison studies based on larger populations and longer follow-up periods are needed to confirm whether LESS adrenalectomy is a better option than conventional LAP in obese patients.
Conclusions
In properly selected patients, LESS retroperitoneoscopic adrenalectomy for obese individuals is technically feasible and safe in experienced hands, offering perioperative outcomes comparable with those of the conventional multiport approach, but with a superior cosmetic outcome.
Footnotes
Author Disclosure Statement
No competing financial interests exist.