
Abstract
Background and Purpose:
To describe a novel and pure laparoscopic approach using a custom-made bulldog clamp with modified port placement for management of distal ureter during laparoscopic nephroureterectomy.
Patients and Methods:
Between October 2013 and December 2014, 31 patients found to have upper tract urothelial carcinoma were treated using this technique. After finishing a standard laparoscopic transperitoneal nephrectomy in a 45° to 60° recumbent position, an additional 12-mm trocar was inserted at the lower abdomen to allow the surgeon to continue dissecting the ureter caudally toward the bladder wall without repositioning the patient. The intramural ureter was separated from the surrounding detrusor muscle and down to the bladder mucosa, until a tent-shaped bladder cuff and intramural ureter could be formed by retraction in the superior and lateral directions. Then, a custom-made laparoscopic bulldog clamp was placed at the bottom of the tent-shaped structure to prevent urine spillage, and the bladder was closed by two-layer running closure using a barbed suture.
Results:
All surgeries were completed uneventfully. The mean operative time and estimated blood loss were 146.6 minutes and 47.3 mL, respectively. The median duration of the postoperative hospital stay was 6 days. No complications were noted. There were no positive margins in any specimen. No patients experienced stone formation or local or bladder recurrence during the 10.5-month follow-up period.
Conclusions:
Our novel technique fully replicates the open excision technique and conforms to the strictest oncologic principles while avoiding patient repositioning and the use of staplers (EndoGIA or Hemolock) to prevent stone formation.
Introduction
U
Although a variety of techniques have been described for the management of the distal ureter during LNU, including open excision (extravesical or transvesical), transurethral resection (pluck technique), the intussusception technique, the laparoscopic transvesical technique, and pure LNU (extravesical stapling technique), to date, no consensus has been reached on the optimal technique, because no technique has been shown to be significantly better than the others. The ideal technique for the management of the distal ureter during LNU should, most importantly, conform to the strictest oncologic principles, which are to remove the entire specimen en bloc without spillage of tumor cells during the bladder cuff excision, and second, the ideal technique should try to avoid patient repositioning to decrease intraoperative time.
Hence, in this article, we describe our novel technique of pure LNU for the management of distal ureter using a custom-made bulldog clamp that provides stronger closing force and has a more appropriate curvature than the ordinary clamp. This technique duplicates the open approach, namely precise en bloc removal of the complete bladder cuff without opening the urinary tract to prevent tumor spillage, and also eliminates the need for staplers (EndoGIA tissue stapler or large Hemolock clip) to avoid the risk of subsequent stone formation. In addition, we herein describe modified port placement, which allows access to both the kidney and ureterovesical junction without requiring patient repositioning.
Patients and Methods
Patients
Between October 2013 and December 2014, 31 patients (19 men and 12 women) found to have UTUC were treated with LNU using our bulldog clamp technique by one surgeon at Peking University First Hospital, Beijing, China. The patient clinicopathologic data were retrospectively collected and are summarized in Table 1. None of these patients had prior or concomitant bladder tumors. All tumors were staged based on the 2002 TNM classification of malignant tumors and were graded by the World Health Organization classification of 1998. 10
Surgical technique
After the induction of general anesthesia, the patient was placed in a semilateral decubitus position (45°–60° oblique position) with the lesion side up (the left side, e.g.) (Fig. 1A). Peritoneal insufflation was performed using the Veress needle technique at the left midclavicular line just inferior to the costal margin. A pneumoperitoneum was created by applying 14 mm Hg of CO2 pressure.
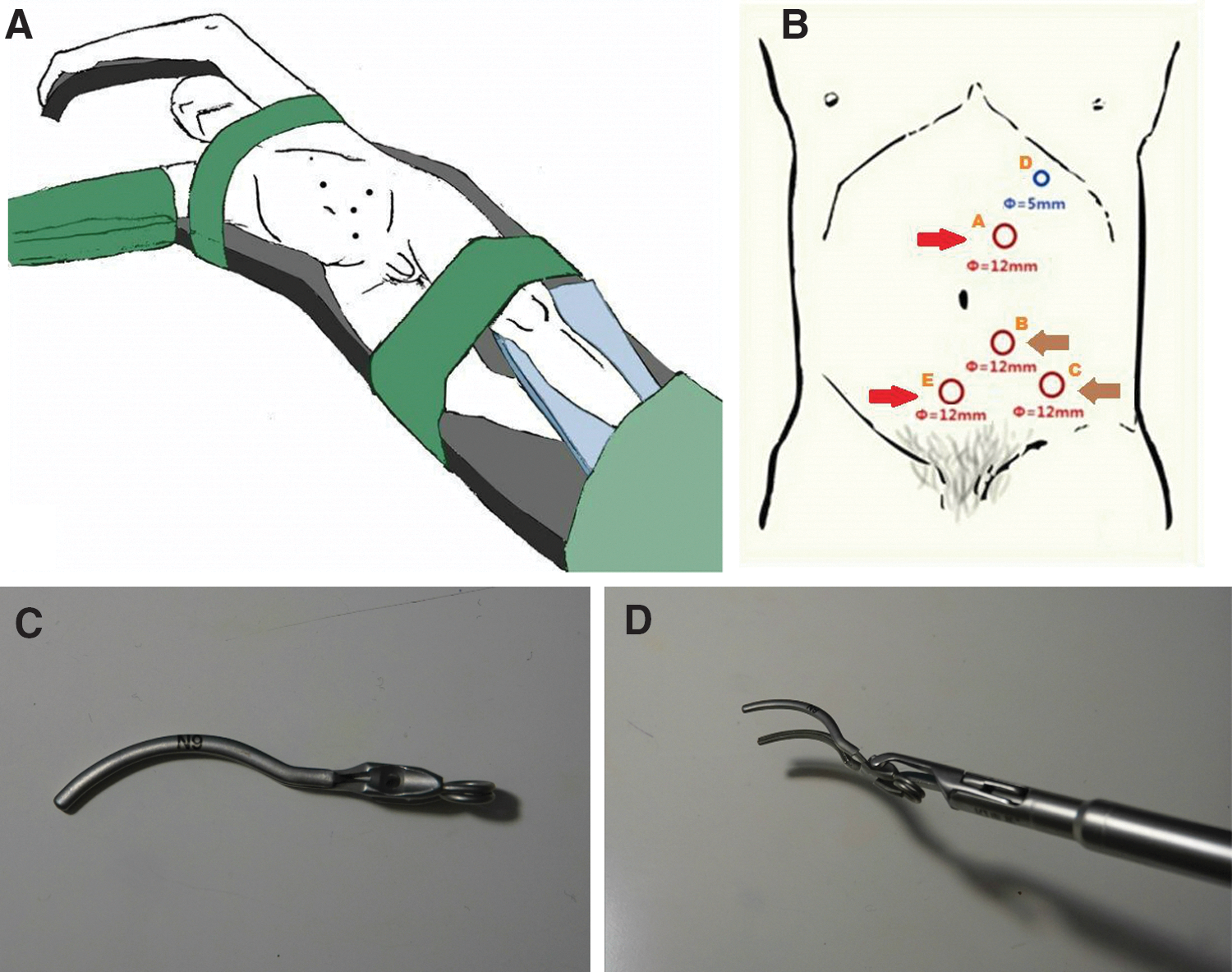
A 12-mm camera port (port A) was first placed 3 cm superior to the umbilicus at the lateral border of the left rectus muscle. Then, two 12-mm trocars, one 3 cm inferior to the umbilicus at the lateral border of the left rectus muscle (port B) and the other at the reverse McBurney point (port C), were inserted with direct laparoscopic visualization as the main trocars to be operated by the surgeon. Moreover, a 5-mm trocar (port D) was placed along the Veress needle at the left midclavicular line just inferior to the costal margin as an auxiliary trocar to be operated by the assistant (Fig. 1B). When the affected side was the right, the trocars' positions were symmetrically transposed, and an additional 5-mm trocar was necessarily placed inferior to the xiphoid at the midline, as needed for retraction of the liver.
Standard laparoscopic transperitoneal nephrectomy was performed, including mobilization of the colon, ligation of the renal hilum, and circumferential mobilization of the kidney, while leaving the ureter intact. Once dissection of the kidney and proximal ureter was complete, an additional 12-mm trocar was inserted in the lower abdomen at the midline (port E) to allow the surgeon to continue dissecting the ureter caudally toward the pelvis and bladder wall without patient repositioning. At this time, the camera port was changed to port B, and the surgeon used ports A and E as the working trocars, while the assistant used port C as the auxiliary trocar (Fig. 1B).
During further mobilization, the ureter was clipped distal to the tumor site to prevent intraluminal tumor seeding. By carefully dissecting the ureter over the iliac vessels down to the ureterovesical junction, the detrusor muscle fibers could be identified. Using a combination of blunt and sharp dissection, the intramural ureter was separated from the surrounding detrusor muscle and down to the bladder mucosa. A tent-shaped bladder mucosal cuff and intramural ureter were formed by retraction in the superior and lateral directions (Fig. 2A).

Then, a custom-made laparoscopic bulldog clamp (Fig. 1C), which provided a stronger closing force (9 Newtons) than the ordinary clamp and had a curved design (Fig. 1D) to fit the baseline of the cone-shape bladder cuff, was placed at the bottom of the tent-shaped structure to prevent urine spillage (Fig. 2B), and a Hemolock clip was used to occlude the distal ureter proximal to the site of the bulldog clamp. A bladder cuff was incised with endoscissors (Fig. 2C).
While keeping the bulldog clamp stationary, the closure of the bladder wall was performed in a two-layer running manner with full-thickness closure using a 1-0 barbed suture (Quill). The bulldog clamp was removed after finishing the first layer of the suture, while tightening the stitches (Fig. 2D). Finally, the en bloc specimen was extracted within an impermeable organ bag through a 6-cm incision that extended port E at the midline of the lower abdomen.
Results
All 31 cases using this new technique were completed uneventfully without conversion to open surgery or patient repositioning. The mean operative time was 146.6 minutes (range: 90–257 minutes). The mean estimated blood loss was 47.3 mL (range: 5–100 mL). There were no intraoperative complications.
With regard to postoperative pathology (Table 1), the mean tumor size was 3.66 cm (range: 1.5–7.5 cm). Twenty-two tumors were located in the renal pelvis and the others were located in the ureter. There were no positive margins in any patients. The pathologic stage was T1 in 16 patients, T2 in 11 patients, and T3 in 4 patients. The tumor grade was low in 21 patients and high in 10 patients. No concomitant carcinoma was found in situ.
The median postoperative hospital stay duration was 6 days (range: 4–8 days). No postoperative complications were found. The median follow-up duration was 10.5 months (range: 4–17 months). At the fist cystoscopic examination (usually 3 months after surgery), we detected that the affected side of the ureteral orifice was absent in all the 31 patients (Fig. 3). No patients have presented with evidence of local or secondary bladder recurrence and none of the patients was shown to have stone formation at the routine postoperative follow-up cystoscopy.
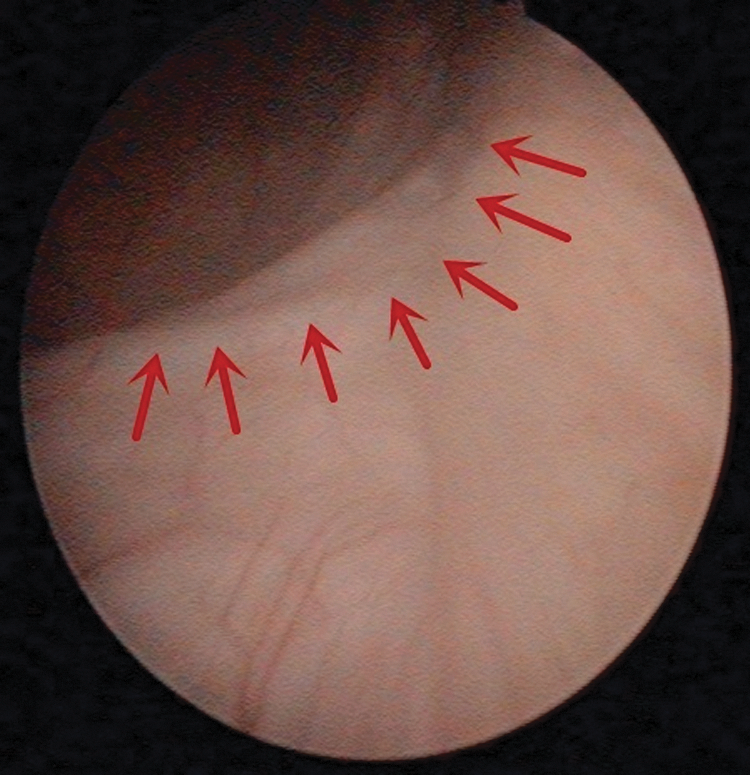
Postoperative cystoscopy showed the absent of ipsilateral orifice (red arrows).
Discussion
In terms of the treatment of UTUC, RNU with ipsilateral bladder cuff excision is the gold standard. Traditionally, this procedure is performed using an open approach, with either one large incision or two separate incisions. However, in 1991, the first LNU was described by Clayman and colleagues and, subsequently, this approach has spread throughout the world. 5 Over the past two decades, with the development of laparoscopy techniques and the advancements in surgical instruments, LNU has become a feasible and safe mini-invasive procedure for the treatment of UTUC in many centers with increasing frequency. 11 –13
The benefits of LNU have been shown to include less blood loss and perioperative pain, shorter hospital stays and faster convalescence compared with open RNU. 6 –8,14,15 Importantly, an increasing number of recent comparative studies have also shown that LNU is as oncologically efficacious as the open approach 9,16 ; thus, LNU should be the preferred surgical method for the treatment of patients with UTUC.
Currently, the greatest controversy regarding LNU is how to choose the optimal technique for the management of the distal ureter and bladder cuff. 17 In general, the distal ureter and bladder cuff handling techniques that are widely used in clinical practice can be divided into five categories, namely open excision (extravesical or transvesical), transurethral resection (pluck technique), the intussusception technique, the laparoscopic transvesical technique, and pure LNU (extravesical stapling technique), and each technique has its own advantages and disadvantages.
Open excision, especially by the transvesical approach through a lower midline or Gibson incision during LNU, adheres strictly to the oncologic principles and remains the most reliable procedure for ensuring complete bladder cuff excision; however, it has the disadvantage of requiring an additional incision, thus, increasing patient injury. In addition, this open approach may be difficult to perform in obese patients or those with a history of pelvic surgery.
Transurethral resection of the ureteral orifice and intramural ureter, followed by “plucking” of the entire distal ureter out of the bladder wall, is considered an alternative method that avoids the need for an extra incision and is associated with a shorter operative time compared with open excision. 18 The disadvantage of this method is the potential leakage of tumor cells from the upper tract into the perivesical space because of the lack of ureteral ligation before resection. This oncologic safety concern has been confirmed by many urologists who reported local recurrence results postoperatively. 11,19 Therefore, several modifications of ureteral occlusion before resection have been reported in the literature. 20,21
The intussusception technique, using a bulb-tipped ureteral catheter, can intussuscept the ureter into the bladder; then, the ureteral orifice is excised using endoscopic instruments. With the risk of potential tumor seeding, this procedure is confined to renal pelvic tumors and has not gained extensive acceptance among urological surgeons. 22
The laparoscopic transvesical technique uses two transvesically placed laparoscopic ports to ligate the ureteral orifice before detachment of distal ureter, and this allows for confirmation that the bladder cuff excision is intact. The main disadvantage of this approach is the possibility of port-site metastases, which may be caused by urine extravasation with tumor cells through the bladder wall defect. In addition, this method is technically difficult with a steep learning curve. 23,24 In summary, none of these four techniques is purely laparoscopic, resulting in the requirement of patient repositioning or the risk of urethral complication due to the use of endoscopic techniques.
Although the extravesical stapling technique is purely laparoscopic and thus has a shorter operative time and maintains a closed urinary system to avoid tumor spillage, concerns of inadequate bladder cuff resection and the risk of leaving viable tumor cells within the staple line, which was observed by Venkatesh and coworkers in a porcine model, 25 do exist. Indeed, higher incidences of positive surgical margins and local recurrence were reported by a number of authors, compared to other approaches of bladder cuff excision. 26,27 Moreover, it is difficult to handle the stapling device and the staples remaining within the bladder generate a risk of stone formation. 28,29 Hence, in our opinion, improvement of this purely laparoscopic technique is urgently needed to ensure the greatest reduction of surgical trauma concurrently with the greatest improvement in oncologic safety.
Our technique is a simple modification of the pure LNU technique that has several advantages. First, by using the custom-made laparoscopic bulldog clamp instead of tissue forceps, which are used in the open technique, our technique can fully replicate the open excision technique with en bloc removal of the complete distal ureter and bladder cuff without opening the urinary tract to prevent tumor spillage. When the intramural ureter was separated from the surrounding detrusor muscle and down to the bladder mucosa, a tent-shaped bladder mucosal cuff and intramural ureter could be detected by retraction in the superior and lateral directions; this ensures the excision of a sufficient amount of the bladder cuff. In the present study, for all cases, an en bloc bladder cuff excision with clear surgical margins both at the base and border of the specimen was achieved.
Second, by inserting an extra trocar (port E) at the midline of the lower abdomen and moving the instruments between ports, our technique facilitates the visualization of the distal ureter and bladder cuff to further assure precise bladder cuff excision during LNU without necessitating patient repositioning. Furthermore, when finishing the first layer of suturing of the bladder wall, the bulldog clamp is removed while the stitches are tightened. This scheme prevents the staple from being left in the bladder (EndoGIA tissue stapler or large Hemolock clip) and, subsequently, avoids the risk of stone formation. Finally, this simple modification does not have a steep learning curve if the urologist already has the ability to perform urinary reconstruction during laparoscopic prostatectomy.
This study has certain limitations, including the small number of patients and the short follow-up period. In addition, there is concern regarding the use of extravesical open excision; thus, caution must be taken, because theoretically, blind extravesical clamping of the distal ureter may involuntarily compromise the contralateral ureteral orifice. Nevertheless, in our study, no instances of contralateral ureteral orifice injury were found, as the distal ureter was carefully dissected. To further evaluate this new technique, studies with longer follow-up periods and larger patient cohorts are needed.
In addition, pure robot-assisted nephroureterectomy has been described by several authors with good surgical and oncologic outcomes. 30 We believe our bulldog clamp technique could be used in robot-assisted surgery and could decrease the difficulty of intracorporeal suturing. However, the availability of robots is still limited by their high cost in China.
Conclusions
Our novel bulldog clamp technique with modified port placement is a pure LNU approach that duplicates standard open RNU, namely precise en bloc removal of the complete distal ureter and bladder cuff without opening the urinary tract to prevent tumor spillage, and it also eliminates the need for staplers to avoid the risk of stone formation, without the need for patient repositioning. This method appears to be safe and feasible; however, studies with longer follow-up periods and larger patient cohorts are required to confirm our findings.
Footnotes
Acknowledgments
The authors thank the entire staff of the Department of Urology, Peking University First Hospital. This work was supported by grants from the Collaborative Research Foundation of Peking University Health Science Center and National Taiwan University, the College of Medicine (No. BMU20120318), the Natural Science Foundation of China (Nos. 81172419, 81372746), the Natural Science Foundation of Beijing (No. 7122183), the clinical features research of Capital (No. Z151100004015173), and the Research Foundation of Peking University First Hospital (No. 2015QN026).
Author Disclosure Statement
No competing financial interests exist.