
Abstract
Purpose:
To investigate the impact of positive surgical margins (PSM) on overall survival (OS) in a large American cohort with intermediate-term follow-up.
Patients and Methods:
Using the National Cancer Data Base, we identified 6038 cases of pathological T1–T3a, nonmetastatic renal-cell carcinoma managed with partial nephrectomy (PN) from 2003 to 2006. Patients were stratified into two groups based on margin status. Predictors of positive margins were evaluated using multivariable logistic regression analysis. OS by margin status was evaluated using Kaplan–Meier analysis and the log-rank test. A multivariable Cox proportional hazards model was used to evaluate the adjusted association between margin status and survival.
Results:
Overall, 302 (5.3%) patients had positive margins. On multivariable analysis, higher pathological T stage and higher comorbidity score were the only factors significantly associated with positive margins (p < 0.001 and p = 0.015, respectively). At 71-month median follow-up, the unadjusted 5-year OS for the entire cohort was 92%. Positive margins were significantly associated with decreased 5-year OS (89% vs 92%, p = 0.002), and this association remained significant in healthy patients (p = 0.027). On multivariable survival analysis, positive margins significantly predicted hastened time to all-cause death (hazards ratio 1.34; 95% CI 1.01, 1.78; p = 0.038).
Conclusion:
In the largest observational study to date, PSM were associated with worse OS after PN. Further study on cancer-specific outcomes with long-term follow-up is needed.
Introduction
P
Patients and Methods
NCDB participant user file for kidney cancer
The NCDB is a joint project of the American Cancer Society and the Commission on Cancer of the American College of Surgeons. It is a large, hospital-based cancer registry database that captures data on ∼70% of all malignancies in the United States annually. The NCDB kidney data set has been described in detail previously. 19 After the Institutional Review Board approval, we used the NCDB's participant user file for kidney cancer.
Study population
Using primary site coding from the International Classification of Diseases for Oncology, 3rd edition, we identified 120,926 patients with RCC diagnosed from 2003 to 2006 to allow a minimum of 5-year follow-up for each patient. Patients before 2003 were excluded because Charlson comorbidity index (CCI) data were unavailable. Only patients with clinical T1–T2 or pathological T1–T3a, nonmetastatic (N0/Nx, M0/Mx) RCC were included (n = 42,642). Patients with T0 stage or unknown tumor size were excluded (n = 11,555). We restricted the cohort to patients who underwent PN (n = 7659). Last, patients with other primary malignancies were excluded (n = 1595) to avoid potential confounding, and cases diagnosed but not treated at the reporting facility were excluded because of missing follow-up data (n = 26).
Study variables
Data elements used in this study included age, sex, CCI, race, insurance type, tumor size, pathological T (pT) stage, tumor histology, tumor grade, and margin status. Age (in years) and tumor size (in centimeters) were treated as continuous variables; all other variables were categorical. Missing data for the race, insurance, and grade variables were included as unknowns. CCI, which was calculated based on the International Classification of Diseases, 9th edition, clinical modification, and secondary diagnosis codes, was categorized as 0 (no comorbidities), 1, or >1. Race was categorized as White or non-White. Insurance type included no health insurance, social (Medicare/Medicaid), and private/managed care. Pathological T stage included T1–T3a. Tumor histology was categorized as clear-cell RCC, papillary RCC, chromophobe RCC, and others. Grade was characterized as low (well differentiated or moderately differentiated) or high (poorly differentiated) based on the Fuhrman nuclear grading system.
Study outcomes
The primary outcome was overall survival (OS) calculated from the date of PN to the date of death from all causes or censored at the date of last contact in living patients. For the overall cohort and in patients with CCI <1, regardless of margin status, the event rate did not reach 50% by the end of the study period; therefore, the median survival time could not be calculated. Accordingly, the primary outcome was expressed in terms of the 5-year OS.
Statistical analyses
Patients were categorized into two comparison groups: a PSM group and a negative surgical margins (NSM) group. On univariate analysis, continuous variables were compared using the Wilcoxon–Mann–Whitney test, and categorical variables were compared with the chi-squared test. The Kaplan–Meier method and log-rank test were used to examine OS. A repeat Kaplan–Meier analysis was performed for OS stratified by CCI. A multivariable Cox proportional hazards model was performed to evaluate the association of margin status and OS when accounting for additional covariates. Statistical tests were performed using SAS® University Edition (SAS Institute Inc., Cary, NC). p-Values <0.05 were considered statistically significant.
Results
The final study cohort included 6038 patients who underwent PN for clinical T1–T2 RCC (Table 1). The median age of patients was 58 years (IQR 49–67); 60% of patients were male; and 81% were White. The median tumor size was 2.5 cm (IQR 1.9–3.5). By pathological T stage, 96% of tumors were T1, 2.1% were T2, and 2.3% were T3a. Clear-cell or other RCC histology was found in 64% of tumors, and 15% of tumors were high grade.
Bold indicates statistical significance.
CCI = Charlson comorbidity index; IQR = Interquartile range; NSM = negative surgical margins; PSM = positive surgical margins.
Overall, 5.3% (302/6038) of patients had PSM. On univariate analysis, PSM were significantly associated with age, CCI, and pT stage (Table 1). Specifically, patients with PSM were more likely to be older, more highly comorbid, and afflicted with higher stage disease. On multivariable analysis, only CCI and pT stage were significantly associated with PSM, p = 0.015 and p < 0.001, respectively (Table 2). Otherwise, patient and disease characteristics for those with and without PSM did not differ significantly (Table 1).
Bold indicates statistical significance.
The median follow-up was 71 months (IQR 56–85), and follow-up did not differ significantly between the PSM and NSM groups (72 months [IQR 56–85] and 71 months [IQR 55–84], respectively; p = 0.653). At last contact, 699 (11.6%) patients died, including 11.3% (647/5736) with NSM and 17.2% (52/302) with PSM. The unadjusted 5-year OS for the entire cohort was 92%. Based on unadjusted Kaplan–Meier analysis, OS differed significantly by margin status (Fig. 1, p = 0.002). PSM status was associated with decreased 5-year OS (89% vs 92%). After classifying the cohort by CCI, PSM remained a significant predictor of decreased 5-year OS (91% vs 94%) in patients with CCI <1 (Fig. 2A, p = 0.027). Patients with a CCI of 1 or >1 had worse OS, but margin status was not significantly associated with a difference in OS (Fig. 2B, p = 0.349; Fig. 2C, p = 0.302).
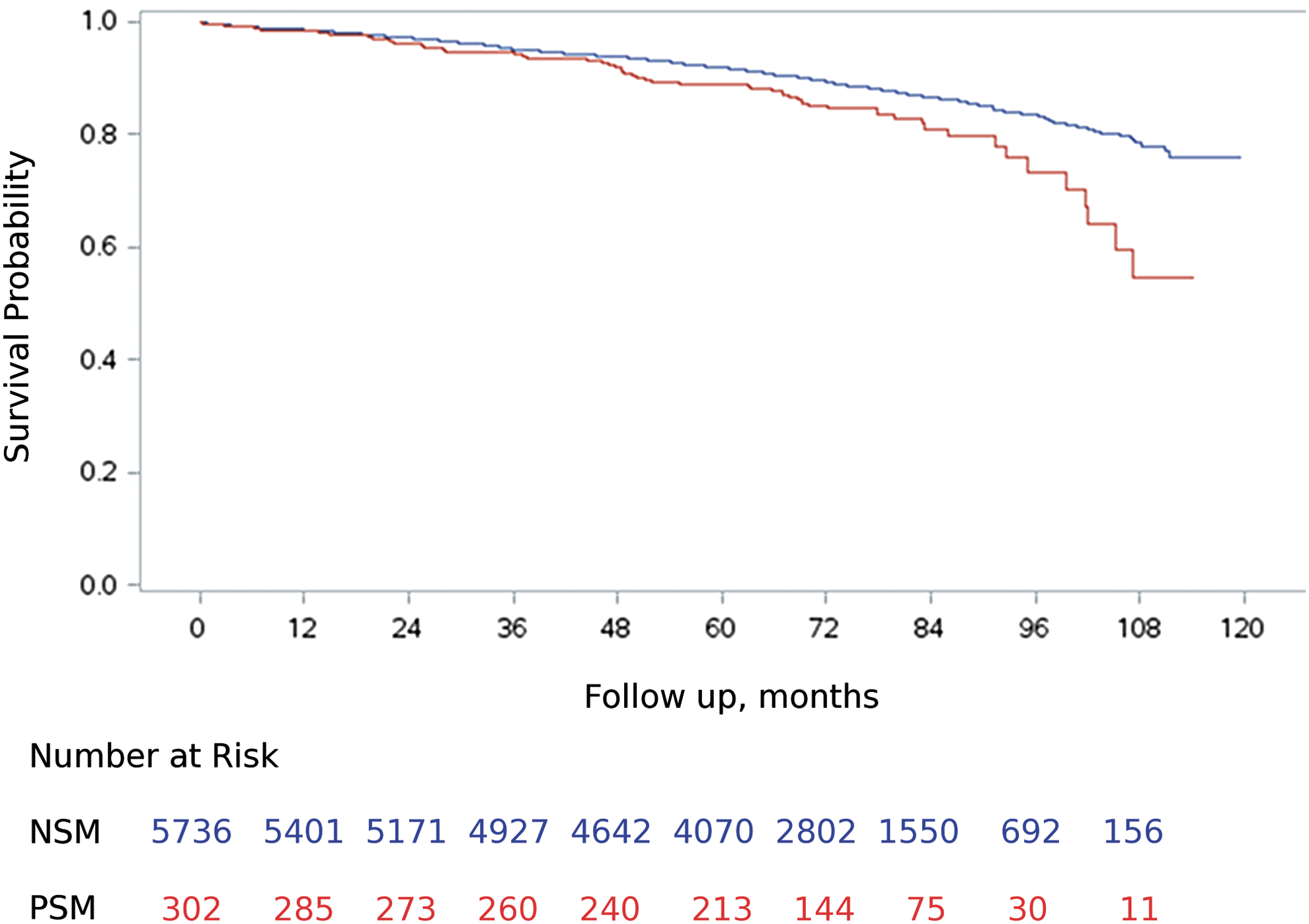
Kaplan–Meier survival curves for PSM (red) and NSM (blue) after PN. NSM = negative surgical margins; PN = partial nephrectomy; PSM = positive surgical margins.
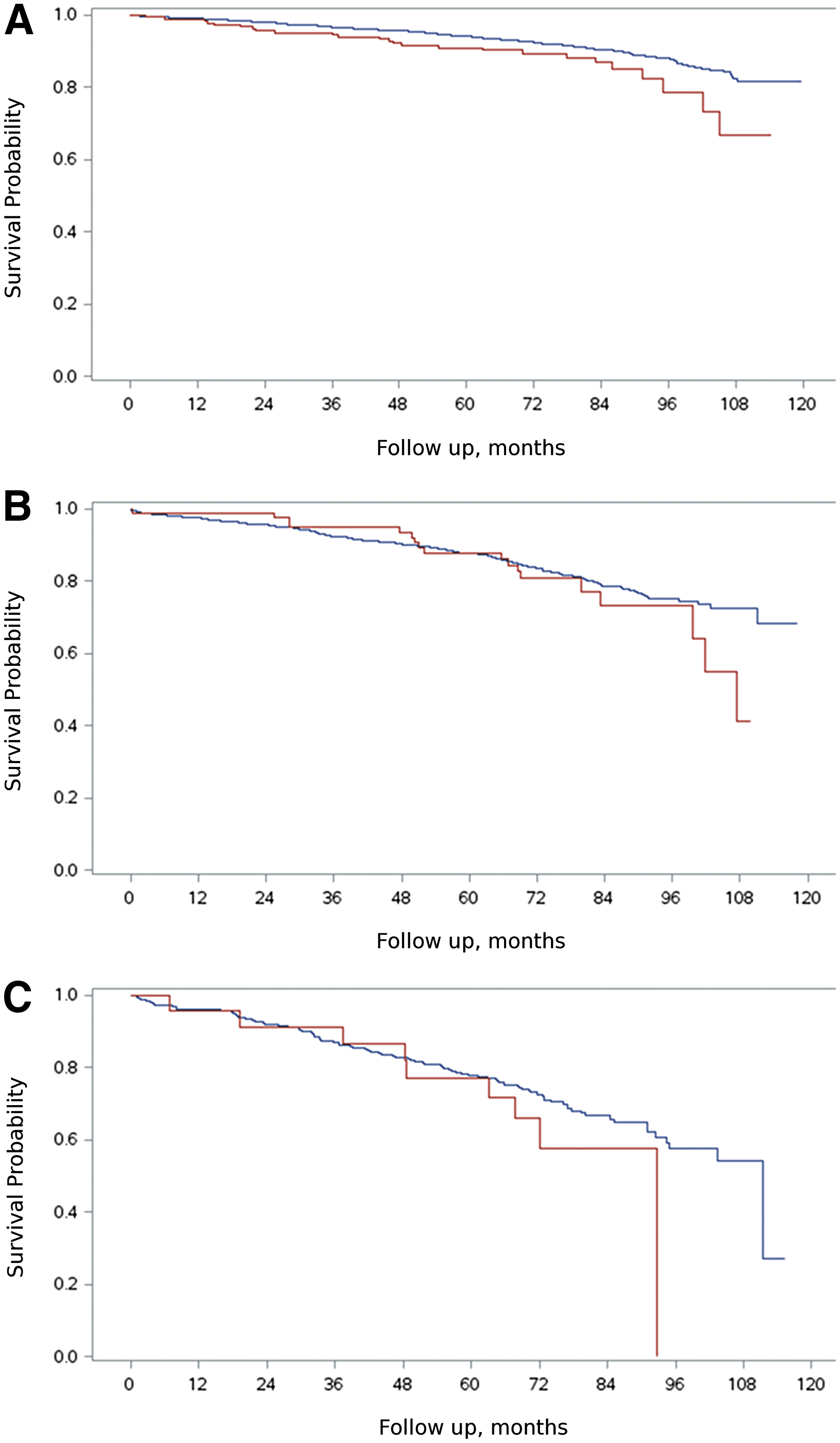
Kaplan–Meier survival curves for PSM (red) and NSM (blue) after PN stratified by Charlson comorbidity index of 0
After adjusting for age, sex, CCI, race, insurance type, tumor size, pathological T stage, histology, and grade, patients with PSM had significantly worse OS compared with those with NSM (hazards ratio 1.35; 95% CI 1.02, 1.80; p = 0.038; Table 3). Other significant predictors of decreased survival were older age, male sex, higher CCI, increased tumor size, higher pathological T stage, and nonchromophobe histology.
Bold indicates statistical significance.
Discussion
The contemporary ideal PN must strike a delicate surgical balance between achieving oncological control and maximizing renal preservation. 20 However, despite a surgeon's best efforts, this pursuit to secure a thin, cancer-free margin is occasionally thwarted. While PSM are usually an infrequent event, they appear to be influenced by patient, disease, and provider factors, including imperative indications for renal preservation, small (possibly endophytic) tumors, upper pole tumors, higher grade or stage tumors, and surgical approach. 8,12,14,21 While PN is generally considered a safe and effective treatment for T1 renal masses, the clinical significance of PSM after PN is unclear. 1 –3 Despite this uncertainty, PSM status is still the best immediate surrogate for oncological control in localized RCC and has been suggested as a potential quality indicator. 22,23 We sought to better elucidate the impact of PSM on survival.
In this study, we report on a large, hospital-based cohort of American RCC patients with a 5% prevalence of PSM after PN. This prevalence corroborates rates previously reported in the literature, ranging from 2% to 13%. 4 –14 With a median follow-up of 5.9 years, we found that PSM were significantly associated with worse OS. However, this association does not imply causation. Since the NCDB does not include information on cancer recurrence, cause of death, or secondary treatments, the exact cause of the excess mortality rate in PSM patients is unknown and not necessarily due to RCC. Nonetheless, this is the first study to detect a statistically significant difference in OS in PSM patients, which may be attributed to the robust cohort of more than 6000 patients, the ample prevalence of PSM (n = 302), the statistically sufficient event rate (n = 699), the inclusion of 9 other variables (aside from margin status) in the multivariable hazards model, and the longer term follow-up data. This association was only noted for healthy patients, possibly due to the long natural history of RCC recurrence after resection with curative intent and the increased risk of noncancer mortality rate in patients with multiple comorbidities. 24
Consistent with the literature, we confirmed that higher pT stage was a significant predictor of PSM. 12 We also noted a significant association between higher CCI and PSM, which has not been previously observed. 14,21 Adherent and/or abundant perirenal fat, which is associated with common comorbidities, including obesity, hypertension, and smoking, increases the technical difficulty of dissection during PN and may explain the association between CCI and PSM. 25 Another possible explanation is that comorbidity is somehow linked to RCC aggressiveness. While this phenomenon has not been described previously in the RCC literature, higher comorbidity burden has been associated with more aggressive disease in both prostate cancer and breast cancer. 26,27 Alternatively, it is possible that some unknown confounding variable, for which we were unable to adjust, such as surgical approach, may have resulted in a spurious association. 14 Due to the limitations of the database, we were unable to evaluate the impact of certain tumor characteristics, such as endophyticness, nearness to the collecting system or sinus, and location relative to polar lines on the occurrence of PSM.
The clinical significance of PSM after PN is still highly contested. Various institutional studies have retrospectively assessed the clinical outcomes of patients with PSM after PN and have arrived at conflicting results, even within the same institution. 8,10,13,15 –17 In an initial report of 777 PNs performed at the Memorial Sloan Kettering Cancer Center, Kwon and colleagues noted that patients with histologically aggressive tumors and PSM after PN were more likely to recur locally. 8 In a multi-institutional study of 809 PNs, Bernhard and colleagues upheld PSM status as an independent predictor of ipsilateral RCC recurrence. 17 In yet another multi-institutional study of 943 robot-assisted PNs, PSM were associated with a significantly higher rate of recurrence and metastases. 13 Alternatively, other observational studies, including an updated analysis of the Memorial Sloan Kettering experience, have contradicted these findings. 10,16 In the largest study, before our own, of 111 patients with PSM, Bensalah and colleagues did not detect a significant difference in recurrence-free, cancer-specific, or OS. 16 Major limitations of all these studies were their short- to intermediate-term follow-up, low event rate, and small sample sizes. With a median follow-up of 1.1 to 3.4 years and only 56 PSM events, on average, per study, none of these studies had adequate follow-up or power to assess the long-term oncological implications of PSM.
In a well-designed population-based study using data from the Ontario Cancer Registry, no association was found between PSM and cancer-specific or OS with a median follow-up of 7.9 years. 12 However, the unusually high PSM rate of 11% in this population raises concerns about the pathological accuracy, especially in the absence of central pathological review. Despite this high event rate, the study only included 71 patients with PSM. Furthermore, due to the limitations of the database, this study could not account for several potential confounders, including comorbidities, race, and tumor histology, which may have biased the results.
The long-term outcomes and optimal management of PSM are also uncertain. Based on available case series with at least intermediate-term follow-up, on average, local or systemic recurrences occur in 11% of PSM patients, and of these, 45% (range, 0%–100%) eventually die from RCC. 4 –6,8,9,15,16 The risk of recurrence and eventual progression may be highest in patients with aggressive disease. 8 However, an independent association between PSM and cancer-specific survival has not yet been established. 12,16 Based on our analysis, PSM were only clinically significant in healthy patients, which may explain why an association between PSM and survival has not been previously detected. Since nearly 90% of patients with PSM do not recur and given that PSM do not always equate to residual disease, re-resection or completion nephrectomy is usually unnecessary. 28 Therefore, pending confirmation of our recent findings in terms of cancer-specific survival, the existing evidence favors a conservative approach to PSM with close monitoring, especially in patients with more aggressive disease and/or greater longevity.
Our study has several noteworthy limitations, including susceptibility to bias due to its retrospective design and the limitations of the NCDB itself. Since follow-up information in the NCDB is limited to vital status, we were only able to assess OS as our primary outcome. That being said, given concerns about the overtreatment of patients with PSM, 28 OS is arguably the most important clinical outcome after PN. Our findings suggested that PSM predict decreased OS; however, without information on cancer-specific recurrence, progression, and/or death, it is unclear whether PSM played a causative role. By adjusting for multiple confounding variables in our analysis, including age, sex, CCI, race, insurance provider, tumor size, tumor stage, tumor histology, and tumor grade, which impact OS, we were able to partially compensate for potential bias. Our study suggests a true association between PSM and survival. However, there are several important factors not included in the NCDB, including postoperative renal function and subsequent PSM management (i.e., observation vs completion nephrectomy vs repeat PN), for which we could not adjust, that may have biased our results. Regarding our analysis of PSM predictors, we were unable to adjust for several other variables, which may have biased these results as well, especially imperative indications for PN, tumor location, tumor complexity, surgical approach, and surgeon experience. Last, due to the long natural history of post-PN RCC, median survival was not reached in our study; therefore, longer follow-up is needed in future studies.
Conclusions
In conclusion, PSM are an infrequent event after PN but appear to be associated with decreased OS at 5.9-year median follow-up. Further research looking at cancer-specific outcomes with long-term follow-up is needed to confirm the clinical significance of this finding.
Footnotes
Acknowledgments
The American College of Surgeons and the Commission on Cancer have not verified and are not responsible for the analytic or statistical methodology used or the conclusions drawn from these data by the investigator.
Author Disclosure Statement
No competing financial interests exist.