
Abstract
Objectives:
To demonstrate the feasibility of our novel natural orifice transluminal endoscopic surgery (NOTES)-assisted approach with medium-term follow-up.
Patients and Methods:
From March 2012, we included all patients who presented to our clinic with symptomatic or complicated retentive bladder diverticula secondary to long-standing infravesical obstruction. After managing the primary cause, we proceeded in all cases to our novel NOTES-assisted approach. We followed up the patients with abdominal ultrasonography at 6 weeks and 12 months postoperatively. Success was determined as subjective relief of the symptoms and objective disappearance of the diverticula in postoperative retrograde cystogram (RGC).
Results:
Between March 2012 and August 2014, eight diverticula were treated using our new technique. The surgery was uneventful. The mean operative time was 134.25 ± 44.92 minutes. Blood loss was minimal (>50 mL). Retrograde cystography was performed on the 10th postoperative day. The introduction of the needle holder through the urethral natural orifice (NOTES) facilitated a more optimal direction of the needle holder for suturing the bladder wall due to its parallel position in relation to the trigone and posterolateral walls. This renders this step easier compared with suturing the bladder wall through the transvesical laparoscopic ports. One case had a grade IIIa complication according to the Clavien–Dindo classification of surgical complications. The study is limited by the small number of cases.
Conclusion:
Laparoscopic transvesical bladder diverticulectomy is a promising and safe procedure with good outcomes. Using the urethra (NOTES assisted) as an extra access to the bladder facilitates diverticular traction and bladder suturing without the need for extra ports. This technique can also be applied together with the novel T-laparoendoscopic single-site surgery approach.
Introduction
T
Yeung and colleagues have described a novel technique for laparoscopic transvesical cross-trigonal ureteral reimplantation for management of vesicoureteral reflux through creation of pneumovesicum with good outcome. 9 This approach was used for management of other urologic procedures, such as distal ureterectomy with bladder cuff excision for upper urothelial carcinoma. 10,11
Pansadoro and colleagues described an elegant and minimally invasive technique to excise bladder diverticula laparoscopically using transvesical approach. 12 With the evolution of laparoendoscopic single-site surgery (LESS), Stolzenburg and colleagues first described LESS for the management of bladder diverticulectomy transvesically through umbilical incision; however, this required bladder closure at the end of the procedure. 13 Afterward, Roslan and colleagues published a small case series for transvesical laparoendoscopic single-site surgery (T-LESS) with good efficacy. However, the small operative field and clashing of instruments added more challenge to the procedure. 1
We present our novel natural orifice transluminal endoscopic surgery (NOTES)-assisted laparoscopic transvesical approach for the management of retentive bladder diverticula, in which the urethra offers an extra access to the diverticula. We assessed the feasibility, clinical outcomes, and their medium-term follow-up.
Patients and Methods
From March 2012 to August 2014, we operated four patients with the excision of a total of eight symptomatic secondary diverticula using our new NOTES-assisted technique. In all patients, we investigated and proceeded to the management of the primary etiology first before performing bladder diverticulectomy. A detailed description of the patients' preoperative details and indications for intervention are listed in Table 1.
PVR = postvoid residual; UTI = urinary tract infection.
The diagnosis was established through pre- and postvoid ultrasonography with the assessment of the diverticular diameter and anteroposterior and oblique retrograde cystography with postvoid films. The mean diverticular size was 4.4 ± 1.83 cm.
After obtaining written informed consent, the patients were scheduled for operation. In the following section, the operation will be described step-by-step.
• The patient is placed in the lithotomy position under general anesthesia.
• Diagnostic cystoscopy is performed to: ○ Observe the position of the diverticula in relation to the ureteral orifices, followed by the insertion of ureteral catheters when the diverticulum is located near the orifice or intramural part of the ureter. ○ Inspect diverticula from the inside for tumors or suspected lesions. ○ Place special self-retentive optic 10-mm trocar and two working 5-mm trocars with internal balloons (Fig. 2) in a flat triangular pattern (Fig. 1) into the full bladder under cystoscopic guidance.
• Creation of pneumovesicum until 12 mm Hg pressure is achieved.
• Circumferential incision of the mouth of the diverticulum using monopolar electrocautery scissors (Fig. 3).
• Grasping the diverticular mucosa and separating it from the detrusor muscle attachments using both blunt and sharp dissection (Fig. 4).
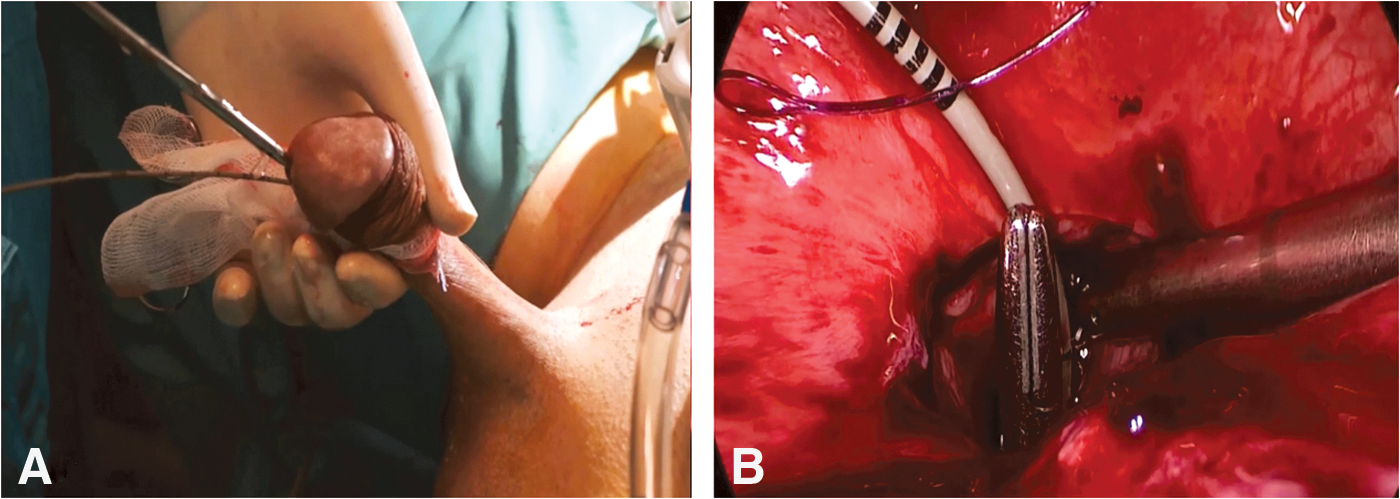
• In a scenario of large diverticula, a blunt-tipped grasper is inserted through the urethra as an extra port (NOTES assisted) after lubrication to perform traction on the diverticular mucosa.
• After complete separation of the diverticular mucosa, the excised mucosa is extracted with cystoscopy through the urethra to avoid extraction through the narrow 5-mm ports with possible loading of the specimen inside the trocar in cases of large diverticulum.
• Ensure adequate hemostasis at the surgical bed.
• Insertion of (V-Loc®; Covidien) 2/0 suture on a 5/8 round needle through the camera port into the bladder.
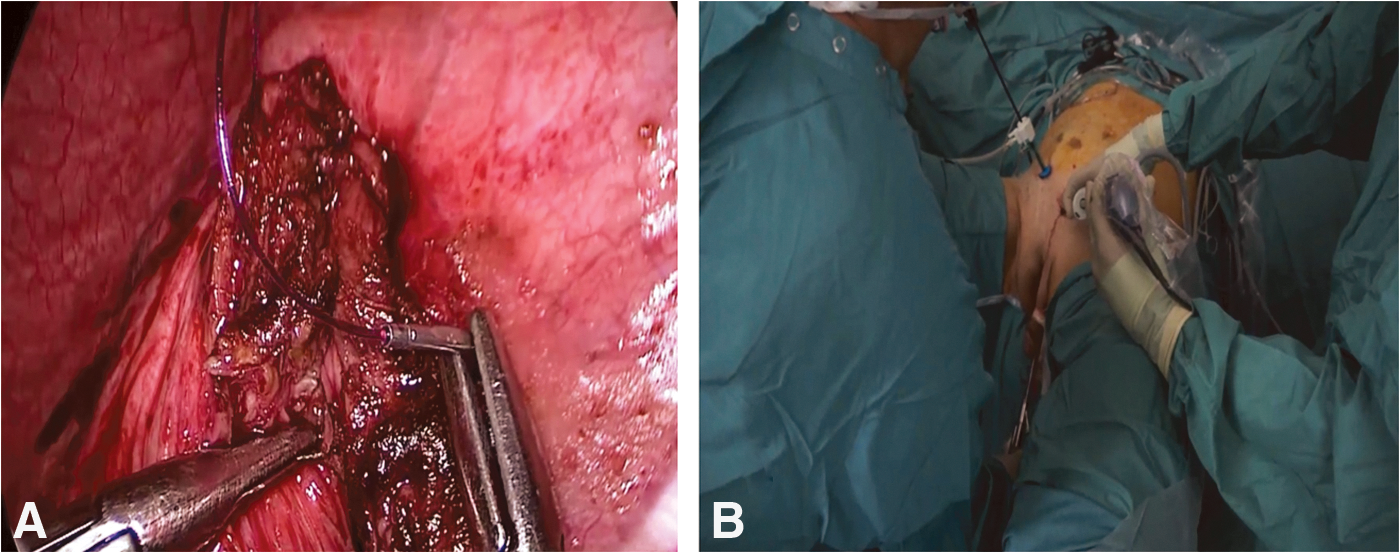
• Insertion of the laparoscopic needle holder through the urethra (NOTES assisted) to suture the bladder wall in one layer (Figs. 5 and 6). This provides a more optimal direction of the needle holder for suturing of the bladder wall because it is parallel to the trigone and posterolateral walls, where most diverticula are located. This renders this step easier than suturing the bladder wall through the transvesical laparoscopic ports (Fig. 8).
• Placement of LAPRA-TY® (Ethicon) after complete watertight closure of the bladder wall through the camera 10-mm port guided by the cystoscopic optic through the 5-mm port.
• Insertion of urethral catheter.
• Closure of the laparoscopic ports in layers, that is, muscle, subcutaneous tissue, and skin.
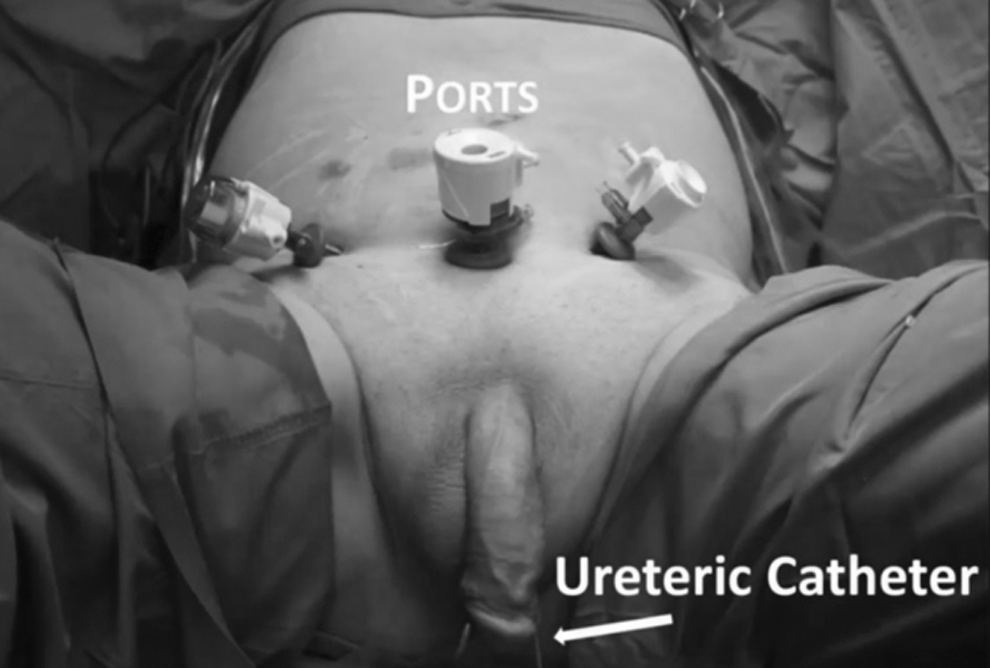
Trocar configuration. Trocars are inserted into the bladder in a flat triangular pattern.
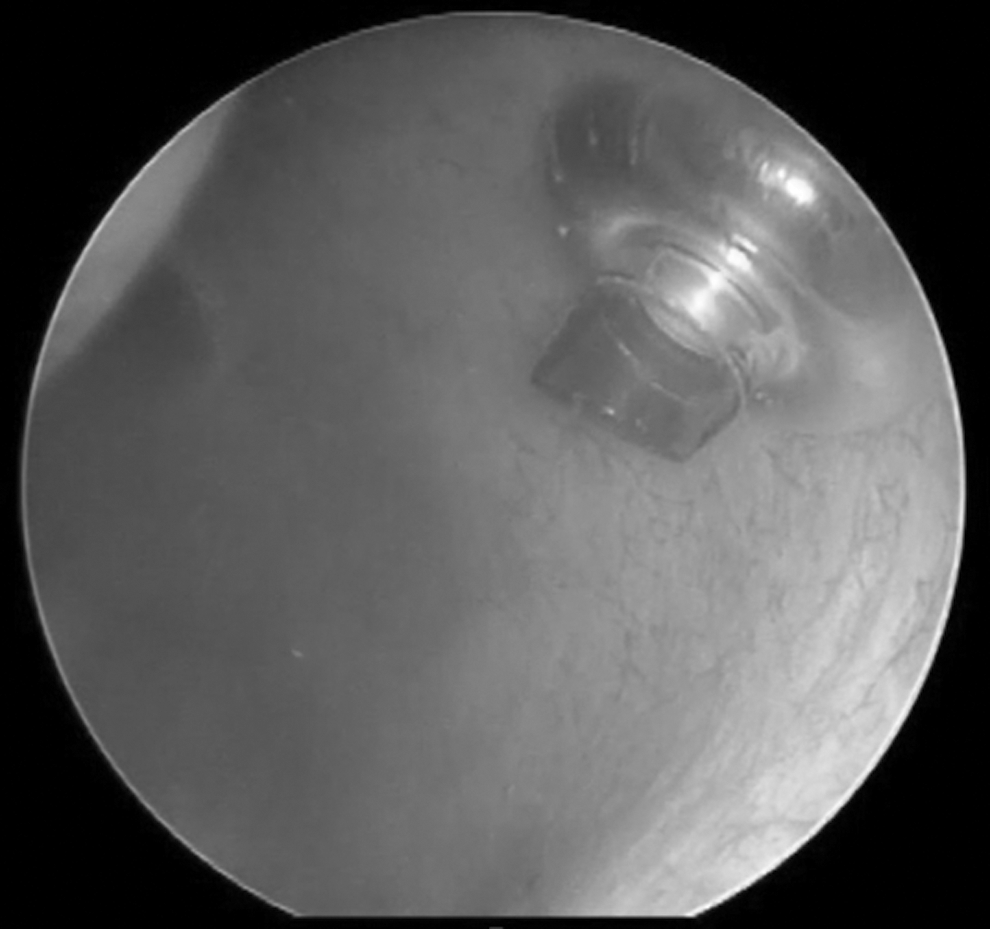
Cystoscopic view. Insertion of self-retentive trocars in the bladder under cystoscopic guidance.

Laparoscopic view. Circumferential incision of the bladder wall mucosa at the mouth of the diverticulum using monopolar scissors.
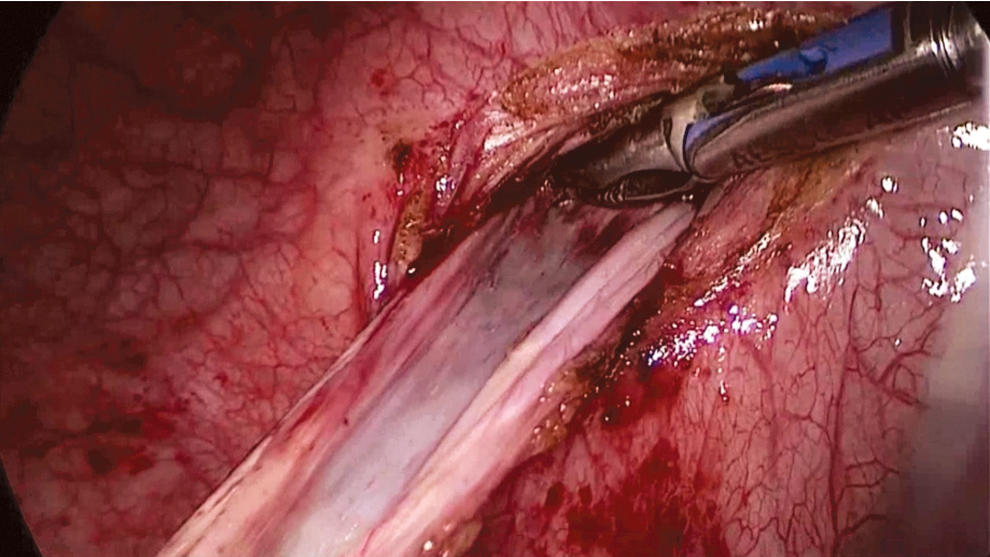
Laparoscopic view. Stripping of the diverticular mucosa from the detrusor muscle attachments using blunt and sharp dissection.
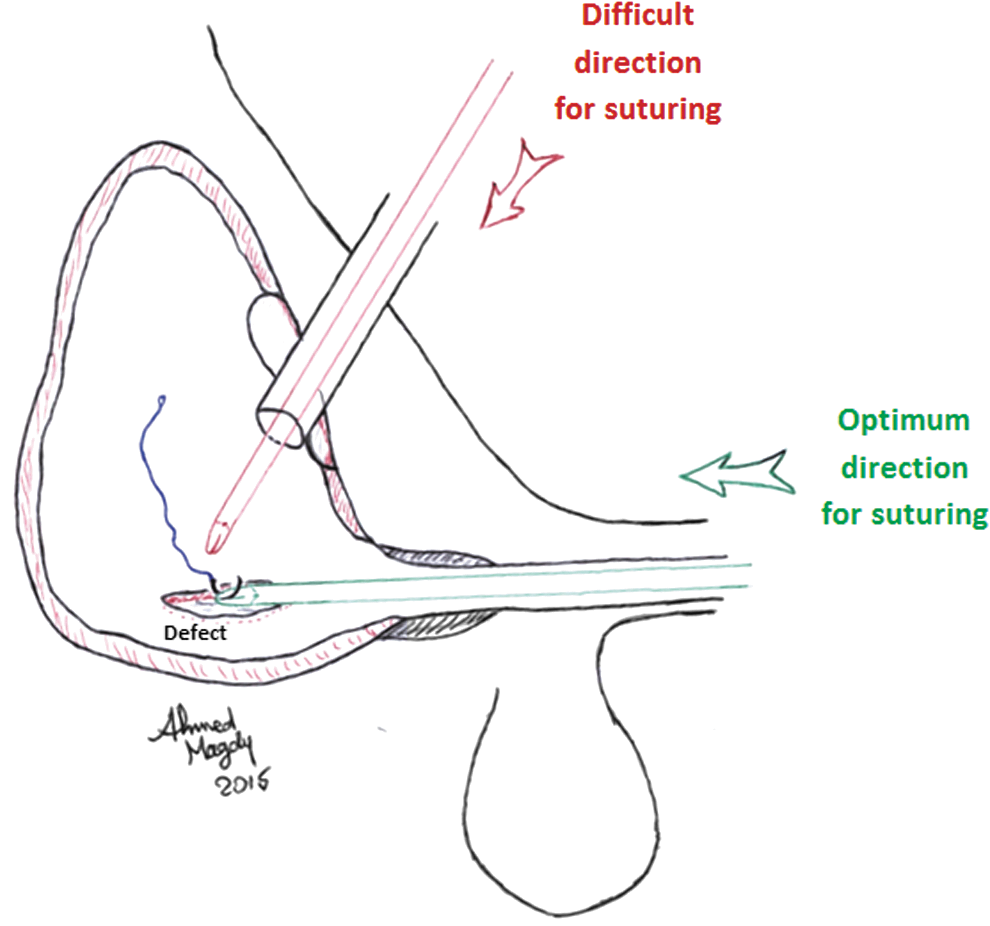
Illustrative diagram showing the advantage of our new concept from the ergonomic point of view, where suturing through the urethra offers an optimum direction of the needle holder in line with the defect.
We used 30°cystoscopic and laparoscopic optics (STORZ®), standard monopolar scissors, bipolar graspers, and a normal laparoscopic needle holder throughout the procedure with no need for sophisticated or special operative armamentarium. No leak of gas was noticed during manipulation of graspers or needle holder through the urethra.
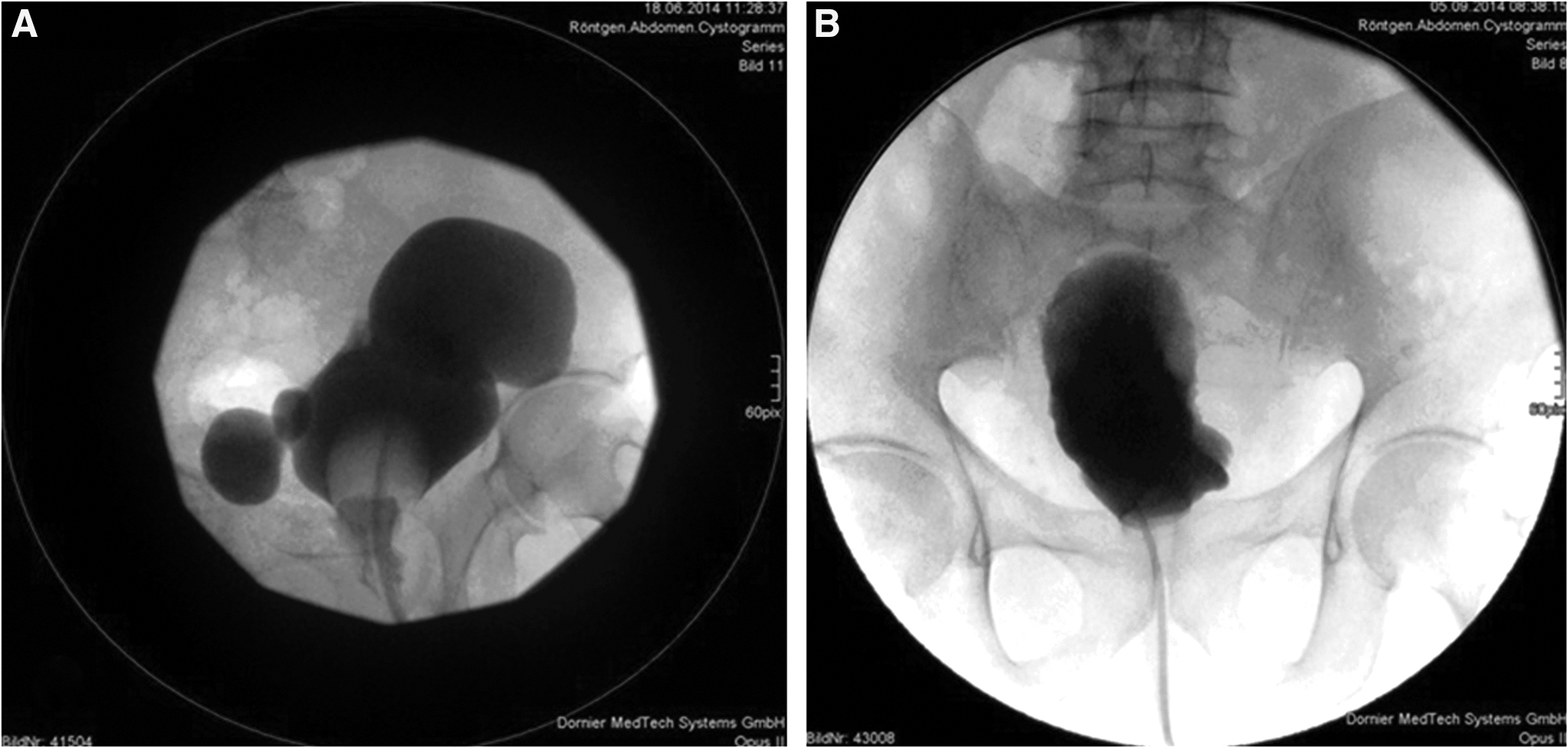
Retrograde cystogram with postvoiding film was performed on the 10th day postoperatively in all patients to test watertight healing of the bladder and ensure complete excision of the diverticula with no residual urine (Fig. 7). The patients were discharged after removal of urethral catheter and followed up for 1 year postoperatively.
Results
In four patients, eight diverticula were excised using the NOTES-assisted laparoscopic transvesical technique. All our patients were male. The mean age of the patients was 71.7 years. Success was determined as the subjective relief of the aggravating symptoms and objective disappearance of the diverticula in postoperative retrograde urethrocystogram.
Operative time ranged from 83 to 179 minutes, with a mean operative time of 134.25 ± 44.92 minutes. Blood loss was minimal in all cases (<50 mL). Mean excised diverticular size was 4.4 ± 1.83 cm. Urine after the operation was blood tinged with no need for bladder irrigation. No suprapubic catheter or drain was placed, and the bladder wall was not closed at the port site but was left to heal on the urethral catheter applying the same principle of the extravesical bladder tear.
One case had a grade IIIa complication according to the Clavien–Dindo classification of surgical complications 14 in the form of hydronephrosis on the right side with consecutive loin pain that necessitated intervention in the form of temporary percutaneous nephrostomy (PCN) under local anesthesia. In this patient, two right paraureteral diverticula were excised near the intramural ureter and right orifice. When we removed the right ureteral catheter immediately following the operation, edema likely formed around the orifice and intramural ureter, which led to the temporary obstruction of urine outflow at this side, thereby necessitating relief using a PCN. The patient was given analgesics and antiedematous treatment in the form of α-chymotrypsin, and the PCN was removed without subsequent problems after 3 days. We recommend leaving the ureteral stent in case of paraureteral diverticulectomy for at least 48 hours after the procedure to avoid this complication.
A mean patient follow-up of 11.6 months showed a good outcome with no medium-term complications, for example, urethral stricture or reported recurrence. The mean postvoid residual (PVR) urine has decreased by 116.25 mL. Detailed outcomes of the procedure are listed in Table 2.
Grade IIIa according to the Clavien–Dindo classification of surgical complications.
Discussion
Bladder diverticula are usually asymptomatic with no significant morbidity. However, some cases mandate intervention due to recurrent or unresolved urinary tract infection, hematuria, stones, and/or tumors inside the diverticula. Under rare circumstances, the diverticula may rupture and cause acute abdomen. 15
The treatment of secondary diverticula must follow the management of the primary cause. 16 The primary cause is usually a bladder outlet obstruction in the form of bladder neck contracture, benign prostatic enlargement, urethral stricture or, in rare cases, neglected long-term meatal stenosis. 1 A recent study described the combined laparoscopic management of bladder diverticula together with photoselective vaporization of prostate in the same setting; in this scenario, 1 of 14 patients (7.14%) required TUR incision after 1 year. 17 Another earlier study described simultaneous holmium LASER enucleation of the prostate with laparoscopic diverticulectomy but with a relatively longer operative time. 18 We preferred to perform both procedures in two different sessions with a mean interval of 94 ± 5.47 days to ensure that there was no need for a second intervention for the primary cause and to not disturb the surgical field in the primary intervention. We performed uroflowmetry for all cases included in this study before diverticulectomy, with a mean flow rate of 17.27 ± 1.65 mL/second.
In our patients, we used our new NOTES-assisted laparoscopic transvesical approach. Depending on the fact that most of the diverticula are located at posterolateral or paraureteral sites, insertion of the needle holder through the urethra offers (from an ergonomic point of view) a more optimal angle for closure of the bladder wall. The other alternative is to suture the bladder through articulated instruments, which has a longer learning curve to master and more challenges, especially in a small working space (as reported by Roslan and colleagues 1 ). Mechanically articulated instruments, such as Dextrité®, can also be used. However, these have the same drawbacks in addition to mechanical failure and the need for larger ports to drive them in. Notably, we used a normal laparoscopic needle holder with a relatively blunt tip. This together with ample urethral lubrication with gel are protective measures against iatrogenic urethral injury and subsequent urethral stricture.
In the first two cases, we applied a penile band to clamp the urethra and prevent gas leakage. However, we reported no gas leaks from the urethra during the procedure without this band. This matches the results of Roslan and colleagues. 16
The maximum number of excised diverticula in a single patient was 3. Our mean operative time was 134.25 ± 44.92 minutes (range: 83–179) compared with 256 and 216 minutes for a standard laparoscopic transperitoneal procedure performed by Abdel-Hakim and colleagues 4 and Moore and colleagues, 19 respectively. This is also less compared with the T-LESS technique, which was 256 minutes, and this is due to the small working space and coalition of the instruments, as argued by Roslan and colleagues. 1 This finding clearly demonstrates the advantage of our new technique, which helps minimize the operative time.
In our series, blood loss was minimal in all cases (≤50 mL). This matches most of the results published for other laparoscopic techniques. 1,4,13
We were able to completely and safely excise diverticula with a size up to 7 cm, with a mean size of 4.4 ± 1.83 cm, whereas the mean size of robot-assisted technique was 8.3 ± 3.6 cm. 20 Still we cannot state that this is a limitation of our technique as we performed the procedure in all presented cases to our clinic without selection.
We had no cases of inadvertent bowel injury. The trocars are inserted into a full bladder with saline applying the same principle of inserting a suprapubic catheter. A full bladder comes in direct contact with anterior abdominal wall and pushes the peritoneum backward, that is, away from the abdominal wall and upward rendering the procedure safe, unless there were bowel adhesions due to previous abdominal operation or history of pelvis irradiation.
One aspect of the technique involves asking the anesthetist not to bring the patient into a state of diuresis. The accumulation of urine frequently into the surgical field requires frequent suction, which adds to the operation duration, especially if the diverticula are located in a paraureteral position.
The hospital stay in our series was 10 days as a standard in our center; this nearly matches the results of Abdel-Hakim and colleagues 4 and Tareen and colleagues, 21 in which the hospital stay ranged from 7 to 14 and 5 to 14 days, respectively. This is because we performed retrograde cystography (RGC) in our patients before discharge. However, Roslan and colleagues 1 removed the catheter at 4 to 7 days and even stated that it can be minimized as few as 2 days without performing a postoperative RGC.
We performed a medium-term follow-up of 11.6 months. We scheduled the patients for follow-ups at 6 weeks and 1 year after the procedure. We performed transabdominal ultrasonography to check for PVR urine and the recurrence of diverticulum. The average PVR volume was 31.25 ± 6.29 mL. There were no reported recurrences or reported medium-term complications, for example, urethral stricture, in our small case series.
A point of technique is that this technique may be difficult to apply in domal and anterior wall diverticula, which are not common sites. In these cases, we recommend laparoscopic or LESS transperitoneal approach.
Conclusion
NOTES-assisted laparoscopic transvesical bladder diverticulectomy is a promising and safe procedure with good outcome. Using the urethra as an additional access to the bladder facilitates diverticular traction and bladder suturing with no need for extra ports and no reported technique-related complications on medium-term follow-up. This technique can also be applied together with the novel T-LESS approach.
Footnotes
Author Disclosure Statement
No competing financial interests exist.