
Abstract
Introduction:
Extracorporeal shockwave lithotripsy (SWL) has a low complication rate. While serious complications are rare, cardiac arrhythmias, such as ventricular tachycardia, may occur. The etiology of these arrhythmias is poorly understood, but it appears to be due to stimulation of the heart by the shock waves.
Objective:
This study examines the effect of rotating the patient 15° to 20° when an arrhythmia occurs.
Methods:
Eight hundred nineteen patients were prospectively evaluated for arrhythmias during SWL. The initial patient position was dependent on the location of the stone and the body mass index (BMI) of the patient. If a sustained arrhythmia developed, treatment was withheld for 2 minutes and then recommenced. If the patient developed an arrhythmia again, the patient was rotated 15°–20° away from the original position and treatment recommenced.
Results:
Twenty patients developed significant arrhythmias during SWL. Arrhythmias occurred more frequently in patients with a lower BMI (p < 0.01), of younger age (p = 0.01), and with right-sided stones (p = 0.035). After the first rotation, 11 patients had no further arrhythmias, and 4 patients had a reduction of their arrhythmia to unsustained minor arrhythmias that did not require cessation of the treatment. The remaining five patients required a second repositioning. Three of these patients required gated SWL to abolish the arrhythmia.
Conclusion:
Changing the position of the patient by rotating the patient by 15 to 20° can eliminate arrhythmias that develop during SWL.
Introduction
E
The mechanical and dynamic forces generated by the shock waves can cause trauma to thin-walled vessels in the kidneys and adjacent tissues. 2 These and other factors may lead to complications, such as perinephric hematoma, bacteremia, obstruction of the urinary tract by stone fragments, and cardiovascular complications. 4 Morbid cardiac events are rare, but the incidence of cardiac arrhythmias, such as unifocal premature ventricular contractions (PVCs), during SWL is not uncommon and ranges from 11% to 59%. 4,5 Although ungated SWL has been shown to be safe when simple monitoring rules are followed, gating of the shock waves to the electrocardiogram reduces the incidence of arrhythmia significantly. 6 –8
The etiology of these arrhythmias is poorly understood but appears to be due to a direct stimulation of the myocardium, which is related to the relative positions of the shockwave source, the stone, and the heart (Fig. 1). 8 –10 The idea of this study originated from the observation that some patients, who required repeated SWL for the same stone, may have an arrhythmia on one occasion and not another. It was therefore speculated that this might be related to a minor change in position between the two treatments. We hypothesized that by changing the position of the patient during the procedure, we could change the direction of the shockwave path, thereby altering its effect on the heart and reducing the incidence of cardiac arrhythmias. This study examines the effect of rotating the patient 15° to 20° from their original position each time an arrhythmia occurs during an SWL procedure.
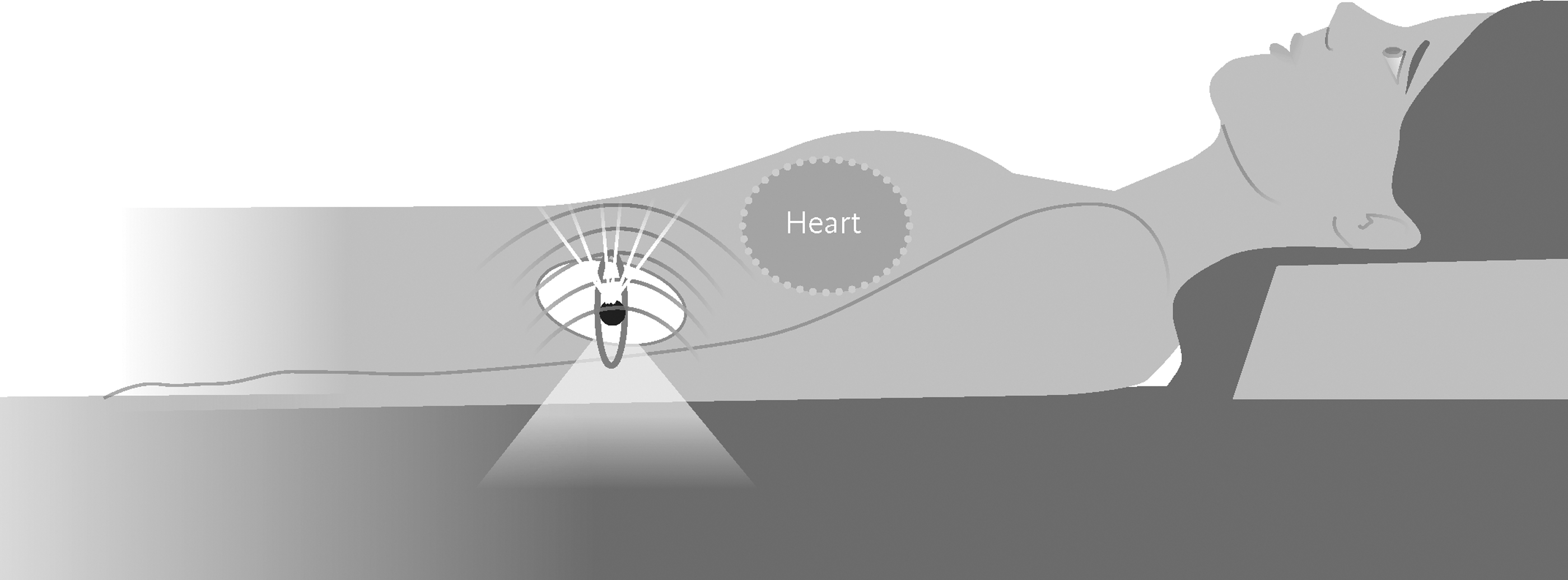
Shock waves proximity to the myocardium when treating kidney stones.
We did not expect this maneuver to replace cardiac gating, but we were hoping that this would add further information to our limited understanding of arrhythmias developing during SWL.
Materials and Methods
We prospectively evaluated 819 patients for arrhythmias during SWL on a Storz Modulith SLX-F2 electromagnetic lithotripter (Storz Medical AG, Tagerwillen, Switzerland) from January 2 to May 8, 2014. The patients were treated with as much as 3000 shocks at a rate of 120 shocks per minute and at an energy level of six. Energy ramping was routine, starting with an energy level of one and increasing that by one level every 125 shocks to the treatment level of six (power level 6 is midrange on the Storz Modulith SLX-F2 producing a peak positive pressure of 83.4 MPa at the F2 at this level). The treatment was performed under intravenous sedation using fentanyl 25 to 75 mg and propofol infusion, with a small amount of midazolam in younger patients, supervised by an anesthesiologist. The patients were attached to an ECG monitor and an oximeter. The initial patient position was dependent on the location of the stone and the body mass index (BMI) of the patient. Stones on either side may be treated with the patient in complete supine position. More frequently, however, especially with thinner patients, the patients were rotated about 15° to 20° with the side opposite to the stone elevated. This is the result of the patient position on the foil hammock, which tends to rotate the patient to some degree when the stone is positioned over the shock-head. With stones in the right kidney, the patient would be placed with the right side down over the shock-head in the right posterior oblique (RPO) position and for left-sided stones in the left posterior oblique (LPO) position.
If a sustained arrhythmia developed during SWL, treatment was withheld for 2 minutes and then recommenced. This was done to confirm that if the arrhythmia was controlled, it would be due to the patient rotation and not a short period without treatment allowing a normal rhythm to return. If the arrhythmia did return, when ESWL was restarted, as occurred in all 20 patients, the patient was rotated to the flat, RPO or LPO position depending on the initial position, in an attempt to prevent the arrhythmia by altering the trajectory of the SWL blast path, angling the shock wave away from the heart. For left-sided stones, the patient was rotated anticlockwise looking from the foot of the table from LPO to flat or from flat to RPO, and for right-sided stones, the patient was rotated clockwise from RPO to flat or from flat to LPO depending on the initial position (Fig. 2). If the patient continued to have a sustained arrhythmia, they were further repositioned into the third of the three possible positions. After two attempts of repositioning, if the arrhythmia continued, the patient was gated for the remaining of the treatment. The treatment was continued on all patients until complete fragmentation had been obtained or to a maximum of 3000 shocks.
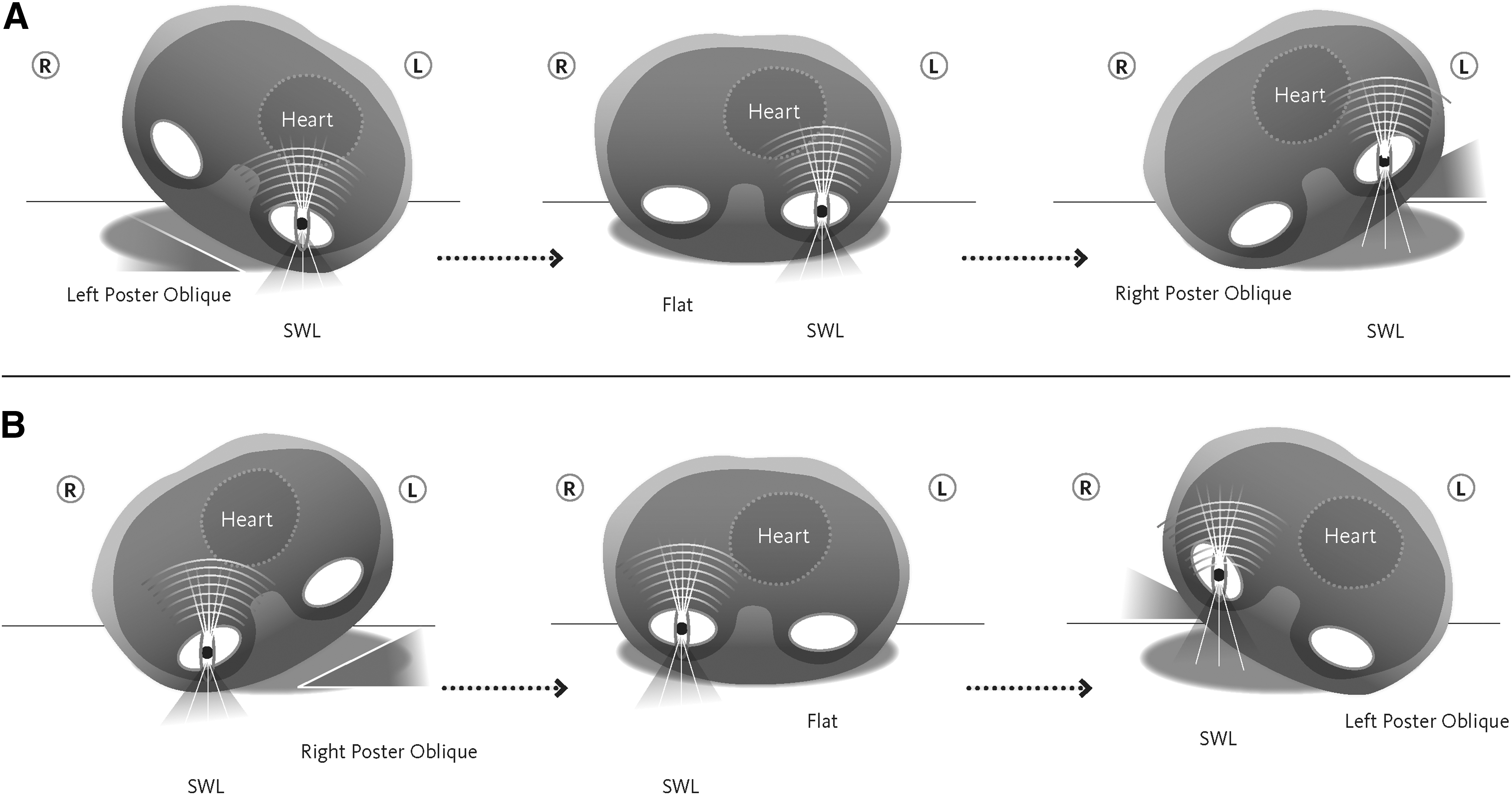
Patient positioning during SWL.
Patients' demographics, including age, gender, height, and weight, were collected. Treatment information and outcomes were collected, including the energy level, number of shocks administered, success, and whether or not the arrhythmia was controlled by changing the position. All statistical analyses were performed using SPSS 22.0 software. A two-tailed p-value <0.05 was used for statistical significance. Categorical variables were analyzed using Pearson's chi-square test. ANOVA was used to compare the means of continuous variable.
Results
Of the 819 patients studied, 20 patients (2.4%) developed significant arrhythmias during SWL. The arrhythmia was mainly in the form of ventricular tachycardia (V-tach) in 12 patients, sustained PVCs in 4 patients, and 4 patients had both. Arrhythmias occurred more frequently in patients with a lower BMI (p < 0.01), of younger age (p = 0.01), and with right-sided stones (p = 0.035). Although younger patients had a lower BMI, both BMI and age were independently significant. Of the 20 patients with significant arrhythmias, 16 patients had renal stones (6 upper pole, 4 interpolar, 4 lower pole, and 2 renal pelvis) and 4 had right-sided upper ureteral stone. No arrhythmias were seen when treating interpolar and lower ureteral stones (Table 1). Two patients had a cardiac history: one had incomplete RBBB (right bundle branch block), and the other had a history of ischemic heart disease and placement of coronary artery stents. The onset of the arrhythmia was unpredictable. In some patients, it appeared with the initiation of treatment (within 150 shocks), while in others, it occurred at various intervals during treatment. Seventeen of the 20 arrhythmias appeared at the maximum energy level of six, whereas the other 3 arrhythmias appeared at energy levels 2, 3, and 4.
Bold is to show that these are significant (< 0.05).
BMI = body mass index.
When a significant arrhythmia developed, treatment was stopped and held for 2 minutes. Treatment was then recommenced at energy level 2 and ramped as much as 6. The arrhythmia again developed in all patients. After the first rotation, 11 patients had no further arrhythmias (including the two patients with cardiac history), and 4 patients had occasional, unsustained, and hemodynamically insignificant arrhythmias that did not require cessation of the treatment. The remaining five patients required a second repositioning. In two of these patients, the arrhythmia was controlled, but three of these required conversion to ECG-gated SWL to abolish the arrhythmia (Table 2). In total, no further arrhythmias were seen in 11 of the 20 patients after repositioning. Gated SWL was only required in 3 of the 20 patients after changing the position a second time.
Arr = arrhythmia; PVC = premature ventricular contraction; V-tach = ventricular tachycardia.
Discussion
The pathophysiological basis of cardiac arrhythmias during SWL is still unclear after more than 30 years of SWL. Among the various hypotheses put forward to explain this phenomenon, two are most often quoted: direct mechanical stimulation of the heart and a neurohumoral response to the treatment or both. 11 Delius and colleagues induced cardiac arrhythmias in piglet hearts by focusing shock waves at the apex of the heart and found that the probability of arrhythmia was significantly decreased as the focus of shock wave was moved away from the heart. 12 Previous studies on SWL-induced cardiac arrhythmias examined various variables that can lead to the development of arrhythmias but failed to explain the relationship between the variables. Zanetti and colleagues demonstrated no correlation between cardiac arrhythmia and the side treated, the number or strength of the shock waves, or the administration of analgesics. 5 Greenstein and colleagues found that arrhythmias were more frequent during SWL to the right side but did not find any correlation with patient's age, gender, presence of heart disease, mode of anesthesia, or number of shock waves. 8 A more recent study by Skinner and Norman demonstrated similar findings, but as in this study, they also found that cardiac dysrhythmias occurred more frequently in younger patients. 11
In 1989, Ector and colleagues hypothesized that cardiac arrhythmias are developed by the direct pressure stimulation of the myocardium. 13 This hypothesis was supported by Greenstein and colleagues and Skinner and Norman, who found that patients treated for right-sided renal stones are more likely to develop cardiac arrhythmias than those with left-sided ones. 8,11 They suggested that this was because the shock-head was angled, directing the shock waves toward the heart. We also found that arrhythmias were more common when treating right-sided stones, but the shock-head on the Storz Modulith SLX-F2 lithotripter faces directly anteriorly. With right-sided stones, however, some of the patients are positioned at an angle (RPO), directing the shock wave toward to the heart. In contrast, 60% of the patients were positioned flat. This would suggest that reflected shock waves may be important and that the right side of the heart is more sensitive to this stimulation than the left, despite the fact that the heart remains within the low-pressure areas of the shockwave (SW) pressure field during patient positioning and that pressure changes at the heart would likely be subtle.
It has been shown that arrhythmias are more common with renal stones compared with ureteral stones. 6,9 We observed a similar finding in our study, and even though nonsignificant, the incidence of arrhythmias was higher in renal stones than in upper ureteral stones. No arrhythmias occurred when treating stones in the interpolar and lower ureter. These findings do suggest that proximity to the heart is associated with an increased incidence of cardiac arrhythmias.
All these findings do suggest that the direction of the shock wave is important in the development of arrhythmias during SWL and that changing the position of the patient changes the axis of the shock wave. This may change the direct or reflected pressure stimulation of the heart and thereby reduce the incidence of arrhythmias. Rotating the patient 15° to 20° from the original position, directing the shock wave away from the heart, reduced the incidence of cardiac arrhythmias.
Similar to Skinner and Norman, we found that arrhythmias were more common in younger patients, but we also observed that the arrhythmias were significantly more frequent in patients with a lower BMI. Since arrhythmias are thought to be due to stimulation of the myocardium, we suggest that patients with a higher BMI do not only have an increased skin-to-stone distance but also have a longer path from the shock-head to the heart.
If a patient develops arrhythmia during the procedure, the current recommended protocol is to change the procedure from ungated to ECG-gated lithotripsy to prevent the development of morbid arrhythmias. This is the first study to demonstrate that rotating the patient slightly during SWL prevents arrhythmia in the majority of instances, obviating the need for ECG gating. This adds to our understanding of the factors involved with the development of arrhythmia during SWL, but the practical application of this technique may be limited. From an academic perspective, our finding supports the mechanical origin of arrhythmia in SWL rather than the neurohumoral hypothesis.
All patients in this study were treated with a shockwave rate of 120 shocks per minute, which is not an optimal treatment rate. Research in our unit and others has demonstrated improved results with a slower shock rate, especially with larger stones. 14 –16 Treatment at a slower rate might probably also lower the risk of developing arrhythmias, but there is a current lack of evidence in the literature to support this. However, in our publicly funded healthcare system, there is a limited access to SWL and long wait times for treatment. With wait times of more than 3 months for renal stones and only three lithotripsy centers to service a population of more than 13 million people in the Province of Ontario, until we gain approval for a second lithotripter to run in parallel, we are only able to treat a limited number of patients with a slower rate (e.g., those with large stones or who have failed prior SWL treatment) without extending wait time significantly.
Conclusions
Changing the position, by rotating the patient by 15° to 20°, can eliminate arrhythmias that develop during SWL. This is the first study to demonstrate this effect and adds useful information to our limited understanding of this phenomenon.
Footnotes
Author Disclosure Statement
No competing financial interests exist.