
Abstract
Objectives:
To test if obesity predisposes to higher rates of adverse outcomes after percutaneous nephrolithotomy (PCNL).
Materials and Methods:
Within the Nationwide Inpatient Sample (NIS), we identified patients treated with PCNL between 1998 and 2010 for kidney stones. We examined the temporal trends in PCNL use and charges among obese and nonobese patients. We then tested the effect of obesity on perioperative complications, transfusions, length of stay (LOS), and total hospital charges (THCs). LOS and THCs were defined as a continuous variable and were also dichotomized according to the 75th percentile into prolonged LOS (pLOS) and increased THCs (iTHCs). Then, multivariable models were fitted.
Results:
Overall, a weighted sample of 90,529 individuals treated with PCNL between 1998 and 2010 was examined. Of those patients, 9300 were obese (10.3%). The proportion of PCNLs performed in obese patients increased throughout the years from 7.4% to 16.7% (p < 0.001). Overall complication rates were 21.6% vs 22.0% (p = 0.3) and transfusion rates were 4.3% vs 4.0% (p = 0.1) for obese and nonobese patients, respectively. Obese patients had fewer genitourinary complications (13.4% vs 15.0%, p < 0.001), but had higher rates of sepsis (1.7% vs 1.3%, p = 0.009) as well as respiratory (3.0% vs 2.5%, p = 0.002) and vascular complications (0.3% vs 0.2%, p = 0.007). Conversely, pLOS (20.9% vs 18.8%, p < 0.001) and iTHCs (30.8% vs 24.4%, p < 0.001) were more frequently recorded in obese patients. In multivariable analyses, obesity was neither associated with higher rates of overall complications (odds ratio [OR], p = 0.3) nor with higher rates of transfusions (p = 0.3). However, obesity was associated with pLOS (OR: 1.21, p = 0.002) as well as iTHCs (OR: 1.17, p = 0.002).
Conclusions:
PCNL in obese patients did not result in higher rates of individual complications or transfusions. However, it resulted in higher rates of pLOS and iTHCs.
Introduction
P
Materials and Methods
Study source
We relied on the NIS, which is an inpatient database that is representative of ∼20% of U.S. community hospitals, for the years 1998 to 2010. Discharges are then weighted to provide national estimates. 13
Study population
All diagnoses and procedures were abstracted using the International Classification of Disease, 9th revision, clinical modification (ICD-9-CM) codes. We selected patients through a two-step approach, according to previously published methodologies. 14,15 First, we selected patients who underwent PCNL, using the procedure code 55.04 (percutaneous nephrostomy with fragmentation) or the combination of the codes, 55.03 (percutaneous nephrostomy without fragmentation) and 55.21 (nephroscopy). Second, we restricted our analyses to patients who had primary or secondary ICD-9 diagnostic codes for kidney lithiasis: 592.xx (calculus of kidney and ureter) and/or 274.11 (uric acid nephrolithiasis). Patients <18 years old and patients with missing information on gender, income, insurance, and hospital bed size were excluded (overall 5% of the complete population).
Study design
We evaluated the effect of obesity on perioperative outcomes following PCNL.
Covariates
Multiple patient and hospital characteristics were described. Specifically patient age, gender, race (Caucasian vs African American vs Other vs Unknown), and insurance status (Medicaid/Medicare vs Private vs Other) were described. Patient comorbidity status was calculated using the Elixhauser modification of the Charlson comorbidity index (CCI). 16 We excluded obesity from the CCI as it is our variable of interest in the current report. Median household income for the ZIP of residence was described by quartiles, according to the categorization of the respective year by the NIS. 13 Obesity status was defined as a BMI ≥30, according to the World Health Organization definition, 17 using ICD-9-CM diagnostic code 278.00 (Obesity, unspecified), V85.3x (Obesity, BMI 30–39), as well as V85.4x (Obesity, BMI 40 and over), and 278.01 (Morbid obesity). Hospital characteristics consisted of hospital bed size (High vs Medium vs Low), hospital teaching status (Nonteaching vs Teaching), hospital region (Northeast vs Midwest vs South vs West), and hospital location (Rural vs Urban), according to the NIS definitions. 13 Year of procedure was categorized as 1998 to 2002, 2003 to 2006, and 2007 to 2010. Finally, hospital volume was calculated as the number of PCNLs performed at the center for the specific year during which the index patient was treated.
Outcomes
Perioperative outcomes were defined as perioperative complications, postoperative transfusions, LOS, and total hospital charges (THCs). Perioperative complications were defined using previously published codes that were adapted to the PCNL setting. 18 They included intraoperative, cardiac, respiratory, vascular, wound/bleeding, genitourinary, gastrointestinal, neurological, sepsis, and miscellaneous complications. Transfusions were defined with ICD-9-CM procedure codes, 99.02 and 99.04, as previously published. 18 LOS was defined as a continuous variable. Additionally, LOS of >4 days (75th percentile) was defined as prolonged LOS (pLOS). THCs were available in 97% of patients. They were adjusted for inflation to the 2010 U.S. dollar, according to the Bureau of Labor. 19 THCs were defined as a continuous variable and also as a categorical variable (with two categories). Specifically, THCs were dichotomized according to the 75th percentile ($39,080). Patients who had THCs greater than this cutoff were considered to have increased THCs (iTHCs). To assure that THC and iTHC differences were not confounded by pLOS, sensitivity analyses on THCs and iTHCs were done among patients with pLOS.
Statistical analyses
A predefined discharge weight was applied for each patient to approximate national estimates. Continuous variables were described with mean and standard deviation, while categorical variables were described with frequencies and proportions. Welch's t-test and chi-square test were used to assess differences between continuous and categorical variables, respectively. Temporal trends for the number of cases and the overall charges, as well as the mean charges per hospitalization, were computed for overall, obese, and nonobese patients throughout the study period. Moreover, the proportion of PCNLs performed in obese patients was evaluated. Estimated annual percentage changes (EAPCs) were evaluated using a linear regression model. Finally, multivariable analyses adjusted for clustering were fitted to predict the effect of obesity on overall complications, transfusions, pLOS, and iTHCs. Covariates for the model included age, CCI, hospital volume, race, ZIP income, insurance status, hospital bed size, hospital teaching status, hospital region, hospital location, year of procedure, and obesity. All statistical analyses were completed with RStudio (Version 0.98). 20 Finally, all tests were two-sided and statistical significance was defined as p < 0.05.
Results
Baseline characteristics
Using weighted estimates, 90,529 patients underwent PCNL between January 1998 and December 2010 (Table 1). Of those, 9300 were obese (10.3%). Compared with nonobese patients, obese patients were significantly younger (mean age 52 vs 53, p < 0.001), less healthy (mean CCI 0.95 vs 0.76, p < 0.001), more frequently of female gender (63% vs 50%, p < 0.001), and more frequently held private insurance (57% vs 51%, p < 0.001). Moreover, obese patients were more likely to undergo PCNL at a higher volume hospital (mean cases/year 19 vs 15, p < 0.001) and at a teaching hospital (68% vs 62%, p < 0.001). Small, although statistically significant, differences were also recorded in relation to race, ZIP income, hospital bed size, hospital region, and hospital location (all p ≤ 0.03). Specifically, obese patients were more frequently of African American descent (6.8% vs 5.5%, p < 0.001), resided in a ZIP region with lower median household incomes (48.4% vs 42.8% of the first two quarters, p < 0.001), and more frequently resided in the West (20.9% vs 17.6%, p < 0.001). Finally, obese patients were more frequently treated in urban hospitals (95.5% vs 94.0%, p < 0.001) and less frequently in hospitals with small bed volumes (5.8% vs 6.4%, p = 0.03).
CCI = Charlson comorbidity index; SD = standard deviation.
Temporal trends
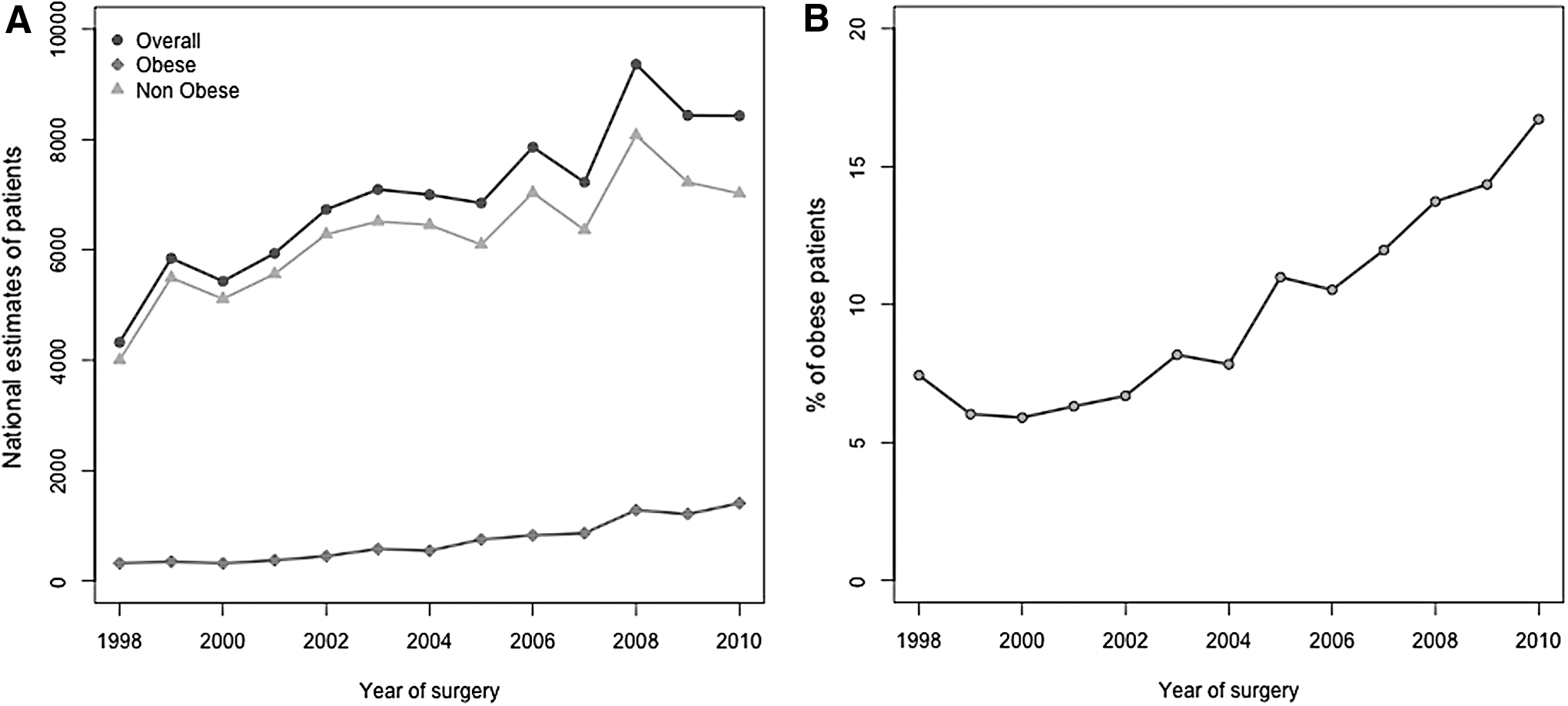
Overall, national estimates of PCNL cases increased throughout the study period (Fig. 1A). Specifically, 4325 cases in 1998 and 8430 cases in 2010 were recorded (EAPC 4.7%/year, p < 0.001). An increase was present in both the obese (EAPC 15%/year, p < 0.001) and nonobese subpopulations (EAPC 3.6%/year, p < 0.001). The proportion of obese cases throughout the years increased from 7.4% to 16.7% (p < 0.001, Fig. 1B).
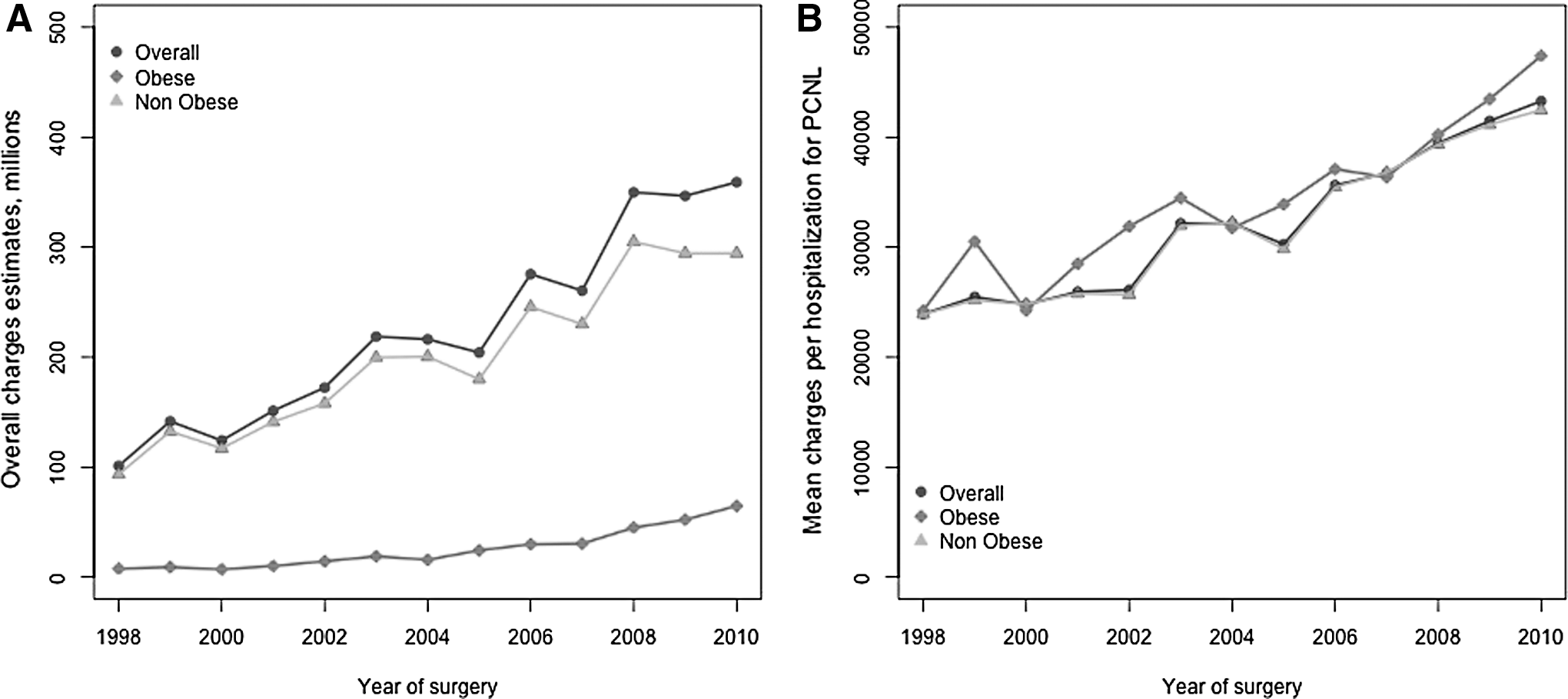
After adjusting for inflation, overall charges increased from 101 million in 1998 to 359 million in 2010 (EAPC 10.3%, p < 0.001) (Fig. 2A). Moreover, mean charges per hospitalization for the overall population also increased during the study period, from $23,922 in 1998 to $43,280 in 2010 (EAPC 5.4%, p < 0.001, Fig. 2B). The magnitude of the increase was similar in both obese (EAPC 5.1%, p < 0.001) and nonobese (EAPC 5.4%, p < 0.001) patients.
Perioperative outcomes
Any complications occurred in 21.6% and 22.0% of obese and nonobese patients, respectively (p = 0.3) (Table 2). Obese patients had fewer genitourinary complications (13.4% vs 15.0%, p < 0.001), but had higher rates of sepsis (1.7% vs 1.3%, p = 0.009), respiratory (3.0% vs 2.5%, p = 0.002), and vascular complications (0.3% vs 0.2%, p = 0.007). Transfusion rates were comparable between obese and nonobese (4.3 vs 4.0, p = 0.1) patients. Mean LOS was also similar between the two groups (3.5 and 3.4 days for obese and nonobese patients, respectively, p = 0.3). However, the rate of pLOS was higher in obese patients (20.9% vs 18.8%, p < 0.001). Mean THC was significantly higher in obese patients (mean $37,434 vs $32,793, p < 0.001). Finally, iTHCs were also more frequently recorded in obese patients (30.8% vs 24.4%, p < 0.001).
Multivariable models adjusted for age, CCI, hospital volume, gender, ethnicity, Zip income, insurance status, hospital bed size, hospital teaching status, hospital region, hospital location, year, or diagnosis.
Information was not displayed due to confidentiality reasons according to HCUP guidelines.
Information unavailable for 553 patients.
iTHCs = increased total hospital charges; LOS = length of stay; pLOS = prolonged length of stay.
Among patients with pLOS (data not shown in Table 2), mean THC was still significantly higher in the obese population (mean $64,919 vs $56,862, p < 0.001). Moreover, iTHC was recorded more frequently among obese patients (65.6% vs 58.5%, p < 0.001).
In multivariable analyses adjusted for clustering and several patient and hospital characteristics, obesity was neither associated with overall complications (odds ratio [OR] 0.94, confidence interval [95% CI] 0.84, 1.06, p = 0.3) nor was it associated with transfusions (OR 0.89, 95% CI 0.70, 1.12, p = 0.3). However, obesity was associated with pLOS (OR 1.21, 95% CI 1.07, 1.37, p = 0.002) as well as with iTHC (OR 1.17, 95% CI 1.06, 1.29, p = 0.002).
Discussion
Obesity is a growing public health issue in the United States and is associated with kidney stone formation. 21 Obese patients may also be predisposed to higher morbidity following different stone surgeries such as PCNL. We tested this hypothesis using a large population-based database, namely the NIS. Specifically, we examined the effect of obesity on perioperative complications, transfusions, LOS, and THC following PCNL.
Our findings demonstrated a number of important observations. Overall, we found that the absolute estimates of the number of PCNLs increased between 1998 and 2010. Specifically, PNCL estimates increased by ∼5% every year. The EAPC was greater for obese than for nonobese patients (15% vs 3.6%, both p < 0.001). Two possible concepts may explain this phenomenon. It may be due to the increasing incidence of obesity in the United States. Alternatively, the greater anatomical knowledge, experience, and technological advancements available may have permitted PCNLs to be performed for more difficult cases. In consequence, urologic surgeons may have developed greater expertise with PCNLs in the obese and this openness to embark on PCNLs in obese patients may have contributed to the observed phenomenon. Nonetheless, this phenomenon highlights the importance of an assessment of the effect of obesity on perioperative outcomes following PCNL.
Another important finding of this study is that in parallel to the increase in the number of PCNL cases performed every year, annual overall hospital charges due to PCNL also increased. From 1998 to 2010, overall hospital charges per year due to PCNL increased from 101 million to 359 million, which represents an approximate of 10% increase per year. Furthermore, mean charges per individual PCNL and its hospitalization increased significantly throughout the study period ($23,922 in 1998 to $43,280 in 2010). We also found that obesity was associated with higher charges, even after adjusting for other possible confounders, such as age, comorbidities, and several other variables. We first hypothesized that this phenomenon was due to higher pLOS rates. However, on further analyses that focused only on patients with pLOS, higher charges were still recorded among obese patients, demonstrating that the higher charges recorded for obese patients are due to multiple factors and not just pLOS. Taken together, the overall increase in charges associated with PCNL and its relationship with obesity are worrisome at a national level.
Interestingly, obesity was not associated with greater complication rates. Specifically, obese and nonobese patients had a 21.6% and 22.0% rate of any complications, respectively (p = 0.3). Even after adjusting for several patient and hospital characteristics, we did not record an association between obesity and complications (OR = 0.94, p = 0.3). This is in concordance with several previous reports. 5 –12 For example, El-Assmy and colleagues in a retrospective study of 1121 patients from Egypt found similar outcomes in obese and nonobese patients. 6 Similarly, Fuller and colleagues within a large multi-institutional cohort from 96 centers worldwide, also found a similar complication rate between obese and nonobese patients. 12 In addition, in a retrospective study focusing on PCNL outcomes, Gonulalan and colleagues did not record any differences among groups with different skin-to-stone distances. 10
The absence of a relationship between obesity and perioperative complication and transfusion rates may be due to better patient selection or patient referral to tertiary care centers. Indeed, we found that obese patients were more frequently treated at high-volume, academic, and urban centers. However, after adjusting for these factors in the multivariable analyses, obesity was still unrelated to perioperative complications and transfusions. Nonetheless, the current results must still be interpreted in the context of regionalization of care, where most PCNLs are performed at high-volume, academic, and urban institutions. The findings of this study are significant, in that they demonstrate that obesity by itself should not be a contraindication to PCNL, even at nonacademic, low-volume, and/or rural institutions.
Finally, it is of interest to note that obesity predisposed to different rates of specific complications without achieving clinical significance. For example, obesity was associated with a lower rate of genitourinary complications. This difference was not clinically meaningful and no explanation is available to explain this difference. Alternatively, we recorded a statistically significant different rate of sepsis, which occurred in 1.7% in obese and 1.3% in nonobese patients. Again, this difference cannot be interpreted as clinically meaningful. However, when all increased individual rates (respiratory, vascular, and septic complications) are examined as a whole, they may increase the THC for obese patients in a statistically significant and a clinically meaningful manner. This observation is hypothetical and may be implausible given the indifferent rates of overall complications. However, specific modifiable risks for these complications may be a preoperative target to improve perioperative care in obese patients. Finally, it should be noted that the higher THCs for obese patients do originate from some unfavorable characteristics that may or may not have been measured or included as variables. The same considerations apply for pLOS.
Our study is not without limitations. First of all, it is of retrospective nature. Second, neither the information on stone burden and stone type nor previous stone surgeries was available in the dataset. Third, several operative characteristics, such as operative time, intraoperative blood loss, or patient positioning, were not available. Fourth, the stone-free rate was also not available. Those limitations are noteworthy since all those characteristics could have helped to better describe the patient population and evaluate the outcomes. Fifth, due to the nature of the dataset, we were not able to report complications according to the Clavien grading system. Finally, we were not able to record the physician (radiologist or urologist) who performed the percutaneous access.
Conclusions
PCNL in obese patients did not result in higher rates of individual complications or transfusions. However, from a global perspective, it resulted in higher rates of pLOS and iTHCs.
Footnotes
Author Disclosure Statement
No competing financial interests exist.