
Abstract
Looking for a virtually “scarless” surgery mini-laparoscopy (ML) could be a viable alternative to conventional laparoscopy. ML is a reproducible technique and allows for the preservation of the triangulation concept, the cornerstone of laparoscopic surgery. Drawback of ML could be the poor performance of miniaturized instruments that could affect the confidence of the surgeon and limit the indications. The recent availability of a novel mini-laparoscopic platform in our center expanded the indications of ML to radical nephrectomy even in cases of large renal tumors in kidneys with abundant perirenal fat. The platform is composed by mini-instruments with the peculiarity of a 2.9-mm shaft that is mounted on a handle and a jaw that are comparable in size and performance to those of conventional instruments, increasing the ergonomy and the confidence perceived by the surgeon. Allowing for inclusion criteria, nine consecutive patients were enrolled in our prospective study and underwent percutaneously assisted “two-ports” radical nephrectomy. Preliminary data showed that the novel platform allowed us to perform a safe and effective procedure with acceptable perioperative outcomes and apparent improvements in cosmesis. Larger sample size and comparative studies are needed to confirm these findings.
Introduction
W
In the meanwhile, the new discovery of smaller instruments and the development of mini-scopes have renewed the interest about mini-laparoscopic surgery. 5 –7 The approach represents the most appealing minimally invasive approach due to the fact that it reduces the invasiveness of laparoscopy, in the meanwhile maintaining the triangulation concept, a cornerstone in laparoscopic surgery. On the other side, mini-laparoscopic approach is not devoid of limitations. The limitations are mostly represented by the poor image quality due to the use of miniaturized scopes and the poor performance and ergonomy of mini-instruments that can affect the confidence of the surgeon during the procedure.
If the first hot point is being overcome by the introduction of novel camera systems, 8 the second hot point is still a matter of debate.
Discussion of the Technology
In our center, we recently introduced a novel mini-laparoscopic platform (Percuvance™ System; Teleflex Medical Europe Ltd., Athlone, Ireland), aimed to change the philosophy of mini-laparoscopy.
The platform consists of modular instruments: the set includes standard sized handles, 2.9 mm shafts, and 5-mm jaws (Johanne's forceps and grasper). The key feature of these instruments is the way they are assembled: the handle is mounted to the 2.9 mm shaft, while preparing the armamentarium for the intervention. A dedicated tip is mounted at the end of the shaft. The shape of the tip is comparable to that of a Veress needle. The tip will allow for the percutaneous introduction of the instrument without the need of a port. Once the instrument is introduced, its tip is retrieved throughout the operative port: extracorporeally, the tip used for the percutaneous introduction of the instrument is exchanged with the 5-mm jaw of choice. At this point, the instrument is tested by grasping whatever (i.e., the finger of the surgeon) and then reintroduced inside the intracorporeal working space.
In the “two-ports” laparoscopic technique, one of these percutaneous instruments is used by the nondominant hand of the surgeon (usually with a Johanne's forceps jaw mounted); another instrument can be used for the management of the spleen or the liver, according to the surgeon's preference. By this technique, nine radical nephrectomies for renal tumor were performed by transperitoneal approach. Neither tumor size nor thickness of perirenal fat was a limitation for the approach (Fig. 1).
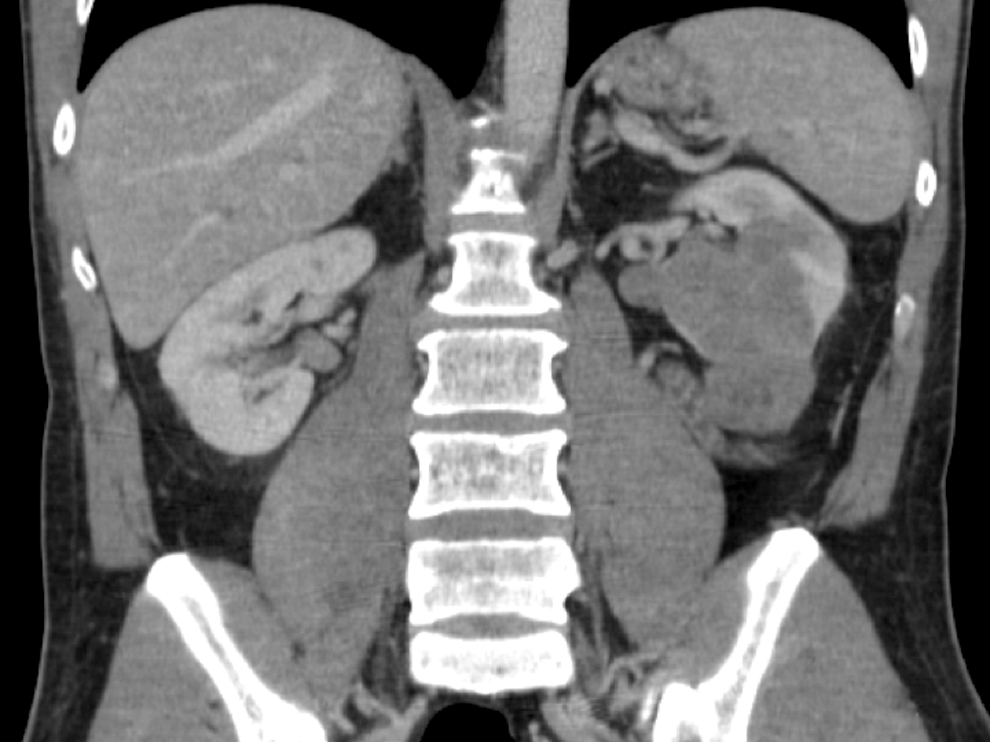
Computed Tomography scan (coronal view) of an operated kidney affected by an 8.5 cm lesion developing from the medium third of the kidney beyond the lower pole.
Over the purpose of the study, other indications of the novel platform of percutaneous instruments were the assistance during pure or robot-assisted laparoscopic procedures to allow for the grasping, the management of any anatomical structure if required, and during pure single-site approach to ensure the triangulation in case of challenging procedures.
The Role of the New Technology in Endourology: Initial Series
We report the initial series of nine patients who prospectively underwent percutaneously assisted “two-ports” radical nephrectomy for renal tumor. To collect a consecutive cohort allowing for inclusion criteria, all patients with renal tumors unsuitable for a nephron-sparing approach were included in the study. Enrolled patients had previously signed an informed consent.
Morbidly obese patients (body mass index ≥30) and/or who had previously undergone significant abdominal surgeries were excluded.
Results
Table 1 shows the demographic and preoperative data. Intraoperative and postoperative data and complications are reported in Table 2. Concerning the use of analgesic drugs, buprenorphine was stopped following the first postoperative day in all cases; no paracetamol vials were required following the postoperative day 1. Pathologic data are reported in Table 3.
ASA = American Association of Anesthesiologists; BMI = body mass index; CCI = Charlson Comorbidity Index; CT = computed tomography; Hb = hemoglobin; SD = standard deviation.
Skin-to-skin.
Including the day of the surgery.
EBL = estimated blood loss; Hb = hemoglobin; SD = standard deviation; WIT = warm ischemia time.
ccRCC = clear cell renal cell carcinoma; pRCC = papillary renal cell carcinoma; PSM = positive surgical margin.
Description of instruments
• Percuvance System (Teleflex Medical Europe Ltd.), a novel platform, including modular disposable components allowing for different instruments' configurations: the handles are mounted with a 2.9-mm shaft that is compatible with interchangeable 5 mm tips, which include graspers and Johanne's forceps.
The basic laparoscopic set was used in all cases, including the following: • Scope: Straight Forward Telescope 0°, enlarged view, 5 mm in diameter, and 25 cm in length. • Camera: SPIEs (Storz Professional Image Enhancement System; Karl Storz Endoskope, Tuttlingen, Germany). • Ports: 5 and 10 mm inner diameter, 10–15 cm in length (on the basis of the patient's). • 10 habitus mm clips applier (Hem-o-lok; Teleflex Medical Europe Ltd.). • 5-mm suction–irrigation cannula with two-way stopcock connector. • Scissors, serrated, curved, and conical, with irrigation connection for cleaning, and double-action jaws. • Bipolar coagulating forceps.
Optionally, other technologies (such as Ligasure or Thunderbeat) could be used according to the surgeon's preference.
Surgical technique
Gaining the retroperitoneum
The pneumoperitoneum was achieved by using a Veress needle. One 5 mm port was introduced above the belly button for the mini-scope. A 10 mm port for the right hand of the surgeon was inserted under endoscopic vision at the level of the pararectal line, caudally.
Assembly and introduction of Percuvance system
The handle was assembled with the shaft; the shaft was assembled with a dedicated tip for the percutaneous introduction (Fig. 2). The percutaneous access of the instrument was performed under laparoscopic view. The instrument was retrieved throughout the 10 mm port. Then the tip for percutaneous access was exchanged with the jaw of choice (usually the Johanne's forceps one). After testing the good holding of the assembled instrument, the instrument was introduced into the abdominal cavity and the procedure began (Fig. 3A–D).
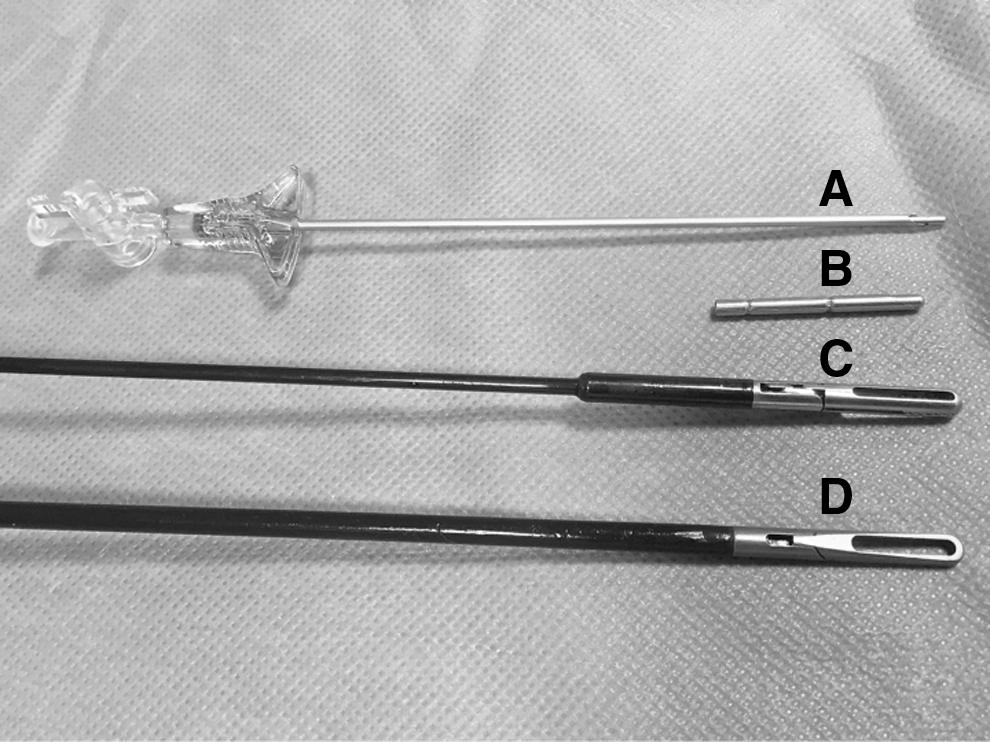
Comparison of outer diameters of the instruments.
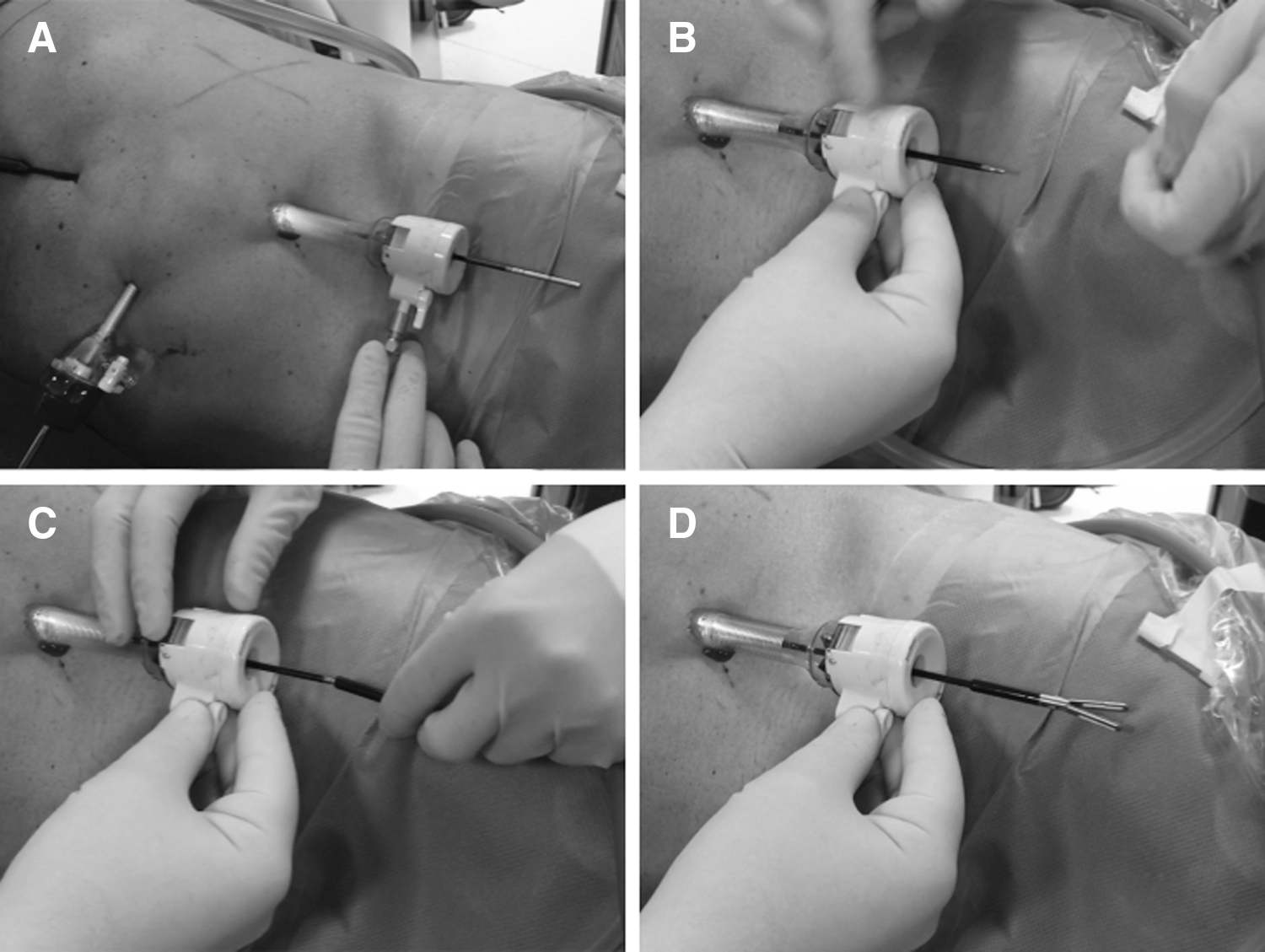
Assembling the Percuvance instrument. Following percutaneous introduction into the abdominal cavity,
Dissection of the renal pedicle, identification of the ureter and gonadal vein, and nephrectomy
The procedure was carried out according to the standard technique as previously described. 9 We underline that in the technique presented in this study, one Percuvance instrument was used for the management of the liver or the spleen for right-sided or left-sided procedures, respectively, without significant differences with respect to the standard approach. Another Percuvance instrument was used by the left hand of the surgeon, mounted with the Johanne's forceps jaw (Fig. 4). All the laparoscopic gestures performed were comparable to those of the standard laparoscopic approach. Specifically, dissection of perirenal fat and renal hylum was performed easily with good feeling perceived by the surgeon in terms of ergonomy and efficacy (Fig. 5).
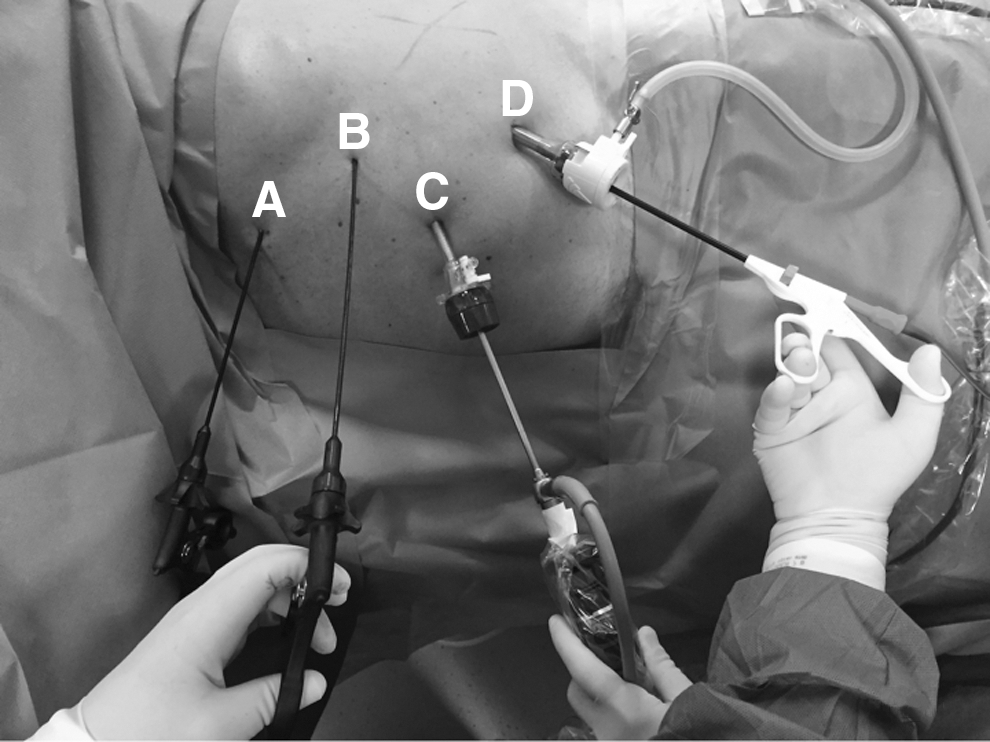
Configuration of the instruments during the procedure.

Intraoperative views showing Percuvance instruments in action.
Preliminary results showed that the novel platform allowed us to perform a safe and effective procedure with acceptable perioperative outcomes. No complications were recorded. All the procedures were completed without need of conversion to the standard laparoscopic approach.
Conclusion
In conclusion, the instruments of the novel platform represent a further evolution of conventional laparoscopy toward the minimization of the trauma related to the laparoscopic access. The use of these instruments can be considered a step forward in the improvement of the cosmetic results. We underline that this is possible without compromising the confidence of the surgeon during the operation and the safety of the procedure. On the basis of the size and the site of the incision for the specimen retrieval, the final result of “two-ports” technique can be similar to that of a single-site surgery: as we used this approach for radical nephrectomy, which requires a significant incision for specimen extraction, the scar for the operative trocar was elongated and used for specimen retrieval and the 5 mm scar for the optical port was used for the drainage, with all the mini-incisions for percutaneous instruments being almost negligible, comparable to that for the Veress needle or a skin mole (Fig. 6). Comparative studies are needed to test if the advantages in terms of cosmetic results are significant for the patients. The surgeon's feedback with the instruments should be tested in a standardized manner to find eventual differences with respect to the standard approach. We underline that our results were obtained by an experienced laparoscopic surgeon at the end of the learning curve for conventional laparoscopic radical nephrectomy. Consistent experience with laparoscopic surgery is mandatory before embarking with this kind of approach.
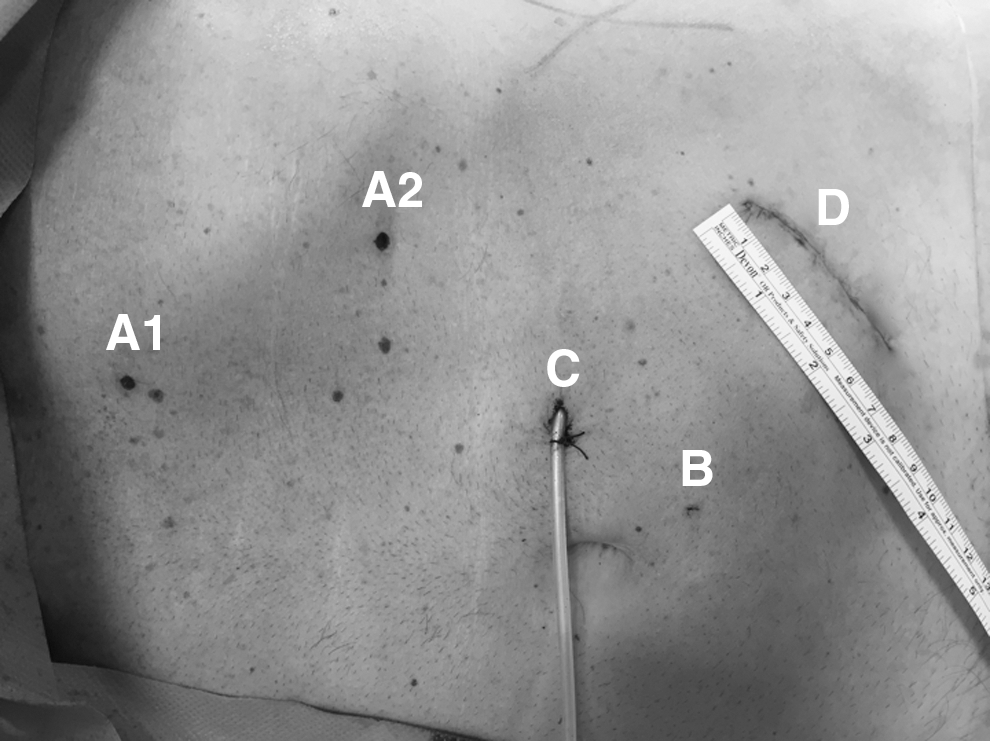
Final result.
Author Disclosure Statement
No competing financial interests exist.