
Abstract
Introduction:
Intracorporeal suturing is considered to be the most challenging aspect of laparoscopic and robotic surgery. To overcome this problem, barbed self-retaining sutures have been effectively employed in various minimally invasive endourologic surgeries. However, the use of this suture has been recently cautioned for pyeloplasty due to a high failure rate. Our objective was to report our experience using barbed suture during robotic pyeloplasty.
Methods:
We retrospectively identified 13 consecutive patients who underwent robotic pyeloplasty with a barbed monofilament (4-0 V-Loc™) suture for the ureteropelvic anastomosis from 2011 to 2014. We compared these patients to 12 consecutive patients who underwent robotic pyeloplasty with a 4-0 nonbarbed suture from 2007 to 2011. We evaluated patient demographics, operative times, preoperative and postoperative symptoms, renal function, and diuretic renograms (DRG). Successful repair was defined as resolution of preoperative symptoms and/or T½ improvement on DRG to less than 20 minutes.
Results:
The median age was 26 (interquartile range [IQR] 20.7–38) years and 35 (IQR 18.3–44) years for the barbed and nonbarbed suture groups, respectively. In the barbed suture group, preoperative DRG revealed ureteropelvic junction obstruction (UPJO) in 11 patients, equivocal UPJO (T½ 10–20 minutes) in one patient, and no obstruction in one patient. In the nonbarbed group, preoperative DRG revealed UPJO in 10 patients, equivocal UPJO in one patient, and no obstruction in one patient. In the barbed suture group, postoperative DRG was obtained in 11 patients, which showed no obstruction in 10/11 patients with 92% of patients experiencing symptom resolution. Similarly, postoperative DRG was obtained in 11 patients in the nonbarbed group, which showed no obstruction in 10/11 patients with 100% postoperative symptom resolution.
Conclusions:
In the largest series reporting use of V-Loc suture for robotic pyeloplasty, the V-Loc suture was safely and effectively used for robotic pyeloplasty repair.
Introduction
I
However, the use of this suture has been recently cautioned for minimally invasive pyeloplasty (MIP) due to a high failure rate published in one series. 5 Theories on the reason for failure include that the suture may cause increased ischemia from the minimal tissue bulk involved in the ureteropelvic junction (UPJ) anastomosis or if the suture is pulled too tight inadvertently. A recent editorial 6 strongly urged publication of any favorable results in MIP using this suture. Our objective was to report our experience using a barbed suture during robotic pyeloplasty.
Materials and Methods
Following institutional review board approval, we retrospectively reviewed the records of 25 consecutive patients who underwent MIP as performed by two surgeons (R.K. and R.O.) from December 2007 to July 2014. We identified 13 patients after January 2011 who had a barbed monofilament 4-0 V-Loc™ (Covidien, Mansfield, MA) suture used for the UPJ anastomosis. This group was compared with 12 consecutive patients who had a 4-0 nonbarbed suture used for the UPJ anastomosis before 2011. We evaluated patient demographics, preoperative and postoperative symptoms, renal function, and diuretic renograms (DRG). Symptomatic pain resolution was defined as the patient subjectively reporting that his/her pain had completely resolved following surgery without need for analgesic medications. Successful repair was defined as resolution of preoperative symptoms and/or T½ improvement on DRG to less than 20 minutes.
Surgical technique
All patients underwent transperitoneal MIP using the da Vinci® Robot (Intuitive Surgical, Sunnyvale, CA). We primarily used the Anderson-Hynes dismembered pyeloplasty technique except for five difficult cases (one nonbarbed and three barbed group) where we used Foley YV plasty technique. For the dismembered technique, we either place a 5-0 polypropyelene suture through the proximal ureter or use the redundant diseased UPJ as a handle to manipulate the ureter to employ a no-touch technique. A diamond-shaped incision is created at the UPJ with robotic Potts scissors. The proximal ureter is spatulated by angling laterally. With larger redundant renal pelvises, the excess renal pelvis is excised and closed with a continuous 4-0 polyglactin suture placed at the lateral aspect of the renal pelvis running toward the anastomosis. One 4-0 V-Loc is then used for the posterior and another for the anterior portions of the running anastomosis with a Lapra-Ty™ device applied on both ends in the barbed group. Alternatively, two interlocked 4-0 V-Loc sutures are placed at the apex of the spatulation into the ureter and the posterior anastomosis to the pelvis is performed in a running manner followed by the anterior. In the nonbarbed group, we used either a 4-0 polyglactin or 4-0 poliglecaprone for the running anastomosis. A 6F stent is placed through the antegrade approach over a Sensor™ (Boston Scientific, Natick, MA) wire after filling the bladder with irrigant to ease placement before completion of the anastomosis. A self-suction drain is placed near the anastomosis in each patient, exiting through the most inferior robotic port site.
Foley YV plasty was performed whenever it was observed that a tension free dismembered pyeloplasty was not possible. The V flap was outlined with stay sutures. The base of the V was positioned on the dependent medial aspect of the renal pelvis and the apex at the UPJ. The incision from the apex of the flap, which represents the stem of the Y, was then carried along the lateral aspect of the proximal ureter well into an area of normal caliber. The flap was developed with robotic Potts scissors. The apex of the pelvic flap was brought to the inferior-most aspect of the ureterotomy incision and an interrupted 4-0 polyglactin suture is placed to secure this. Then either 4-0 nonbarbed or 4-0 V-Loc is run on the posterior walls, the stent is inserted antegrade, and then the anastomosis is completed with approximation of the anterior walls.
Postopertive and follow-up
Patients were discharged home within 2–3 days following the surgery. The drain was discontinued in the hospital after confirming that the drain creatinine level was consistent with serum. The stent was removed in the office without retrograde pyelography following 6 weeks and DRG was performed at 3 months postoperatively.
Statistical analysis
Continuous variables were compared with either the Student's t-test or Mann–Whitney U-test. Categorical variables were compared with Fisher exact or Chi-square test. Statistical significance was considered at p ≤ 0.05. All statistical analyses were performed using Stata® statistical software, version 11.0 (StataCorp, College Station, TX).
Results
The demographics, presentation, and clinical findings of the cohort are listed in Table 1. Overall, the barbed and nonbarbed groups were similarly matched except for body mass index (27.6 ± 4.8 kg/m2 vs 23.1 ± 3.2 kg/m2, p = 0.01, respectively) and follow-up (11 ± 8 months vs 37 ± 27.5 months, p < 0.01, respectively). There were eight patients having ≥6-month follow-up in the barbed group. Mean operative time was 35.8 minutes shorter in the barbed group, however, this was not statistically significant (p = 0.10). All, but one patient in each of the groups had preoperative clinical symptoms in the form of flank pain on the affected side. The one patient in the nonbarbed group without flank pain was found to have obstruction on DRG following work-up for a febrile urinary tract infection. The one patient in the barbed group without symptoms had developed a UPJ stricture following renal trauma and was found to have a worsening renal ultrasound with obstruction on DRG. In the barbed group, preoperative DRG revealed ureteropelvic junction obstruction (UPJO) in 11 patients, equivocal UPJO (T½ 10–20 minutes) in one patient, and no obstruction in one patient. The latter two patients were operated on for both symptoms and worsening renal ultrasound. Repair was primary in 11 patients and secondary in two patients. In the nonbarbed group, preoperative DRG revealed UPJO in 10 patients, equivocal UPJO in one patient, and no obstruction in one patient. The latter two patients were operated on for both symptoms and findings of a crossing vessel on imaging. All 12 patients in the nonbarbed group underwent primary repair.
BMI = body mass index; DRG = diuretic renograms; EBL = estimated blood loss (in mL); IQR = interquartile range; SD = standard deviation; UPJ = ureteropelvic junction; UPJO = ureteropelvic junction obstruction; MDRD = modification of diet in renal disease; eGFR = estimated glomerular filtration rate.
Postoperative DRG revealed no obstruction in 11/12 (84.6%) patients in the barbed group and 10/11 (83.3%) patients in the nonbarbed group (p = 0.95.) The improvement in the T½ between preoperative and postoperative DRG for the barbed suture group is shown in Figure 1. The mean% change improvement in the T½ was 55%. The one patient still meeting criteria for obstruction did show a much improved washout on DRG with a 69% improvement in T½. That patient also had a prior open UPJ repair. There was no worsening in relative renal function from preoperative to postoperative DRG for any patient. Symptom resolution was seen in 92% of patients. The one patient whose symptoms did not improve had a history of substance abuse and showed no obstruction on postoperative DRG.
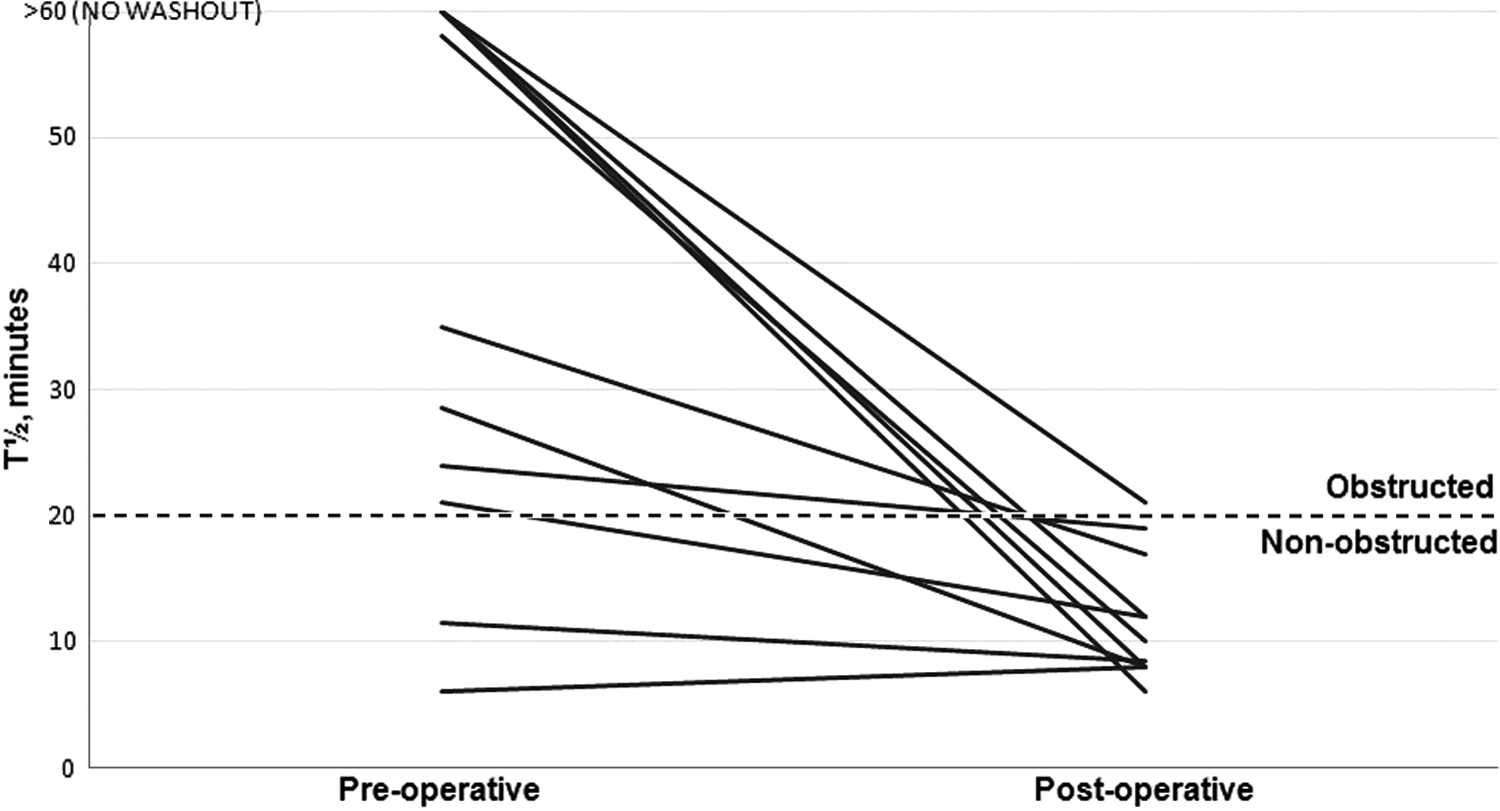
Preoperative and postoperative DRG in the barbed suture group. All, but one patient had radiographic evidence of no obstruction following robotic pyeloplasty. DRG = diuretic renograms.
The improvement in the T½ between preoperative and postoperative DRG for the nonbarbed suture group is shown in Figure 2. The one patient still meeting criteria for obstruction did show a much improved washout on DRG with a 64% change improvement in T½. Symptom resolution was seen in all patients. There was no significant deterioration in renal function in any patient. There were no significant complications in both groups. There were no known incidences of urine leaks or urinomas, and drain duration was similar in both groups.
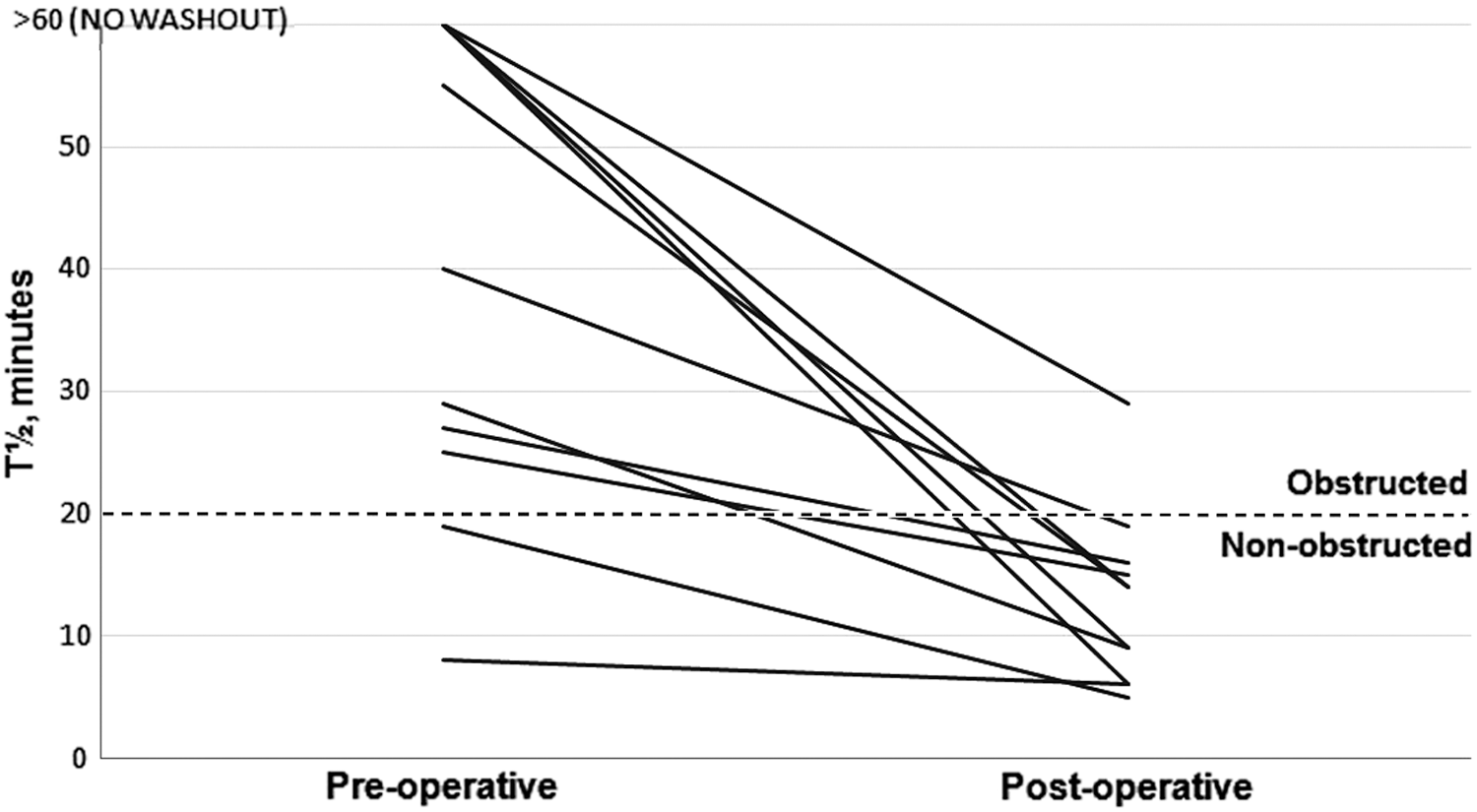
Preoperative and postoperative DRG in the nonbarbed suture group. All, but one patient had radiographic evidence of no obstruction following robotic pyeloplasty.
Discussion
Our results show successful outcomes for robotic pyeloplasty using the barbed V-Loc suture for the UPJ anastomosis. In the only other study that has shown successful outcomes using barbed suture, Shah and colleagues 4 briefly described their experience in nine patients who did not have any postoperative evidence of urinary extravasation. Seven patients completed the 6-month follow-up and did not have any radiological signs of obstruction. However, the authors did not go into further details as they also described the barbed suture's success in various other surgeries such as robotic cystectomy and prostatectomy. Our series was slightly larger with all 13 patients having no signs of urinary extravasation. We have had eight patients who completed the 6-month follow-up and none has had postoperative symptoms. Only one patient met criteria for obstruction on DRG by 1 minute. This was a secondary repair case that underwent Foley YV plasty. While technically that is considered a failure by the study's definition, clinically it was a success given the greatly improved washout on DRG and resolution of preoperative symptoms.
The success rate for robotic pyeloplasty in primary and secondary repair using a standard 4-0 polyglactin suture has been shown to be 96.1% and 94.1%, respectively. 7 The senior surgeon reporting such successful results was highly experienced with robotic UPJO management. The senior surgeon (R.K.) on this study performed 12 robotic pyeloplasty surgeries before the first case of using a barbed suture. With known highly successful results using a standard polyglactin, the transition to the V-loc suture was done to facilitate intracorporeal suturing and thus improve operative times as confirmed by a previous in vitro study. 8 Operative times did improve for the barbed suture cohort by a mean of 35.8 minutes in our series, however, this was not statistically significant. It is difficult to compare operative times in a training program where the experience of participating residents may be highly variable. In addition, the theoretical advantage of shortening the learning curve for novices is difficult to investigate. Theoretically, if the improvement in operating time was significant, the relatively low cost of the V-Loc ($22) and Lapra-Ty ($83) devices 9 compared with the cost of operating room time ($15–$20 per minute) 10 would reduce costs on an average by $589 per case. The ease and success of this suture in UPJ reconstruction warrants further investigation in future primary repairs. Prospective analysis of suturing times for trainees with a barbed and nonbarbed suture, for example, may serve to better answer the question.
We have limited experience with the barbed suture in secondary repair cases. It has been used in only 2/13 patients in our series with one success following prior balloon endopyelotomy and one radiographic failure following open pyeloplasty. This suture may have a potential role in secondary repair, but this also needs further study.
Liatsikos and colleagues 5 recently published their initial unfavorable results with a barbed 4-0 Quill™ (Angiotech, Vancouver, British Columbia) suture in a small series of six patients undergoing dismembered MIP utilizing conventional laparoscopy. The three surgeons from the series are highly experienced laparoscopic surgeons who had previous experience using barbed sutures in both laparoscopic and robotic prostatectomy. Five out of six patients were failures showing both UPJ stenosis on retrograde pyelography at 1 month and obstruction on DRG 4 months postoperatively. The failed cases ended up undergoing salvage endourological or open intervention. These failures were potentially attributed to learning curve, overtightening of the suture, and the intrinsic characteristics of the suture itself, which may elicit inflammation and fibrosis. The surgeons abandoned the barbed suture stating it was not a good option for upper urinary tract reconstruction. Their opinion was also echoed by another highly experienced laparoscopic surgeon stating that if the suture is pulled too tightly, it could inadvertently render the anastomosis ischemic. 6 The use of the robotic platform for ease of suturing in our series compared with conventional laparoscopy, which may be putting undue tension on the anastomosis, may certainly be a strong factor for our success rate. Future studies looking into the force used to create the UPJ anastomosis and success in MIP are certainly warranted.
One hypothesis that could explain the difference between our favorable results and the study by Liatsikos and colleagues 5 is from the use of different barbed sutures. They used 4-0 Quill, which is a bidirectional barbed suture as opposed to the unidirectional barbs on the V-Loc. These two sutures were tested in wound closure in a porcine model and the V-Loc was noted to be significantly stronger than Quill during the critical phases of wound healing (days 0, 3, and 7). 11 This is likely due to the differences in barb geometry of the sutures. The V-Loc is created with dual cut angle making the barbs shorter and more rigid, while the Quill is cut with a single cut angle making it more flexible and prone to slippage. Thus, the design of the barbs on the V-Loc results in greater tissue holding capacity due to the lower cut angle. Weld and colleagues 2 noted that the Quill trended toward a greater degree of fibrosis compared with standard suture in porcine pyeloplasty, but this was not statistically significant (p = 0.11). However, the degree of fibrosis was significant for Quill sutured bladder neck anastomosis from the higher surface area of the barbing process. The difference in design of the V-Loc and Quill may elicit different degrees of fibrosis leading to failure. Otherwise, the unidirectional vs bidirectional barbs do not seem to make a difference in water-tightness. However, fibrosis and water-tightness have never been compared between the Quill and V-Loc suture, nor have the two sutures been compared head to head in a randomized trial for robotic pyeloplasty. It is interesting to note that the other studies on robotic pyeloplasty with barbed suture by Shah and colleagues 4 employed a V-Loc rather than the Quill.
There are several limitations to the study. The retrospective design of the study precluded a standardized questionnaire for reporting symptom improvement. While we did not obtain DRG on two patients, they did not report any postoperative pain. We also do not routinely perform retrograde pyelograms during stent removal unless obstructive symptoms are suspected. While currently this is the largest series using the V-Loc suture, it is still relatively small to draw any confident conclusions. However, the majority of our patients have had a long-term follow-up, and the barbed suture repairs appear durable thus far.
Conclusions
In the largest series reporting use of a barbed suture for robotic pyeloplasty, the V-Loc suture was safely and effectively used for primary robotic pyeloplasty repair. This suture can be effectively employed using either the dismembered or Foley YV plasty technique.
Footnotes
Author Disclosure Statement
No competing financial interests exist.