
Abstract
Introduction:
Several anatomic and clinical factors have been implicated in the failure rates of shock wave lithotripsy (SWL), including the attenuating effects of bony structures. We designed an in vitro model that incorporates the lumbar spine, including vertebral bodies and transverse processes along the pathway of shockwaves, to mimic the clinical scenario during SWL of upper ureteral stones. We hypothesized that the presence of bone structures in the SWL pathway significantly affects the fragmentation rate.
Materials and Methods:
An ordnance gelatin (OG) model was conceptualized and created to allow a pig's lumbar spine to be embedded within it. Artificial urinary calculi weighing 2 ± 0.1 g (1.2-cm diameter) were prepared using BegoStone plaster. The trial was divided into two arms: group 1 models had OG only and served as the control and group 2 models had the bone embedded in the gelatin with stone wells placed above the transverse processes. Twenty-four stones per group were subjected to SWL using the STORZ MODULITH SLX-F2 lithotripter, using the same treatment parameters. Fragments were sieved through 2- and 4-mm filters, and the fragmentation coefficients (FC) were calculated. The Mann–Whitney test was used to compare FC between the two groups.
Results:
The mean fragmentation rate of group 1 was statistically significantly higher compared with group 2 using a 4-mm sieve (43% vs 0.62%, p < 0.001) and the 2-mm filter (18% vs 0.52%, p < 0.001).
Conclusions:
The presence of bone structures dramatically reduces the fragmentation rate of phantom stones using an OG in vitro model. The OG model is inexpensive and simple to use to simulate clinical situations during SWL.
Introduction
S
After shock waves are generated by the lithotripter and appropriate coupling is assured, energy waves propagate through the body until they reach the focal point and stone fragmentation occurs. 8,9 Shock waves can be attenuated along the way, that is, energy can be partially absorbed by the medium in which they move through and depends on the density of the medium. Attenuation will decrease the energy delivered to the focal point thus reducing the possibility of fragmentation. 10
It is well known that bony structures in the pelvis negatively affect the SWL efficacy for mid- and distal ureteral stones. For stones located in the proximal ureter and depending on the position of the lithotripter therapy head, bony structures may attenuate the energy delivery to the target. Despite the overall similar results comparing SWL and ureteroscopy (URS) for proximal ureteral stone management, 11 –13 we hypothesized that the presence of bone structures in the SWL pathway significantly affects the fragmentation rate in a novel in vitro model. We believe the effects of the transverse processes and lumbar spine are a less recognized cause for reducing the fragmentation of proximal ureteral stones. On the basis of our previous experience with in vitro studies for SWL, 14,15 (Alenezi, in press) we designed an ordnance gelatin (OG) model that incorporates the presence of transverse processes and lumbar spine along the pathway of shock waves to mimic the clinical scenario during SWL of proximal ureteral stones.
Materials and Methods
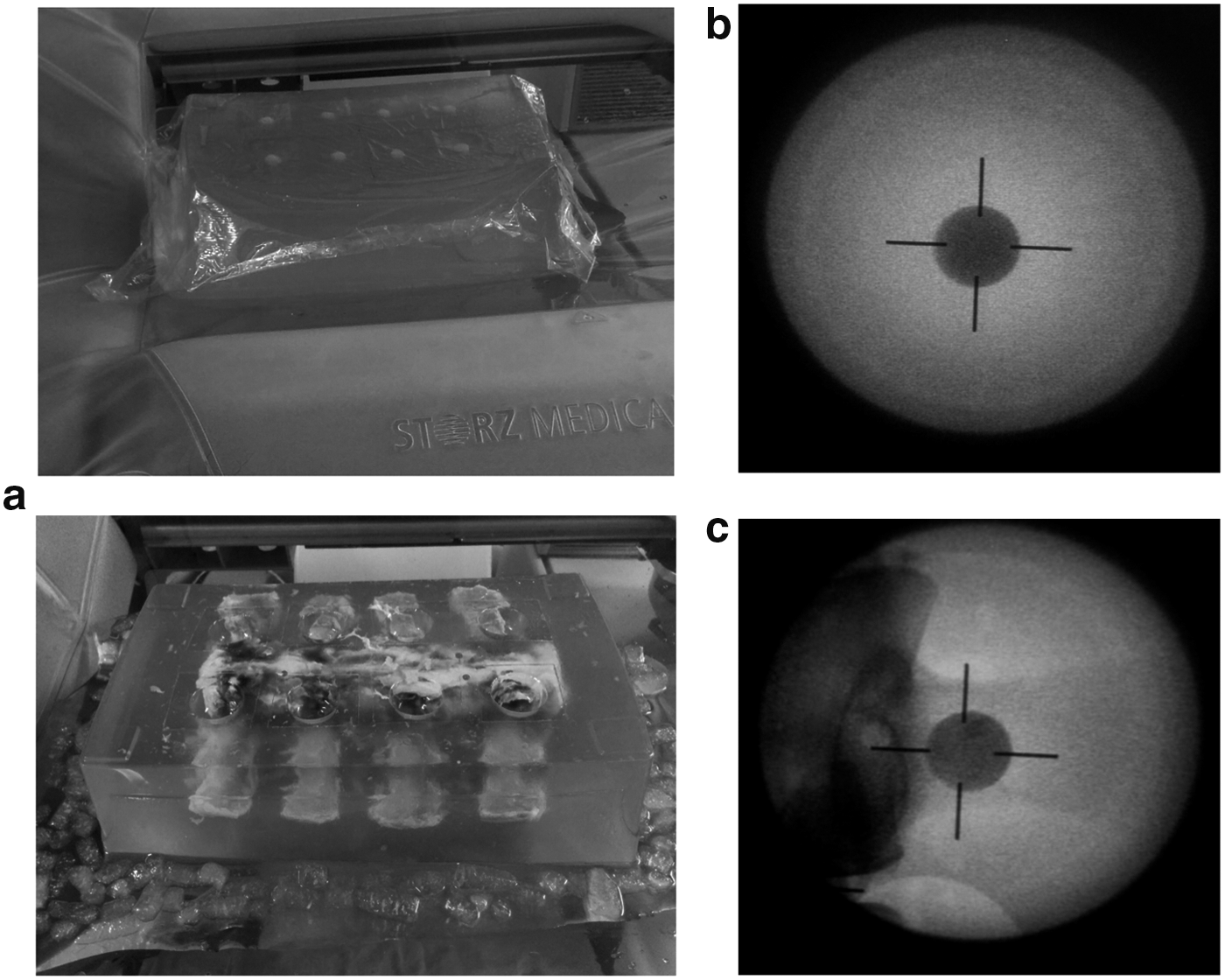
We developed the OG models according to the original description by Fackler and Malinowski 16 for ballistic studies. Previous studies have used this solution for an in vitro model to simulate soft tissue in SWL. 14,15 A 10% solution of unflavored gelatin in double-distilled water was poured into a plastic container (30 × 19 × 10 cm) containing eight semispherical polyethylene molds (diameter 3 cm, depth 2.5 cm), which created the stone wells. Experimental models were created by setting the lumbar spine in the plastic container before pouring the OG solution to simulate the anatomic characteristics of a stone located in the upper third of the ureter, as shown in Figure 1. Transverse processes of the lumbar spine were settled in front of the stone wells to mimic the clinical scenario of a patient being treated supine on the lithotripter (Fig. 2). Models were created and kept at 4°C until they were used.
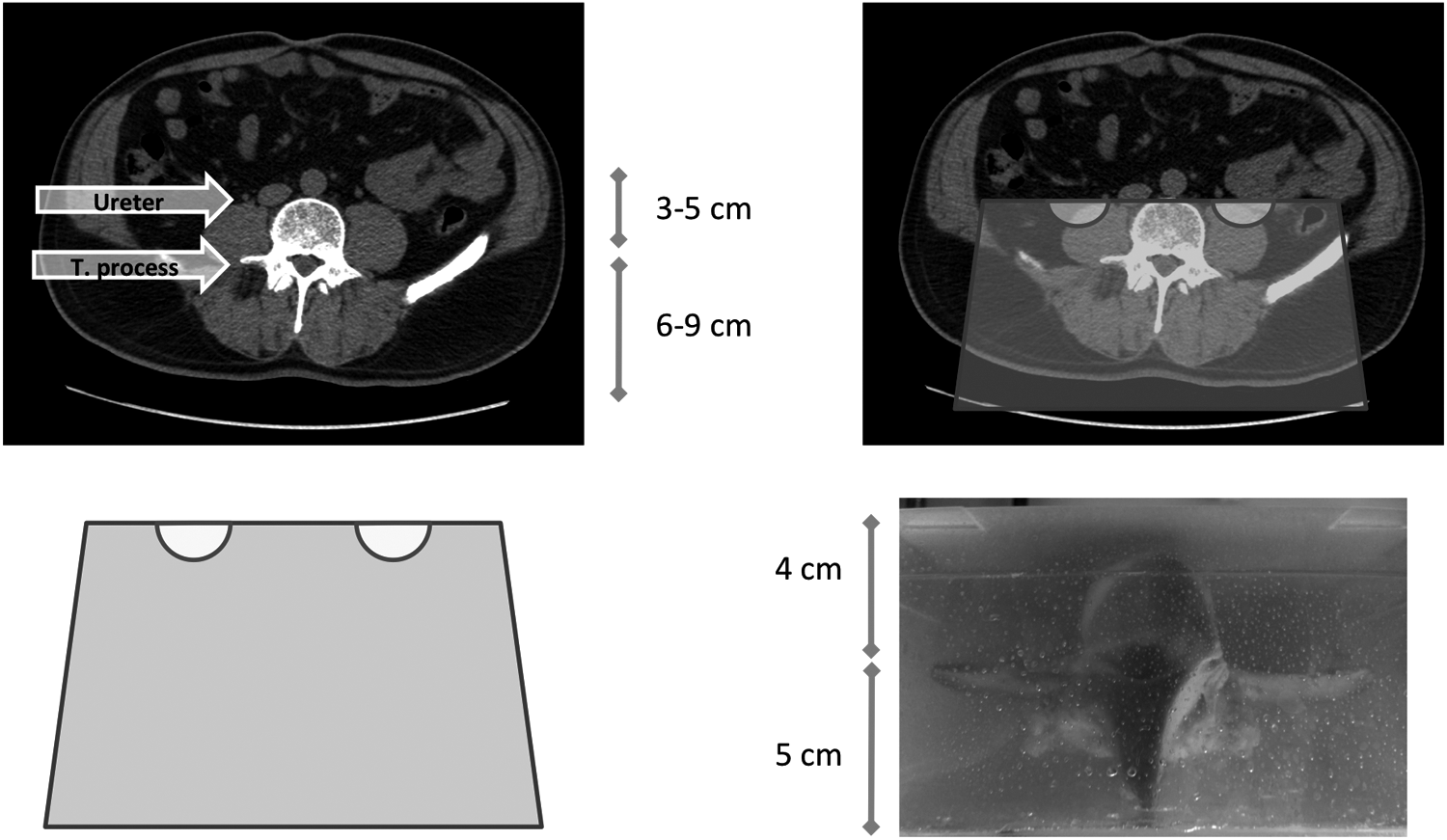
Schematic representation of the experimental design.
Several studies have evaluated the physical properties of different animal bones in the setting of biomaterial research. The pig bone structure is closely related to human bone in terms of mineral density and composition, along with its microstructure. 17,18 The lumbar spines used for the bone models were collected from a local abattoir and comprised four vertebral bodies en bloc. Fresh bones were cleaned to remove adjacent tissue and frozen at −18°C until set to create the experimental model.
Two initial models were made, the first without embedded bones and the second with an embedded porcine lumbar spine. These models were initially tested with phantom stones to determine the strength of the gelatin and the optimal SWL protocol. Testing of both models showed that 2000 shocks were sufficient to partially fragment the artificial calculi in the control model without causing disruption of the OG structure.
A stone model with a homogenous consistency to eliminate the variable of differing fragility to shock wave energy was needed. Artificial phantom stones made from BegoStone Plus (Bego), a super-hard plaster used for dental applications, which demonstrated similar physical properties to hard renal stones such as calcium oxalate monohydrate, were used. 19 Spherical artificial calculi were made according to the manufacturer's instructions using a 1.2- by 1-cm polystyrene mold. After 24 hours, stones were removed from the mold and manually sanded to achieve a 2000 ± 100 mg weight with a smooth surface.
Fragmentation coefficient (FC) was evaluated after shockwave lithotripsy was applied to the control and experimental models. The FC was calculated according to the following formula: 100 × (PreSWL weight–postSWL weight)/(preSWL weight). 20 A sample size of 23 stones per group was required to find a significant difference between the FC means, assuming an effect size of 1, with a power of 0.90, and a type I error of 0.05 (G*Power V. 3.1.9.2).
Models were placed on the lithotripter table and stone phantoms were positioned in each of the stone wells filled with 6 mL of human urine. The model was covered with plastic wrap and held on the table with an acrylic lid. Cold water was poured to facilitate coupling between the model and therapy head. After focusing the stone in three planes, the MODULITH SLX-F2 lithotripter (Storz Medical AG) was used to administer a total of 2000 shocks at a rate of 2 Hz, an energy level of 6 with the narrow focus, to each stone. The shock wave frequency and energy level settings were selected to represent our usual clinical practice and the manufacturer's recommendations. Fragments were retrieved from each stone well, air-dried overnight, and sieved through a 2- and 4-mm filter. The FC was calculated with the remaining fragments. Normality of the data was evaluated with the Shapiro–Wilk test. FCs from each group were analyzed and compared using the Mann–Whitney test. IBM SPSS Statistics for Windows, Version 20.0 (IBM) was used for statistical analysis.
Results
All models were constructed and shocked within 72 hours. Total cost of the materials used in the entire experiment was approximately 250 US dollars. Each OG model comprised eight stone wells and was subjected to approximately 138 (135–140) minutes of therapy. Three models were constructed per group to complete the previously calculated sample size of 24 stones per arm. The mean pretreatment weight of the 48 stones was 2031 ± 36 mg, range (1914–2082 mg), and the distribution of weight among the stones treated in the control and the experimental arm was similar (2029 ± 28 vs 2034 ± 43 mg, p = 0.27).
FCs for the stones treated in group 1 (control arm) using 2 and 4 mm cutoff points were 18% and 43%, respectively. Stones treated in group 2 were fragmented into large pieces or had a small indentation on the surface, where the focal point was located (Fig. 3). FCs were 0.52% and 0.62% for the 2- and 4-mm sieve, respectively, and were statistically significantly different to the FCs in the control arm (p < 0.0001). Table 1 summarizes the study findings.

Fragmentation among phantom stones.
Mann–Whitney test.
Discussion
SWL is the most common treatment used for patients with stones in the upper urinary tract. 21 Several clinical and radiologic factors have been associated with a higher SFR such as size <10 mm, 12 upper ureter location compared with mid- or distal ureter, skin-to-stone distance <10 cm, 3 and mean stone attenuation <1000 HU. 22 Moreover, different pre-SWL nomograms have been published, which predict SWL success; however, they are not widely generalizable due to many other factors not accounted for. 23,24 Despite the technologic advancements in endoscopic equipment, SWL remains a first-line treatment option for proximal ureteral stones. 12 It is noninvasive, has a low complication rate, and has acceptable stone-free rates with one treatment session.
Patient positioning has been recognized as an important variable in SWL outcomes, especially with ureteral stones. It is accepted that bony structures may attenuate the acoustic waves impacting the stone. Although supine positioning is most commonly used when treating renal and upper ureteral stones, it has been suggested that placing patients in the prone position may improve fragmentation if ribs or vertebral bone structures are close to the blast path. 25
Zomorrodi et al. in a small retrospective analysis concluded that prone positioning for upper ureteral calculi was safe and resulted in similar fragmentation rates compared with the supine approach (82.9% vs 81.8%) in 1.9 SWL sessions. 26 Hara et al. showed a superior fragmentation rate in patients with upper ureteral stones using a semilateral/rotated position to minimize the effect of bone structures. 27 On the contrary, Göktaş et al. did not find differences in stone-free rates at 3 months between supine and prone positions. 28 Phipps et al. evaluated the outcomes of SWL for distal ureteral stones, using a transgluteal approach to avoid pelvic bony structures. 29
Limitations of these studies include the inability to control for other important variables that theoretically might impact stone fragmentation rates such as stone composition, skin-to-stone distance, bowel gas interference with acoustic propagation in the prone position, and the location of the therapy head of the lithotripter.
We cannot make any specific recommendation about supine versus prone positioning being better for SWL in proximal ureteral stones based on our data alone. We have shown that, however, avoiding bony structures in the shock wave path will improve stone fragmentation rates and believe greater attention should be paid to optimizing patient positioning especially in those lithotripters that have a fixed treatment head. Correlation of the fluoroscopic imaging identifying potential bone-stone conflicts and preoperative imaging allowing measurement of skin-to-stone distance should be considered together, and may permit oblique repositioning of the patient to minimize bony structure interference.
To measure the impact of bone structures on stone fragmentation, we designed this in vitro study. Our previous experience with tissue simulation using OG facilitated the creation of this novel model. 14 We constructed a gelatin model with a pig's lumbar spine to simulate the clinical situation of a stone located in the upper ureter and used objective measures to compare treatment outcomes. The construction process was standardized, experimental models were tested to ensure their robustness, and clinically relevant SWL protocol was used.
Results revealed a dramatic reduction in the fragmentation of the stones treated in the experimental model. Most stones in the experimental arm showed fragmentation, but only into large pieces that did not pass through the sieve. Previous studies have used different cutoff values to evaluate in vitro fragmentation; therefore, we used both 2- and 4-mm sieves, and significant differences were found with both.
Our data provide an objective measurement of the deleterious impact of lumbar spine and transverse processes in stone fragmentation. Phantom stones have been shown to simulate calcium oxalate monohydrate characteristics, 19 one of the harder stones we face in clinical practice. The striking difference between the FC of the two groups may be related to the fixed position of the stone wells in the experimental arm, anterior to the transverse processes and close to the vertebral bodies (Fig. 2c).
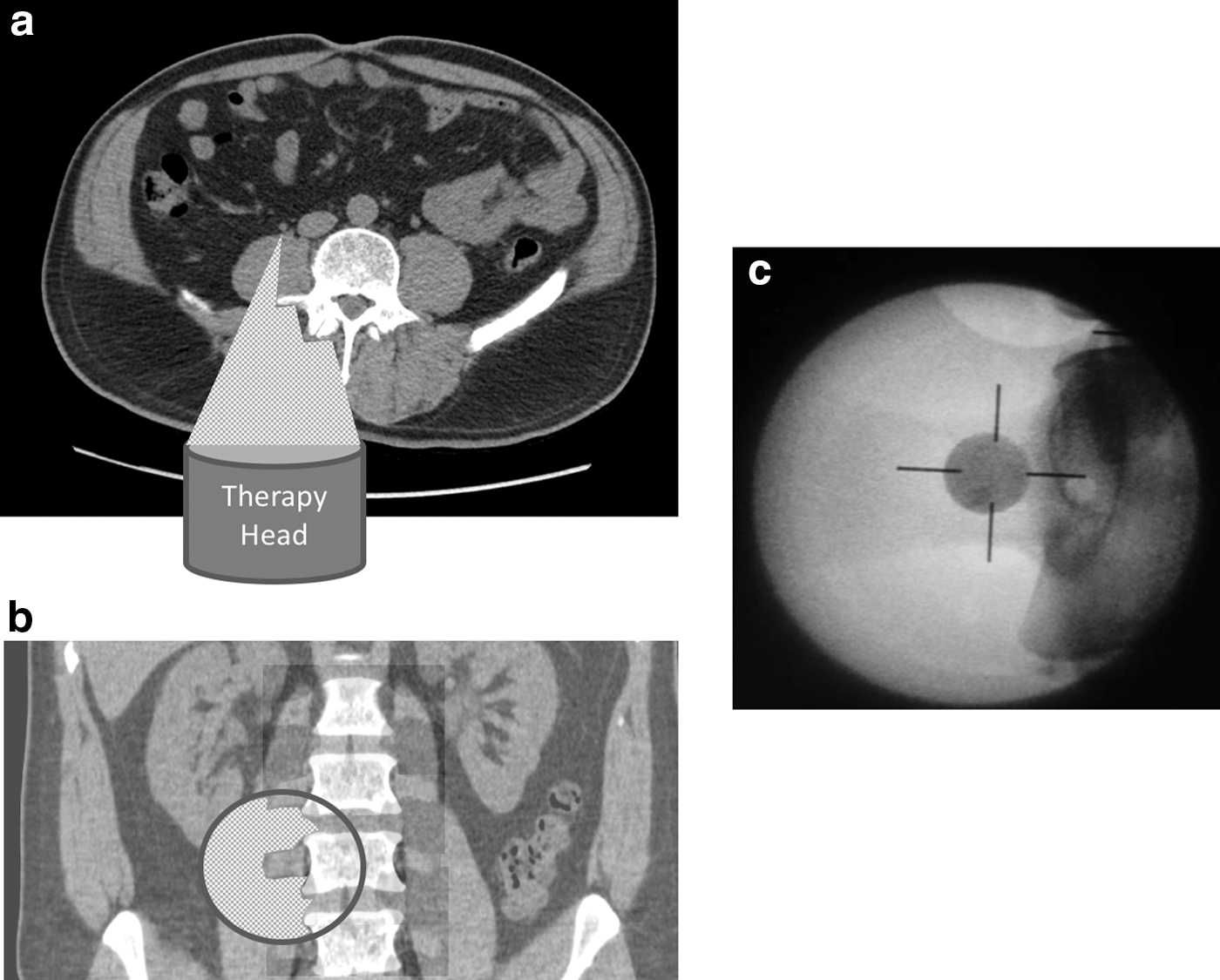
Limitations of this study include the fact that our results may not be applicable to all lithotripters. We have simulated the clinical situation using the STORZ MODULITH lithotripter, but results may not apply for the equipment where the therapy head is mobile such as with the Lithostar Modularis Variostar (Siemens) or the Sonolith (EDAP-TMS). In these machines, shock waves may travel through the flank of the patient avoiding bony lumbar structures for treatment of proximal ureteral stones.
It is acknowledged that this model may mimic the worse case scenario for SWL fragmentation of upper ureteral stones (Fig. 4). Clinically, the situation is likely to be more dynamic with ureteral peristalsis, urine flow, and patient respiration altering stone position relevant to the bony structures. As such, the magnitude of the effect of bony interference observed in this model may be less in clinical practice.
OG is widely used in ballistic research and is considered a soft tissue simulant, 30 however, it may not reflect the heterogeneous characteristics of different human tissues. This model was designed to simulate a stone located in the upper ureter, and the distances between the therapy head, the bone structures, and the stone wells were similar to what we might find in patients of average body habitus. Unfortunately, it was not possible to determine the magnitude of attenuation of shock waves in the model between the bone and gelatin compared with the interface of muscle and connective tissue to the lumbar spine in humans.
Another limitation of this study is that the phantom stones were hard. The impact of bone structures may not necessarily be as dramatic for softer stone compositions. In future studies, the FC could be evaluated using softer stones. Testing with a hydrophone could measure the acoustic pressure field to provide a more quantitative assessment of the attenuation effect. OG can be used effectively as a tissue simulator. It is relatively easy to use, inexpensive, and may be suitable to evaluate other shock wave parameters or treatment strategies.
Conclusions
The presence of bone structures dramatically reduces the fragmentation rate of phantom stones in this ordnance gelatin in vitro model. The OG model is inexpensive and simple to use allowing the simulation of several clinical situations during SWL.
Footnotes
Acknowledgment
The authors wish to thank the Mount Brydges abattoir staff for their assistance.
Author Disclosure Statement
The authors have nothing to disclose.