
Abstract
Background and Purpose:
To evaluate the safety and efficacy of a ring suture technique during retroperitoneal laparoscopic partial nephrectomy (RLPN) for management of renal cell carcinoma (RCC) in the renal hilum.
Patients and Methods:
Data for patients with renal hilar cancer who underwent RLPN from January 2010 to March 2015 were collected. All surgeries involved the ring suture technique, following the same procedure: the renal artery was dissected and clamped, the tumor was enucleated from the kidney, defects of the vascular and collecting system were repaired, and then the edge of the renal parenchyma was sutured continuously along the border. Finally, the renal artery clamp was removed, and any injury of the vascular system was repaired if necessary. We retrospectively analyzed renal ischemic time, blood loss, and postoperative complications.
Results:
Among the 17 patients, 11 were male (median age 61 years, range 42–71 years). Mean tumor diameter was 3.4 ± 0.9 cm and median R.E.N.A.L. nephrometry score was 8 (range 6–10). The mean warm ischemic time was 23.0 ± 9.2 minutes and median blood loss during surgery was 110 mL (range 70–350 mL); we had no case of uncontrollable massive bleeding. Radical nephrectomy was used in one case because of tumor embolus in a branch of the renal vein. All patients recovered well following surgery. Pathology confirmed the diagnosis of RCC in all cases, with the main subtype clear-cell carcinomas (88.2%).
Conclusions:
The ring suture technique is safe and effective for management of renal hilar cancer during RLPN for selected patients.
Introduction
R
Surgical resection remains the gold standard for curative treatment of localized RCC. Partial nephrectomy (PN) is a reference standard for T1 tumors and is recommended by several guidelines. PN has comparable oncological outcomes to radical nephrectomy (RN) and results in less postoperative chronic kidney disease, associated with morbid cardiovascular events, and better postoperative renal function and quality of life. 4,5
Laparoscopic PN (LPN) has gained popularity as minimally invasive surgery. Studies with limited follow-up have indicated that it has similar oncologic outcome as open PN. 6,7 LPN can be performed efficiently and effectively by the transperitoneal or retroperitoneal approach. However, the retroperitoneal approach is predominant in most centers in China because of direct access to the kidney and urologists' familiarity with the retroperitoneal anatomy.
LPN for certain tumor locations, such as renal hilar masses, especially those located posteriorly, can be challenging even in experienced hands. One challenge for hilar cancer is renorrhaphy following tumor resection because of limited tissue left for reconstruction and nearness to the main branches of renal vascular.
The purpose of this study was to validate the feasibility and efficacy of retroperitoneal LPN (RLPN) for hilar tumors by using a ring suture technique developed and adopted at our center to manage complicated renal masses undergoing PN.
Patients and Methods
Patients
Between January 2010 and March 2015, 17 consecutive patients with renal hilar cancer underwent the ring suture technique during RLPN. Metastatic disease was excluded by plain X-ray of the chest (routine) or bone or brain scan (according to clinical indication). Hilar cancer was defined as renal cortical tumors located in the renal hilar zone and contacting the renal artery, vein, or both directly as identified on preoperative CT. Clinical data were collected retrospectively. The R.E.N.A.L. nephrometry score was determined according to preoperative CT images. 8 If the tumor was close to the collecting system, a 5F ureteral catheter was placed preoperatively into the pelvis of the involved kidney for retrograde injection of saline with indigo carmine dye during surgery.
Data on patient demographic characteristics, tumor size, nephrometry score, warm ischemic time, blood loss, and postoperative complications were collected retrospectively. Patients were followed up at 3 months for urinalysis, serum creatinine level, and enhanced CT scan.
Surgical technique
All surgeries were performed according to the same protocol by experienced laparoscopic surgeons under general anesthesia. The retroperitoneal approach was adopted for all procedures. The patient was placed in a modified lateral decubitus (full flank) position similar to that described previously by our institution. 9 Generally, we use three ports for posterior renal hilar tumors and four for anterior tumors (Fig. 1). The first port is placed at the lateral border of the erector spinae muscle, 2 cm below the 12th rib by an open technique. A small incision is made 2 cm below the 12th rib, and the retroperitoneum is accessed by piercing the muscle layers with a hemostat at the lateral border of the erector spinae muscle. Then, a balloon dilator is used to open the working space. The second port is placed 2 cm above the iliac crest at the middle axillary line. The third port is placed at the anterior axillary line 2 cm below the costal margin. The fourth port is placed at the anterior axillary line about 6 cm beside the second port to facilitate management of an anterior hilar tumor.

Port distribution in retroperitoneal laparoscopic partial nephrectomy.
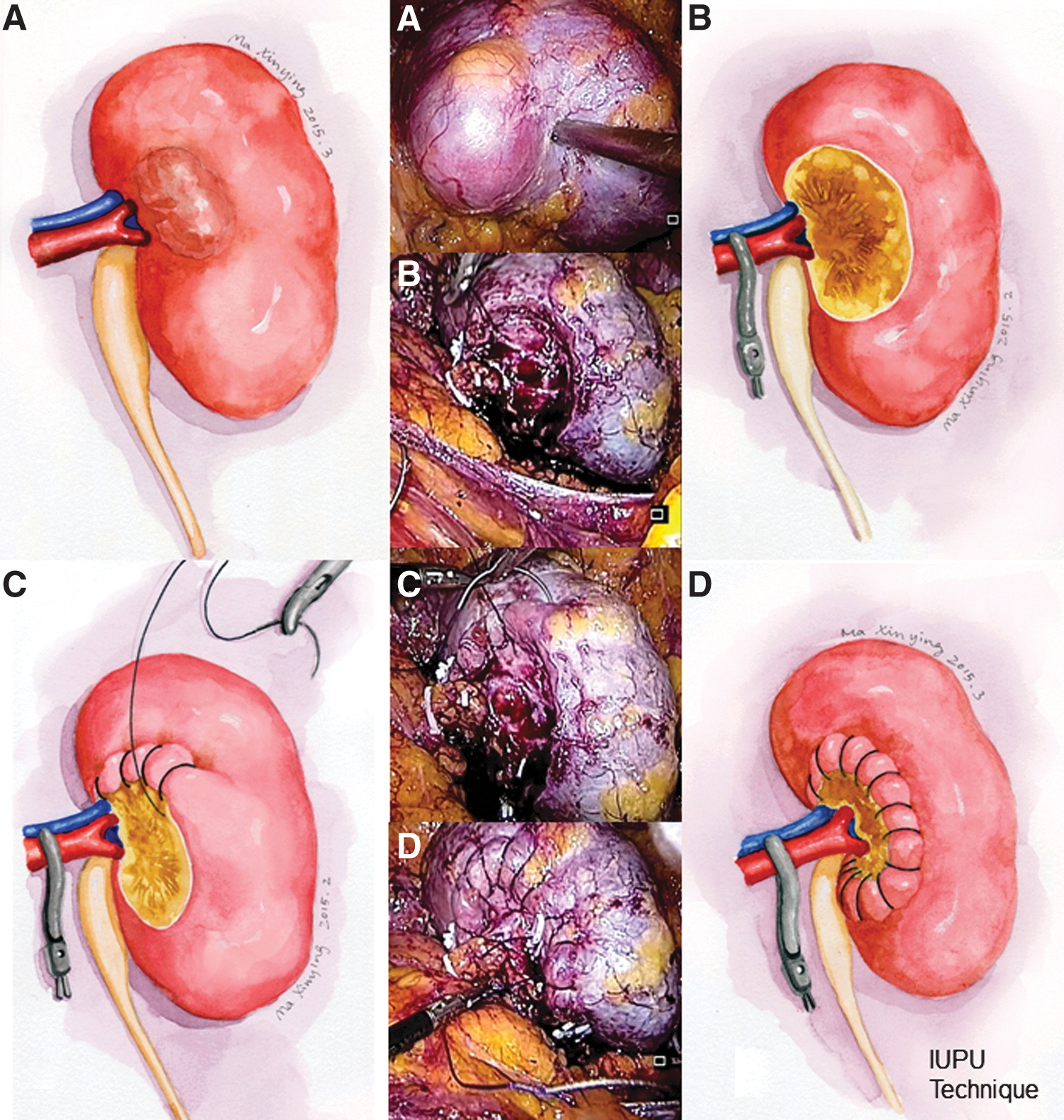
After extraperitoneal fat is cleared, the Gerota fascia is incised sharply. Then, the kidney is mobilized thoroughly along the surface of the renal capsule to obtain maximal mobility of the kidney and adequate exposure of the tumor (Fig. 2A). The renal artery is dissected and mobilized gently. An amount of 12.5 g mannitol is administered intravenously before a bulldog clamp is placed on the artery. Then the tumor is enucleated from the kidney by blunt and sharp dissection. The vascular system feeding the tumor is tied by the use of clips (Fig. 2B). Then, apparent defects of the vascular and collecting system are repaired. Saline with indigo carmine dye is retrogradely injected through the ureteral catheter placed preoperatively to identify collecting system damage if needed. The edge of the renal parenchyma is sutured continuously along the border with a 0-0 absorbable unidirectional barbed suture (Quill PDO suture, 36-mm 1/2 circle tapper point needle) (Fig. 2C). The stitches should stay close to the edge of tumor bed and involve the full thickness of the parenchyma. The tumor bed is excluded from the suture and kept open. Finally, the renal artery clamp is removed, and any injury to the vascular system is repaired (Fig. 2D). An amount of 10 mg intravenous furosemide is administered after the clamp is removed. The specimen is put into a laparoscopic entrapment sac and retrieved from the port below the 12th rib (the first port).
Results
Among the 17 patients, 11 were male (median age 61 years, range 42–71 years; Table 1). Mean tumor diameter was 3.4 ± 0.9 cm (range 2.9–4.7 cm) and median R.E.N.A.L. nephrometry score was 8 (range 6–10). Mean warm ischemic time was 23.0 ± 9.2 minutes (range 18–43 minutes). Median estimated blood loss during surgery was 110 mL (range 70–350 mL); we found no uncontrollable massive bleeding. RN was used in one case because of a tumor embolus in branches of the renal vein. All patients recovered well following surgery. Most drainage tubes were withdrawn on day 2 postoperatively. Pathology confirmed the diagnosis of RCC in all cases; the main subtype was clear-cell carcinoma (88.2%). The overall Fuhrman grade distribution was 17.6%, 47.1%, and 35.3% for Fuhrman 1, 2, and 3 tumors, respectively. No patients had positive surgical margins. Patients were followed up at 3 months postoperatively, with no postoperative hemorrhage, urine leakage, hematuria, or renal atrophy. All patients had normal serum creatinine level.
RCC = renal cell carcinoma
Discussion
In this study, we used a novel renorrhaphy method, a ring suture technique, to manage complicated renal hilar cancer. Among the 17 consecutive patients with hilar cancer, the mean tumor diameter was 3.4 ± 0.9 cm (2.9–4.7 cm) and median R.E.N.A.L. nephrometry score was 8 (range 6–10), so these were complicated cases and difficult to manage by traditional renorrhaphy. However, all surgeries were successful with the ring suture technique. No case was transferred to open surgery or RN except one with a tumor embolus in a branch of the renal vein. The ring suture technique has advantages over traditional techniques in managing complicated hilar cancer.
PN is a standard treatment for localized RCC, especially for small renal masses. LPN has similar oncologic outcome as open PN. 6,7 However, specific tumor locations can increase the difficulty of LPN, and renal hilar cancer is considered one of the most challenging locations, even in experienced hands. Renal hilar cancer implies challenges in access and resection 10 and in renorrhaphy. Renorrhaphy is a crucial step in LPN and has a close relationship with both hemostasis and minimizing postoperative complications. Several techniques devised to facilitate the suture procedure include the sliding clips technique and V-Hilar Suture Renorrhaphy. 11,12
Traditional renorrhaphy, which we commonly use, involves two layers of suture: the first layer to suture the tumor bed and the second to suture the edge of the parenchyma. 13 Following suture, the resection defect should be closed perfectly. However, for renal hilar tumors, the traditional suture method may be not suitable, especially for large tumors. First, the tumor bed for a hilar mass is renal sinus fat, which contains the main branches of the vascular and collecting system. So the first-layer suture may cause damage and compression to the renal sinus content. Second, the suture might cut through the parenchyma because of the thinness of the hilar parenchyma, especially when closing surgical wounds of the kidney, which leads to high tension of the thread. 14 Finally, with significant hemorrhage or hematuria following clamp removal, there are two choices: transfer to RN or redo PN.
In our new renorrhaphy ring suture technique, we do not perform the first-layer suture. Instead, we use tumor enucleation to avoid unexpected injures to the vascular and collecting system. During the tumor enucleation step, only tumor feeding vessels are ligated. In addition, any extra damage is repaired following tumor resection. Without the first-layer suture, accidental injuries to the main vascular branches running in renal sinus fat are not a concern. So, the technique can preserve the vessels supplying blood to healthy parenchyma. The technique does not require closing the renal defect. In contrast, we keep the wound open. Different from the second-layer suture with the traditional technique, in our technique, a continuous suture is used along the edge of parenchyma defect, which keeps the suture tension free and avoids a “cheese cutting” effect. 14 If severe hemorrhage or hematuria is encountered following clamp removal, we can also use fixation because the tumor bed is kept open.
In our study, no patient had positive surgical margins. Another technique is tumor enucleation. We prefer blunt dissection along the surface of the tumor pseudocapsule, which avoids excessive vascular or collecting system rupture. Also, it does not increase the risk of positive surgical margins and has similar oncologic outcomes as a sharp excision. 15 –17 Several studies have focused on this patient group, 10,12,18 and our technique had comparable results. However, our technique simplifies the LPN procedure and reduces the difficulty of the LPN technique, so it differs from that used in previous studies. The ring suture technique could also be used in open and robotic surgeries and for the management of endophytic tumor, large tumors, and other complicated cases. In our consecutive patient cohort, no patient experienced uncontrollable massive bleeding during surgery; no case was transferred to open PN or laparoscopic RN except one with a tumor embolus in a branch of the renal vein. No patient had postoperative complications. The technique was safe and can be used for the management of complicated renal hilar cancer when LPN is considered.
Our study has a few limitations, including small sample size, retrospective nature, and no control group undergoing traditional LPN. Nevertheless, our study was a preliminary study that verified the safety and feasibility of the ring suture technique in experienced hands for selected patients.
Conclusions
We report the preliminary results of use of a ring suture technique for the management of renal hilar cancer during RLPN for selected patients. The method is safe and effective. It simplifies the LPN procedure and reduces the difficulty of LPN. The technique is a valuable and reasonable option for laparoscopic surgeons managing renal hilar cancer and other complicated renal masses.
Footnotes
Acknowledgment
The authors thank Ms. Xinying Ma for her excellent medical illustrations.
Disclosure Statement
No competing financial interests exist.