
Abstract
Purpose:
Clinically significant urinary tract infection may be the most familiar complication of urinary catheterization; however, catheter-associated trauma can entail even more significant morbidity. We have designed and patented a novel atraumatic urinary catheter (AUC) and through this study, we compare its efficacy with the conventional Foley catheter (FC) in vivo.
Materials and Methods:
Forty male rabbits were divided into two equal groups for FC and AUC. The animals were catheterized on day 4 for 8 hours to compare the maintenance of the tubes and sedated before standardized forcible extraction of the catheter under sedation with the balloon still inflated. They were then examined visually and by cystoscopy.
Results:
In a number of animals in either group, the catheters failed to drain urine effectively due to anatomical issues. Those were excluded from the study. At the extraction phase, evidence of urethral trauma was found in 13 of 15 FC rabbits, but only in 4 of 14 in the AUC group (p = 0.009). Major trauma, however, was exclusively seen in the FC group, with 12 of 15 subjects sustaining deep lacerations or urethral disruption.
Conclusion:
The two catheters bear similar efficacy for maintaining urine drainage; however, traumatic injury is significantly less common following forceful extraction of the AUC than a conventional Foley.
Introduction
E
Our innovative design for an atraumatic self-retaining urethral catheter (registered under US Patent No. 8939962) represents a modification over the standard Foley promising to limit the risk of injury in case of inadvertent extraction with the balloon still inflated. 9 In this study, we compare the atraumatic urinary catheter (AUC) with a conventional Foley catheter (FC) in vivo.
Materials and Methods
The AUC design
The AUC like the FC is a dual-lumen tubular catheter with a balloon just proximal to its tip. The main shaft is composed of two segments, a proximal part and a distal part, with an intussuscepting junction located within the balloon cuff. When excessive traction force 10 is applied to the shaft with the balloon still inflated, its proximal and distal parts will disengage allowing the balloon to rapidly deflate into the catheter's main lumen, as demonstrated in Figures 1 and 2. 9 The AUC can be made of silicone, latex, or any common material for producing urinary catheters. In the present study, all catheters were constructed from latex.
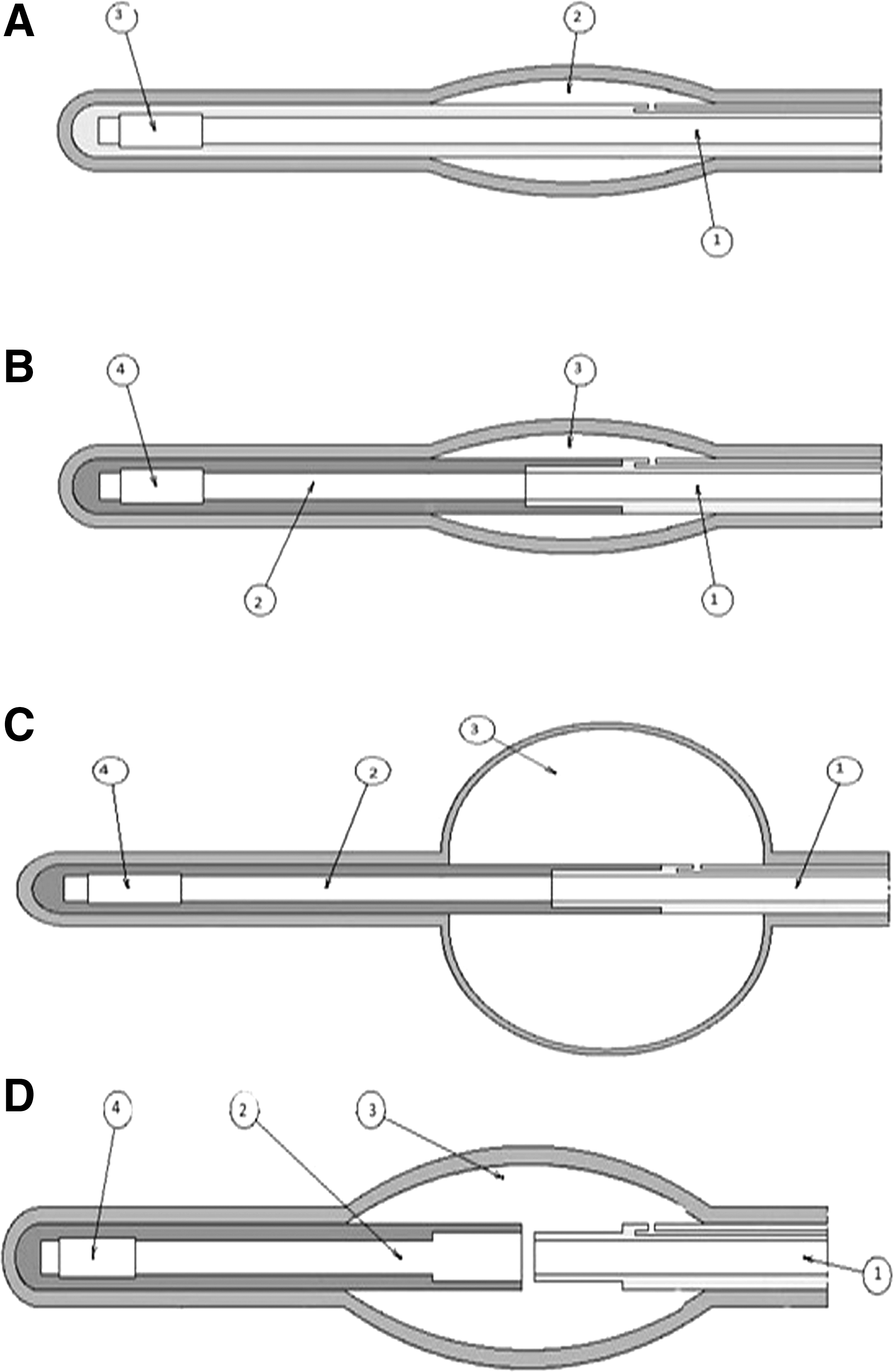
Schematic cross-sectional view of the AUC vs the standard FC.

Cross-sectional view of the AUC (Patent No: 8939962) and the FC.
The animal model
Rabbits have been recommended as an animal model for studying the bladder, urethra, and lower urinary tract system. 11,12 Despite differences in superficial anatomy of the external genitalia, the internal anatomy of their bladder outflow tract has proportions similar to and adequately resembling that of humans. Upon arrival, 40 male New Zealand white rabbits, weighing 3–3.5 kg, were maintained individually in stainless steel cages. The rabbits were acclimatized in a controlled environment (24–25°C, 50%–60% relative humidity), fed commercial pellet diet, and allowed free access to tap water for 4 days before any intervention.
Study method
After gaining approval from our institutional research ethics committee, 40 rabbits were divided into two study groups of 20 each, designated as FC and AUC. The rabbits were first catheterized with a 10F balloon catheter of the respective type after adequate lubrication. The balloon was inflated with 5 mL sterile water and the free segment secured to the abdomen and observed for 8 hours to confirm adequacy of catheter drainage and compare the hold of the balloon retention mechanism. Test subjects in which no urine drained from the catheter over the 8-hour period were categorized as drainage failures. Drainage failure results from kinking at the tip of the catheter where it abuts the bladder wall, obstructing drainage. The slender rabbit bladder appears to be anatomically prone to this, which must be taken into account if Foley-type catheters are being studied for drainage, rather than extraction injury, which was our objective. Nevertheless, drainage failures were excluded from the extraction phase of our study altogether to circumvent any interference with the results of our observation.
Next, each effectively catheterized rabbit was anesthetized with intramuscular injection of 25 mg/kg ketamine and 15 mg/kg xylazine and placed in a suspension harness fixed firmly opposite a standard push/pulling test machine (Torsee PS; Tokyo Testing Machine, Co.). With the balloon still inflated, the catheters were then rapidly extruded by the pulling machine at maximum linear speed (to simulate accidental jerking) with uniform 20 N force, based on the traumatic traction force derived for 5 mL balloon extrusion from a cadaveric model by Wu and colleagues. 10 The catheterized rabbits were evaluated for consequences of forceful balloon catheter extrusion, both visually and by cystoscopy.
The visible consequence of traumatic extrusion was categorized as a, no impact; b, urinary retention; c, gross hematuria; and d, sustained urethrorrhagia, as exemplified in Figure 3.

Visual grading of trauma from forceful catheter extraction in the rabbit.
Having observed and proven that proper nonaggressive insertion and removal of either type of catheter brings no change to the endoscopic appearance, postextraction cystoscopic findings were also classified into four categories, distinguishable from the normal endoscopic anatomy, namely, 1, bladder neck abrasion; 2, superficial mucosal tear; 3, deep urethral laceration; and 4, disruption into perivesical fat; as seen in Figure 4.
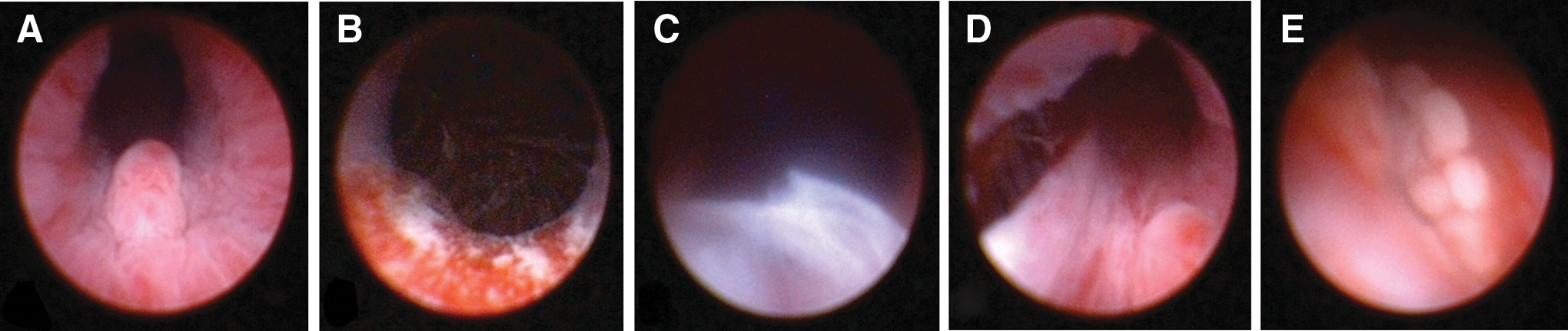
Cystoscopic grading of urethral trauma from forceful catheter extraction, compared with normal findings in the rabbit.
Fisher's exact test was used to determine significant discrepancy within the two groups. The chi-square test was used to determine any difference in the decatheterization outcome between those groups. p Values less than 0.05 were considered significant. Statistical analysis was performed on SPSS (version 11.5).
Results
In the FC group, drainage failure occurred in 5 of 20 (25%). This compared with 6 of 20 (30%) catheterizations in the AUC group. These results indicate no significant difference in drainage failure between the FC and AUC groups (p = 0.740). No catheter was expelled spontaneously in either group.
After forceful extrusion in phase two, the visible impact of this catheter-induced trauma was recorded for all subjects. As given in Table 1, pulling the catheter with such force caused significant visible consequences in 87% of standard Foley test subjects, but no visible change in 72% of those in the AUC group. Notably, the gravest clinical outcome (sustained bleeding from the urethra or urethrorrhagia) was seen in 27% of the FC group, but none of the rabbits with an AUC (p-value 0.009).
Chi-square 11.5125, p-value 0.009.
AUC = atraumatic urinary catheter; FC = Foley catheter.
Table 2 represents the results of cystoscopic evaluation following catheter extrusion. Although no single tested animal in either group was spared with a normal mucosa, 79% of AUC subjects escaped with only hyperemia, while 80% in the FC group suffered deep laceration and disruption into perivesical fat. Notably, the latter two forms of most severe injury were entirely absent from the AUC group.
Chi-square 16.39, p-value 0.009.
Discussion
Foley described his balloon catheter in 1929. Since then, its original structural design has remained the same, yielding to minor modifications in form. The composition and coating have been modified time and again though, aimed to decrease bacterial colonization. 13 Conventional FCs are flexible indwelling tubes with an inflatable balloon for bladder retention close to the bladder end. 14 Urethral catheters may be constructed from different flexible materials, including silicone, latex, or combinations thereof, and are available in a variety of sizes. 15 Indwelling catheters are widely utilized in present day clinical practice. They may be used to monitor urine output, for example, during anesthesia, relieve urinary retention, and in the chronic care setting. 16
In addition to the potential for mechanical failure when inflating and deflating the balloon, indwelling urinary catheters are associated with a number of adverse effects, of which UTI is probably the most prevalent. However, catheter-associated trauma may be as common a complication of FC use as is clinically significant infection. 17 Aggressive catheter insertion can be traumatic and so can accidental intraurethral inflation of the balloon. However, forceful pullout—short of complete deflation—is a common mishap in chronic catheterization; either as an accident or intentionally by a typical demented or agitated elderly, prompted by irritative symptoms. Failure of the jammed deflating mechanism in overdue long-term catheterization is another such setting. 18,19 Resultant trauma in these already complicated patients can further worsen the situation and necessitate additional procedures with increased morbidity and mortality rate.
We recently patented our new design for the AUC (US Patent No. 8939962), which can help address this problematic aspect of indwelling catherization. 9 The AUC has a safety mechanism incorporated within its shaft at the balloon cuff site, which allows the balloon to deflate through the main lumen if its shaft is jerked with sudden and potentially traumatic force. The pressure range required to trip this safety link can be predetermined during the manufacturing process, depending on the medical indications, patient characteristics, and catheter specifications. As with a conventional Foley, the AUC can be made of silicone, latex, and a combination of materials. The AUC has a simple design and its production cost is not significantly different than for a regular FC.
According to Davis and colleagues, balloon pressure in commercial FCs can top 700 kPa, however, urethral injury can be encountered at 150 kPa. 20 The greater the fill volume, the larger is the traction force required to withdraw the catheter from the bladder. Resting balloon pressure can be greater than 89 N for some commercial FCs. 10 Considering the above, we designed the self-retaining mechanism for this experimental study to be activated at a balloon pressure of 150 kPa, roughly corresponding to 20 N traction upon the AUC.
Through this study, we compared the efficacy of our novel atraumatic design with a conventional Foley, in minimizing the extent of injury induced by forceful catheter extraction without deflating the balloon in a controlled in vivo setting. The rabbit model has been stated as an appealing animal model for studying the lower urinary tract by Uthamanthil and colleagues 11 and McMurray and colleagues. 12
To begin with, the AUC and FC displayed no significant difference between ineffectively draining urine from the rabbit bladder. Failure to drain was encountered in 20%–30% of attempted catheterizations with no discrepancy between the two catheters (p-value 0.740). According to previous studies in rabbits, these drainage failure rates are in normal range. 11 All test subjects failing effective drainage were excluded from the extrusion phase to maintain maximum fidelity.
Of the rabbits tested for deliberate extrusion of the FC, 87% sustained objective signs of outflow tract injury. Most notably, immediate urethral bleeding corresponding to significant laceration was only encountered in the FC group and did not happen with the AUC. An additional 60% of FC subjects developed gross hematuria and/or urinary retention, hallmarks of less severe trauma. Gross hematuria and retention were observed at less than half this rate in the AUC group (standing at 28%).
Therefore, by implementing the safety mechanism in the AUC, we can expect to practically circumvent catastrophic trauma from accidental forceful extrusion of the indwelling catheter. Moreover, it may even slash the incidence of less severe injury by half. The relative preventive efficacy of this novel design is more clearly displayed by comparing the proportion of subjects sustaining no objective sign of injury: 71% remaining uninjured on the AUC vs only 13.3% on FC (p-value 0.009).
Conclusion
In conclusion, the safety advantage of the AUC can be put to good use for prevention of accidental iatrogenic urethral injury in at-risk populations such as the elderly and institutionalized patients with dementia; delirious, agitated, and aggressive psychiatric patients prone to self harm, and most care seekers requiring long-term catheterization.
Footnotes
Acknowledgments
The authors express their gratitude to the staff at the HKC clinical skill laboratory for their generous help and to the Razi Institute animal laboratory for supplying the animals in due time.
Author Disclosure Statement
The authors have received no extra institutional or commercial support for this study and therefore declare no conflicts of interest. A limitation of this study may be the modest number of samples, but the indisputably large margin of significance in comparing the outcome in the two groups can be concerting.