
Abstract
Introduction:
In patients with normal estimated renal function before robot-assisted partial nephrectomy (RPN), there is still a risk for de Novo chronic kidney disease (CKD). We assessed the role of dipstick spot proteinuria in risk stratifying patients for CKD progression.
Materials and Methods:
From our prospectively maintained, institutional review board-approved database of patients undergoing RPN, we queried those with estimated glomerular filtration rate (eGFR) >60 and bilateral functional units. We assessed proteinuria through dipstick (trace or above) on voided urine in preoperative urologic appointment <3 weeks before RPN. Proteinuric patients were compared with the remainder of the cohort with parametric comparisons for continuous and chi-squared analysis for categoric variables. Multivariate logistic regression analyses were performed assessing the risk of de Novo CKD stage III development, estimated by the CKD-EPI equation.
Results:
We found 269 patients with eGFR >60 preoperatively, of whom 57 (21%) had proteinuria preoperatively. In univariate analysis, these patients were more likely to be diabetic (p = 0.023) and to be on an angiotensin converting enzyme inhibitor or angiotensin receptor blocker (p = 0.001) but had similar age (p = 0.13), body mass index (p = 0.09), and tumor size (p = 0.56) with similar rates of hypertension (p = 0.07). At a median 16 months, controlling for confounding variables, preoperative proteinuria on urinary dipstick was associated with a 2.3× (95% confidence interval 1.03–4.95) increased risk of de Novo CKD stage III progression.
Conclusions:
Patients with proteinuria preoperatively, despite a normal eGFR, likely have intrinsic medicorenal disease. These patients should be counseled preoperatively that they have a higher risk of CKD progression following RPN.
Introduction
R
Many authors have published articles and recommended techniques for assessing renal function and risk factors for chronic kidney disease (CKD) progression following the procedure. 6 –8 However, despite modification of surgical technique, characteristics intrinsic to the patient or the tumor continue to be the main drivers of renal functional outcomes postoperatively. This is particularly difficult in assessing patients with presumed normal renal function preoperatively (estimated glomerular filtration rate [eGFR] >60). 9
We therefore sought to assess other parameters to determine which patients in this subset harbor risk factors for renal functional decline. The purpose of this study was to assess whether or not preoperative urine protein (as quantified on preoperative dipstick test performed in clinic) could predict renal functional outcomes of patients with eGFR >60 undergoing RPN, independent of confounding variables.
Methods
Using a prospectively maintained institutional review board-approved database of all patients undergoing RPN by a single surgeon, we identified all patients with two functional renal units and a preoperative eGFR >60 as determined by the CKD-EPI equation. These patients were included in further analyses. All procedures were performed by a single surgeon (A.K.H.) using the daVinci Surgical System (Intuitive Surgical, Mountain View, CA). Residents or fellows participated in all procedures, with increasing involvement based on the level of training.
Before the procedure, all patients underwent preoperative cross-sectional imaging with either CT or MRI to evaluate tumor size and location. The RENAL nephrometry score was calculated by a single individual for all masses, as was the determination of the endo/exophytic component of the mass. Patient and tumor baseline characteristics as well as all additional follow-up data points were prospectively recorded into our database. Our surgical technique has been highlighted in previous articles. 10 –12 Briefly, we placed all patients in a lateral position with abdominal insufflation pressure of 15 mm Hg, which is decreased at the conclusion of the procedure to ensure hemostasis. Excision of the mass is performed with cold robotic scissors. Decision on the need for arterial vascular occlusion at the time of surgical excision is determined at the time of the procedure by the attending physician and based on tumor- and patient-specific characteristics. Warm ischemia was minimized in all cases. All patients had general anesthesia performed by a member of the designated genitourinary anesthetic team. Only mild variations were observed among inspiratory pressures and ventilator settings, induction and maintenance anesthetic agents, and postanesthesia care unit medications.
Proteinuria was measured as per protocol on voided urine dipstick measured in all patients at the preoperative clinic appointment. Confirmatory testing or quantification of proteinuria was not routinely performed. Patients with trace or greater proteinuria were included as proteinuric patients. Patients with active urinary tract infection at the time of urine dipstick were excluded from the analysis. We noted comorbidities for patients and included in analysis if they required pharmacologic therapy for treatment of disease (chronic obstructive pulmonary disease, diabetes mellitus, hypertension [HTN]) or in the case of coronary artery disease, if they had required previous invasive procedure for treatment of this disease. We noted perioperative and postoperative usage of either an angiotensin converting enzyme inhibitor (ACEi) or angiotensin receptor blocker (ARB) and included these in analyses. We routinely follow patients postoperatively with radiologic imaging of the chest and abdomen and serum creatinine calculation. Risk for CKD progression was based on serum creatinine measurement >30 days following the initial surgical procedure.
Statistical analyses
We analyzed demographic and perioperative data using descriptive statistics. We expressed categoric variables in frequencies and percentages and continuous variables as mean with standard deviation. Differences were calculated with the chi-squared test for categoric variables or Student's t test for continuous variables.
We performed univariate and multivariate Cox proportional hazard regression analysis to determine the variables associated with the development of de Novo CKD stage III or greater. All variables with a p-value of 0.05 or less were included in the multivariate analysis. We demonstrated the Kaplan–Meier estimate for risk of de Novo CKD development between proteinuric and nonproteinuric patients. We used a two-sided p-value of <0.05 for statistical significance in all analyses. We used JMP 11.0 (Cary, NC) to perform all analyses.
Results
Of 381 consecutive patients undergoing RPN at our institution between March 2009 and August 2014, we noted 269 with eGFRs >60 and with a preoperative urine dipstick measured within 4 weeks of their procedure. Overall, 57 (21%) of patients had urine dipstick positive for proteinuria. Of proteinuric patients, 33 (58%) had traces, 16 (28%) had 1+, 7 (12%) with 2+, and 1 (2%) patient with 3+ urinary protein. For further analysis, we included all proteinuric patients as a single subset.
Table 1 highlights the difference between proteinuric and nonproteinuric patients. Notably, these patients had increased risks of all comorbidities, but only diagnosis of diabetes (p = 0.02) reached a statistical significance. These patients were much more likely to be on an ACEi or ARB (p = 0.008). There were similar rates of hilar clamping at the time of tumor excision, but when clamped, proteinuric patients had about four fewer minutes of warm ischemia (p = 0.007). The mean preoperative eGFR was slightly lower in the proteinuric patients (85 vs 90, p = 0.02).
ACEi = angiotensin converting enzyme inhibitor; ARB = angiotensin receptor blocker; eGFR = estimated glomerular filtration rate.
Among 215 patients with >30 days of follow-up for their renal function, we assessed the long-term risk of developing de Novo CKD stage III or above. We noted that only 40 (19%) of patients were diagnosed with new onset of CKD stage III (Table 2). Using a Kaplan–Meier estimation, we found that proteinuria patients had a higher rate of eGFR decline than those without proteinuria (p = 0.02) (Fig. 1). Subset analysis of patients with CKD stage I (eGFR >90) or CKD stage II (eGFR >60, <90) found that proteinuria was not independently associated with CKD progression (log-rank 0.18, 0.27, respectively). We compared patients with trace proteinuria to those with the 1+, 2+, or 3+ proteinuria noted on dipstick and found no difference between these subsets (log-rank, p = 0.91).
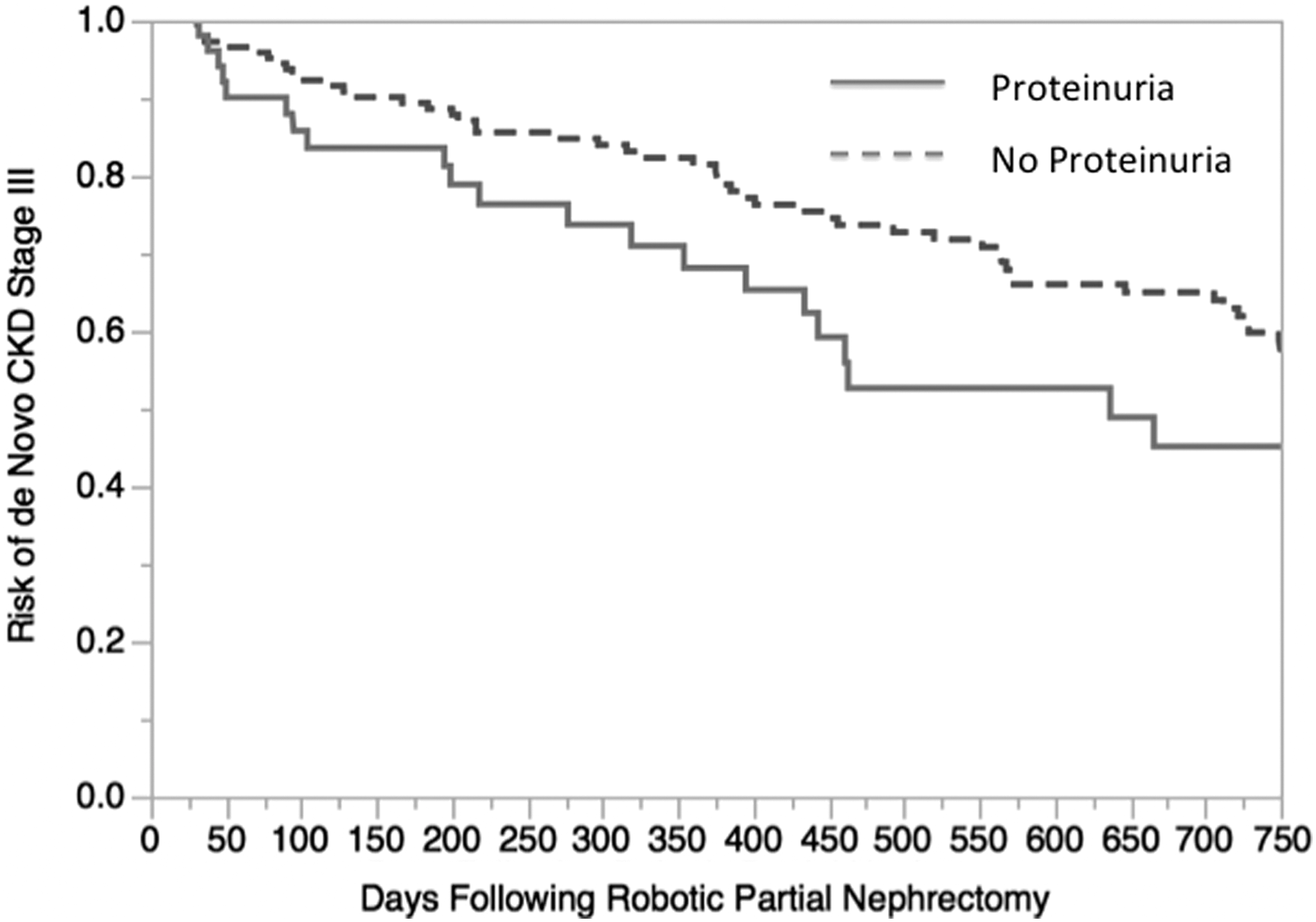
Risk of development of de novo CKD Stage III or above in patients with urinary dipstick for patient with presumed normal renal function with or without proteinuria (log-rank p = 0.02). CKD, chronic kidney disease.
CI = confidence interval; CT = computed tomography; OR = odds ratio.
We subsequently performed a Cox proportion hazard assessment to determine individual variables associated with CKD progression. On the univariate analysis, we identified multiple variables associated with de Novo CKD stage III progression. These included all comorbidities assessed and the utilization of ARB/ACEi. On multivariate analysis, the factors remaining statistically significant as increased risk for long-term CKD progression included history of coronary artery disease and proteinuria. Elevated body mass index and increased preoperative eGFR were protective of CKD progression.
Neither the performance of a clamped procedure (odds ratio [OR] 1.54, 95% confidence interval [CI 0.54–6.50]) nor the duration of warm ischemia (OR 0.98 per minute, 95% CI [0.94–1.03]) was associated with CKD progression. Subset analysis of clamping technique did not impact the proteinuric patients and long-term risk of CKD progression (p = 0.21).
Discussion
In this article, we chose to only assess patients with eGFR >60 as measured by CKD-EPI. This subset of patients is typically considered to have normal renal function, as has been outlined in several previous urologic publications. 13 Kumar et al. noted that following RPN, patients with eGFR >60 before surgery had a 33% risk of progression to CKD stage III or greater at 12 months following the procedure. 9 A similar comparison by Guillotreau et al. demonstrated that in their cohort, 36% of the patients with eGFR >60 preoperatively had CKD progression following RPN at 3 months postoperatively. 14 Perhaps we and other cohorts have noted a substantial rate of CKD progression because we are incompletely characterizing eGFR >60 patients as having normal renal function preoperatively. A substantial cohort of these patients, in fact, have proteinuria noted on their preoperative urinalysis, demonstrating intrinsic renal disease previously unaccounted for.
Despite eGFR measurements indicating these patients had normal renal function, it is unlikely they had normal filtration. Proteinuria is a sign of early renal dysfunction, even in patients with normal measured renal function. The American College of Physicians (ACP) has adapted their definitions of CKD to include patients with eGFR >60 if there is evidence of kidney damage. These patients would qualify as either CKD stage I (if eGFR is >90) or CKD stage II (if eGFR is between 61 and 90). Therefore, all patients with proteinuria are by definition CKD patients and should likely be counseled before any surgical procedure. We note that in either subset of CKD stage I or CKD stage II, we did not find proteinuria to be independently predictive of CKD progression, but that is likely due to lack of statistical power.
Proteinuria was assessed as a single urinary dipstick measurement as per routine at the time of preoperative clinical assessment. The reagent used in measurement of proteinuria is bromophenol blue, which is highly sensitive for albumin. Several conditions can produce false-positive transient proteinuria, including congestive heart failure, dehydration, or even emotional stress or exercise. We did not include these potential confounding variables in our analysis, perhaps limiting the specificity of our classifications. In addition, we did not routinely quantify the extent of proteinuria following a positive detection. While we did note that the degree of proteinuria did not differentiate risk of CKD progression postoperatively, we believe that the sample size and collection technique limited our ability to detect this difference. In this comparison, we compared only 57 patients, and thus it is possible that, if not likely, with a larger sample size, we could establish a stronger comparative analysis in these subsets. In addition, spot urine proteinuria tests have trouble differentiating the exact amount of proteinuria and therefore likely do not place patients into subgroups with enough accuracy. 15
More accurate measurements of renal proteinuria may produce improvement in our sensitivity to predict changes in postoperative renal function. While the Kidney Disease Improving Global Outcomes guidelines recommendations include initial screening for proteinuria with an untimed urine specimen with automated reading, this is less preferable to either the urine albumin to creatinine ratio or the protein to creatinine ratio. 16 This helps to reduce variation seen in dilution of the automated proteinuria reading. However, even the untimed albumin to creatinine or protein to creatinine ratio may not reflect protein excretion variation due to stress, time of day, exertion, or other factors. Confirmatory 24-hour collection may be required in these situations. 17 Our current practice in the clinic has changed to include calculation of the protein to creatinine ratio with a hope that this can improve postoperative diagnostic accuracy of risk for renal functional decline.
We included the utilization of ACE/ARBi following the procedure. The ACP guidelines state strong recommendation for the usage of either an ACEi or an ARB in patients with HTN and stage I to III CKD. 18 While it appeared that this was independently associated with renal functional decline in the univariate analysis, the multivariate analysis demonstrated that this was an association with the other confounding variables rather than truly independent of renal functional outcomes.
While in patients with medically induced renal disease, CKD progression is predictive of long-term morbidity and mortality rate, the utilization of a threshold cutoff at eGFR of <60 may be an artificial assessment in this patient cohort. 19 Recent comparisons between surgically and medically induced renal disease demonstrate these might be separate disease entities. 20,21 While this proteinuria cohort demonstrates some degree of medically induced renal dysfunction, the risk of disease progression needs additional follow-up to assess for other endpoints, including cardiac morbidity or progression to dialysis.
Renal volume preservation has been demonstrated in several studies to predict functional outcomes, however, this was not assessed independently in this study due to limitations with imaging follow-up. 4,5 We therefore assessed renal quality, independently assessed with proteinuria. Proteinuria is a simple noninvasive test that is performed preoperatively to aid in risk assessment before surgical resection. We note that a history of coronary artery disease places the patient at a significantly increased risk of CKD progression. Likely due to global endothelial dysfunction and plaque formation, these patients are at risk for long-term renal ischemia and, therefore, renal dysfunction. 22 While elevated body mass index does appear to provide some degree of protection from renal decline in this cohort, the mechanism of this association is being investigated and will be the focus of future research.
There are several limitations inherent in this article. As a retrospective analysis of a prospectively maintained database, many limitations are noted in this study design. In addition, we do not have routine estimations of remaining renal volume. We also lack long-term estimation of renal function as noted by development of proteinuria in postoperative follow-up. We also are unable to estimate the number of patients who had resolution of proteinuria postoperatively. Estimation of glomerular filtration rate by the CKD-EPI equation, while typically effective, has its limitations. Assessment with renal scintigraphy before and after surgery was impractical in our patient population. As all patients had bilateral functional renal units in this study, we are unsure as to which kidney is responsible for the preoperative proteinuria. An additional limitation in these data is the median follow-up of only 16 months. Continued longitudinal assessments of renal function will be required to confirm these early findings. Future studies on this topic could evaluate whether the quantification of proteinuria improves prognosis.
Conclusions
Patients undergoing RPN with eGFR >60 might still harbor signs of renal dysfunction. Proteinuria is independently associated with increased risk for renal functional decline postoperatively. These patients should be counseled preoperatively that they run increased risk of CKD progression and may require closer follow-up.
Footnotes
Author Disclosure Statement
No competing financial interests exist.