
Abstract
Background and Purpose:
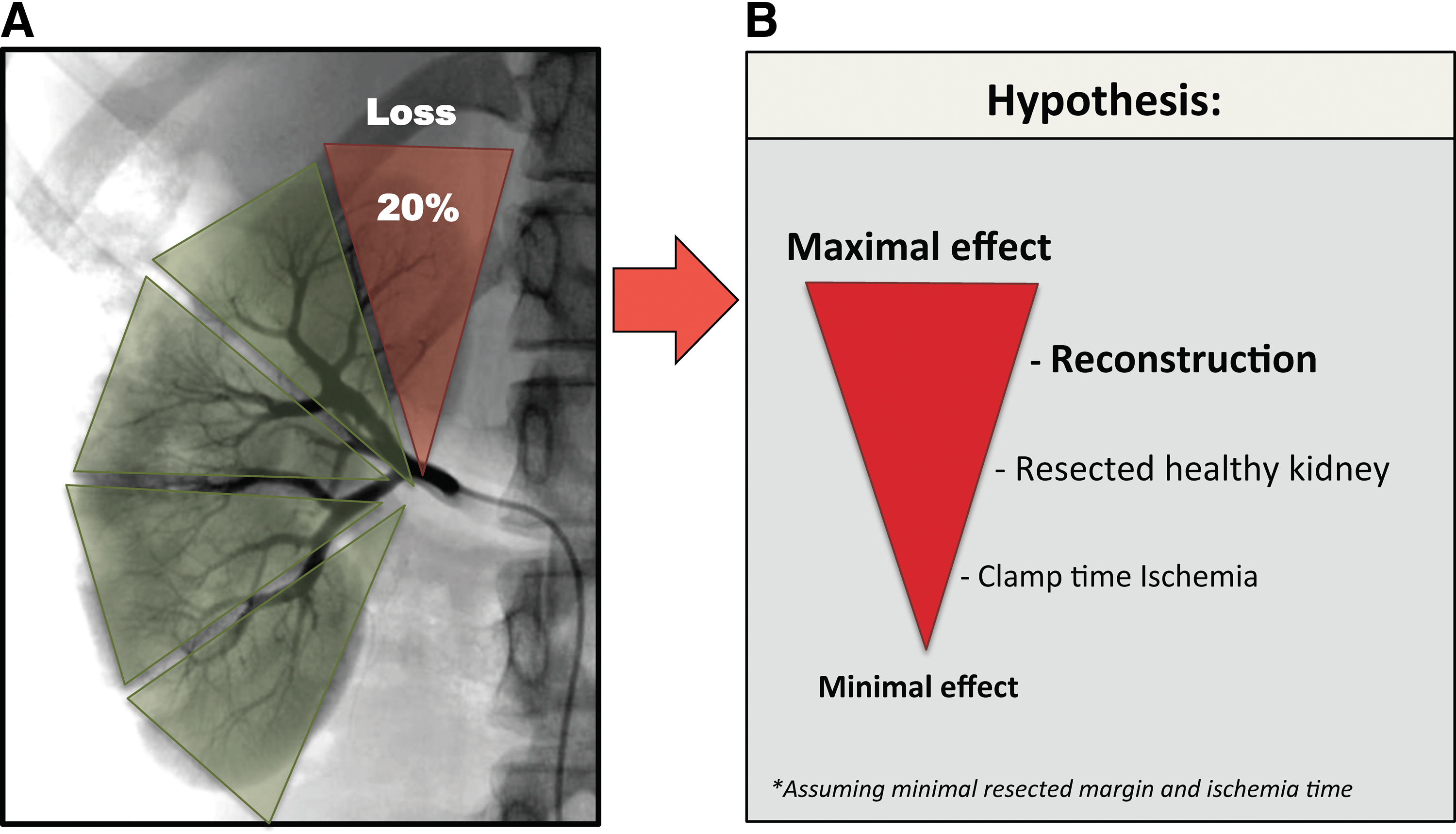
Functional losses near 20% are seen in the operated kidney during partial nephrectomy. Resected healthy margins are small and ischemia time limited in the modern era. We hypothesize that reconstruction following tumor resection is modifiable and a significant cause of renal function injury.
Materials and Methods:
A literature review of Medline and Scopus was performed for all available dates focusing on partial nephrectomy, renal function, and renal reconstruction. An additional review was performed evaluating recent advances in biomarkers of acute kidney injury.
Results:
Serum creatinine is of limited value in measuring renal preservation during partial nephrectomy. Stimulated glomerular filtration rate can estimate renal reserve, but is more difficult to measure. CT-based three-dimensional measurements provide the ability to isolate ipsilateral functional loss. Newer urinary biomarkers of acute kidney injury such as kidney injury molecule-1 and cell cycle markers are emerging and might help to quantify renal function loss in real time. Most prior research has focused on ischemia and enucleation. However, despite minimizing both, significant renal function losses are still seen. Four retrospective controlled studies were found comparing cortical renorrhaphy to omission of cortical renorrhaphy. Three of the four found a statistical benefit to nonrenorrhaphy with the range of volume or functional loss in those three being 3.8% to 11.5% vs 15.6% to 20.4%. Urine leaks and bleeding complications were similar to reported rates for both groups.
Conclusion:
Studies evaluating renal function preservation after partial nephrectomy should control for reconstructive injury in addition to ischemia time and resected healthy margin. Cortical renorrhaphy is associated with renal volume and functional loss on retrospective studies, which might be especially relevant in the setting of chronic kidney disease or solitary kidney. Newer biomarkers of renal injury should be used when studying predictors of renal injury.
Introduction
S
In addition to resected healthy margin, ischemia time and reconstructive injury (renorrhaphy) have been suggested to cause renal function loss during partial nephrectomy. 6 Resection and ischemia time have been studied extensively as they are often considered more “modifiable” than reconstruction. Global ischemia by hilar clamping is referred to as ischemia time. Local or regional ischemia due to ligation of segmental vessels and their arterial branches during renorrhaphy has rarely been studied. To truly be considered “zero ischemia,” both global (clamp) and regional (renorrhaphy) ischemia need to be avoided. We hypothesize that reconstruction is modifiable and potentially the leading cause of renal function injury in the modern era where warm ischemia time (WIT) and resection margin are limited (Fig. 1). Our goal is to review recent studies assessing the effect of renorrhaphy on renal function after partial nephrectomy.
Materials and Methods
A literature search was performed in Medline for all available dates looking for reconstruction-related renal injury during partial nephrectomy using the search terms “‘partial nephrectomy’ AND renal function AND renorrhaphy OR reconstruction.” A similar search was made for resection-related injury using “‘partial nephrectomy’ AND renal function AND resection OR margin OR enucleation.” A search was also made for ischemic-related injury using “‘partial nephrectomy’ AND renal function AND ischemia.” All searches were done on or before January 13, 2016. The total number of articles was noted for each search, and the results for reconstruction-related injury were to assess for inclusion in this review. Additional searches were performed in Scopus and The Cochrane Library.
Results and Discussion
Measuring renal preservation
Serum creatinine is inexpensive and easy to measure, but of limited value in measuring renal preservation after partial nephrectomy. The primary challenge in using creatinine is renal reserve. For example, creatinine-based glomerular filtration rate (GFR) for a healthy kidney donor does not drop by 50% after nephrectomy, but closer to 30% demonstrating the use of renal reserve in the solitary kidney. 7 One way to measure renal reserve is by performing a stimulated GFR measurement. This could be considered a kidney stress test wherein creatinine measurement follows an oral protein load or amino acid infusion. 8 A recent study found stimulated GFR in healthy subjects was 23% higher than baseline GFR, but for a subject with chronic kidney disease stage 3 the renal reserve was only 8.9%. 9 Therefore, serum creatinine changes should be viewed as a poor indicator of loss in GFR.
Recently, CT-based three-dimensional measurements have been used to calculate volume loss between preoperative and postoperative loss. This volume loss has been used as a proxy for renal functional loss. Interestingly, in partial nephrectomy studies, the contralateral kidney demonstrates minimal increase in volume supporting the use of volume loss in the ipsilateral kidney. 10 However, in radical nephrectomy series, the contralateral volume increase is dramatic. This brings into question the ability of volume-based measurements to accurately measure loss in the setting of a solitary kidney where physiologic hypertrophic changes could mask surgery-related volume losses. 11
Newer markers of acute kidney injury could improve partial nephrectomy study designs. 12 Kidney injury molecule-1 (KIM-1) mRNA is found in urine after ischemic and nephrotoxic injury and has been shown to outperform serum creatinine in rat models. 13 KIM-1 was correlated with end-stage renal disease in a recent study in humans. 14 Two cell cycle arrest biomarkers (tissue inhibitor of metalloproteinases-2 and insulin-like growth factor binding protein 7) have been shown to predict imminent risk of acute kidney injury. 15 The cell cycle arrest biomarkers also showed the ability to predict acute kidney injury and death in a high-risk surgical group. 16
Emphasis on clamp time
The study of ischemic injury during partial nephrectomy has dominated the research literature as witnessed by nearly 60% of all articles being in the ischemia category (Fig. 2) on a recent PubMed search (see Materials and Methods section). A recently published partial nephrectomy series demonstrates the emphasis on WIT. 17 The authors observed a nonlinear drop in WIT that was felt to be primarily due to stricter goals. For example, before 2010 a goal of 30 minutes was used, and the average WIT was ∼25 minutes. However, within 10 months the publication of a study entitled “every minute counts” 18 the average WIT was below 20 minutes. The WIT decreased despite increasing size and complexity of tumors.
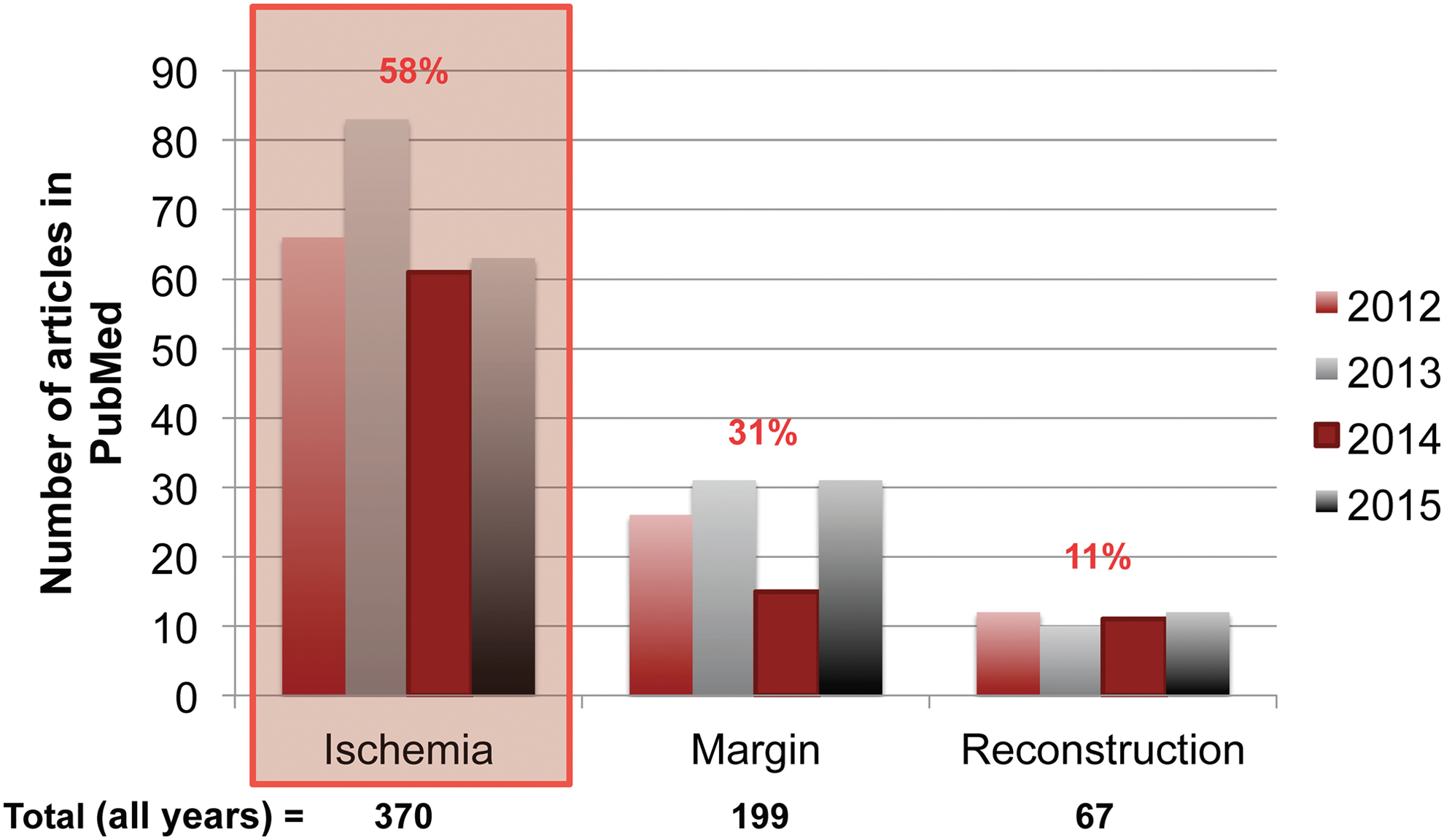
Results of a recent PubMed search using search terms for ischemic injury, enucleation/margin, or reconstruction/renorrhaphy are shown. Color images available online at
Studies have questioned the role of WIT in the modern era with short ischemia times and the inclusion of volume loss into adjusted analyses. 19 In addition, partial nephrectomy studies have demonstrated minimal atrophy after WIT. Funahashi and colleagues 20 showed 0% atrophy with WIT <25 using nuclear function studies, and Zhang and colleagues 21 showed 1% atrophy with a median WIT of 21 minutes when measuring parenchymal thickness on the pole opposite the resection site leading the authors to conclude that every nephron counts rather than every minute counts.
Ischemic injury is difficult to quantify because ischemia time is a proxy for tumor complexity. That is, as the tumor becomes larger and more complex (central/endophytic), it takes longer to resect and reconstruct, thus increasing the ischemia time. Tumor complexity is most likely the driver of renal function loss. Therefore, ischemia time meets the definition of a confounding factor in that it is correlated both with tumor complexity (independent) and renal function (dependent). Numerous systems have been devised such as RENAL Nephrometry, PADUA, C-Index, and tumor contact surface area to measure tumor complexity, but it is still difficult to adequately quantify and control for tumor complexity.
Measuring resected margin
The acceptable healthy margin during partial nephrectomy resection continues to decrease. In 2002, Sutherland and colleagues 22 challenged the 1 cm safety margin when they reported no local recurrences in 41 cases with a median safety margin of 0.2 cm. More recently, enucleoresection has grown in interest as a means of preserving renal function and minimizing complications. However, the technique for reconstruction is often not controlled for during studies of enucleoresection. For example, Durso and colleagues 23 compared healthy margin resection to enucleoresection during partial nephrectomy with volume loss as the primary outcome. They reported improved volume loss with enucleoresection, but did not comment on reconstruction techniques. Reconstruction was likely unbalanced as different surgeons contributed to the two surgical arms.
Enucleoresection is likely associated with a less aggressive reconstructive technique as the depth of resection into the renal sinus is less and blood vessels are often controlled as they are encountered. For example, Mukkamala and colleagues 24 found a decreased incidence of entry into the renal sinus (21% vs 41%) and decreased tumor bed suturing (41% vs 62%) in enucleoresection compared with sharp excision. They failed to show a functional benefit for the enucleoresection group, but did show similar safety and oncologic outcomes.
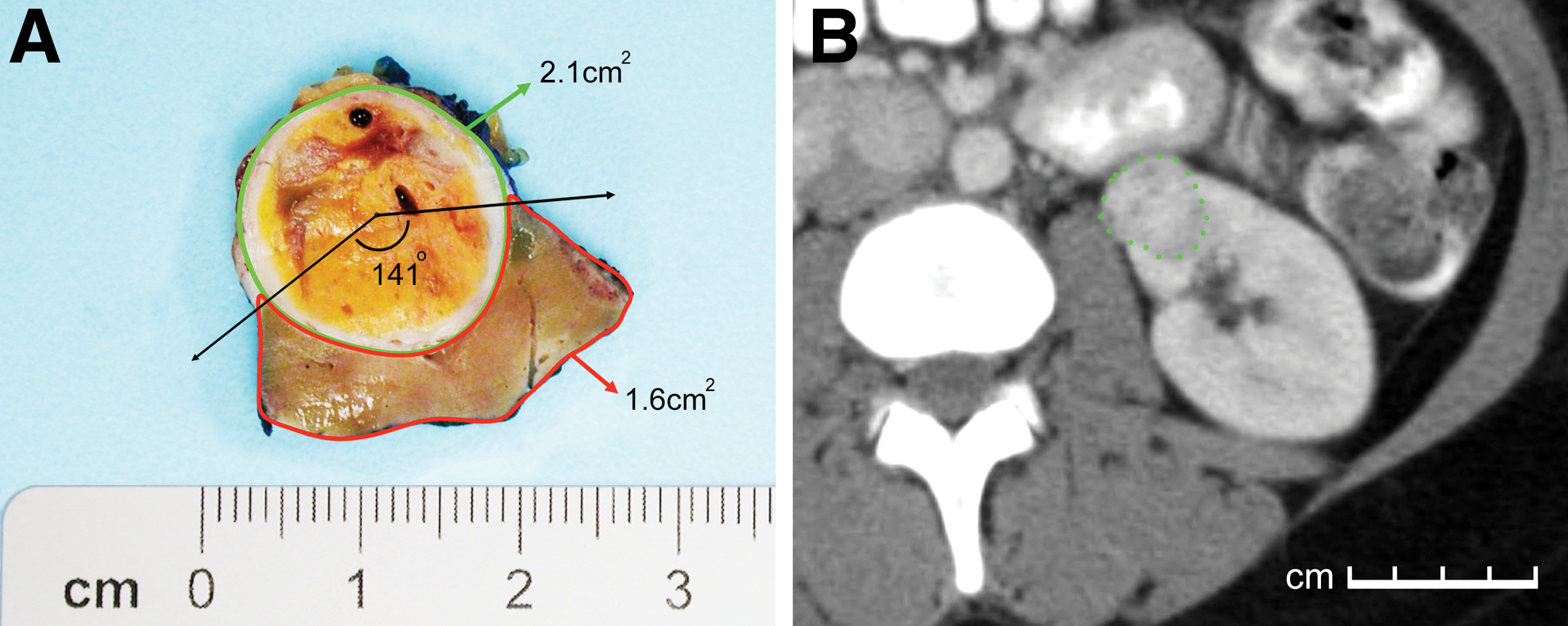
The amount of healthy renal parenchyma resected can be quantified by whole mount analysis of the resected tumor or estimation from a single photo of the resected tumor. An unpublished series of 25 whole mounts demonstrated a median healthy margin length of 5.5 mm and a median volume of resected healthy margin of 9.7 cm3. The median tumor diameter was 3.2 cm in the series. By using a single photo at the greatest diameter and an equation described previously, 25 the volume of resected healthy margin was calculated at 8.1 cm3 and the Pearson correlation between the whole mount and single photo technique was 0.89 (Fig. 3).
Comparing renorrhaphy to nonrenorrhaphy
Multiple small retrospective controlled studies show a benefit in renal function and volume preservation when omitting cortical renorrhaphy both in open and robotic partial nephrectomy. Hidas and colleagues 26 showed improved renal function loss on renal nuclear scan when omitting cortical renorrhaphy during partial nephrectomy (11.5% vs 20.4%, p = 0.02). Cortical renorrhaphy was replaced with tissue adhesive in 24 cases and compared with 32 cases with cortical renorrhaphy. A single surgeon performed all cases by an open approach. All cases had preoperative and postoperative quantitative SPECT measurement of DMSA. Tumor diameter was similar between the sealant group (3.6 cm) and the renorrhaphy group (3.4 cm), while cold ischemia time was shorter in the sealant group (19 minutes vs 29 minutes, p = 0.02).
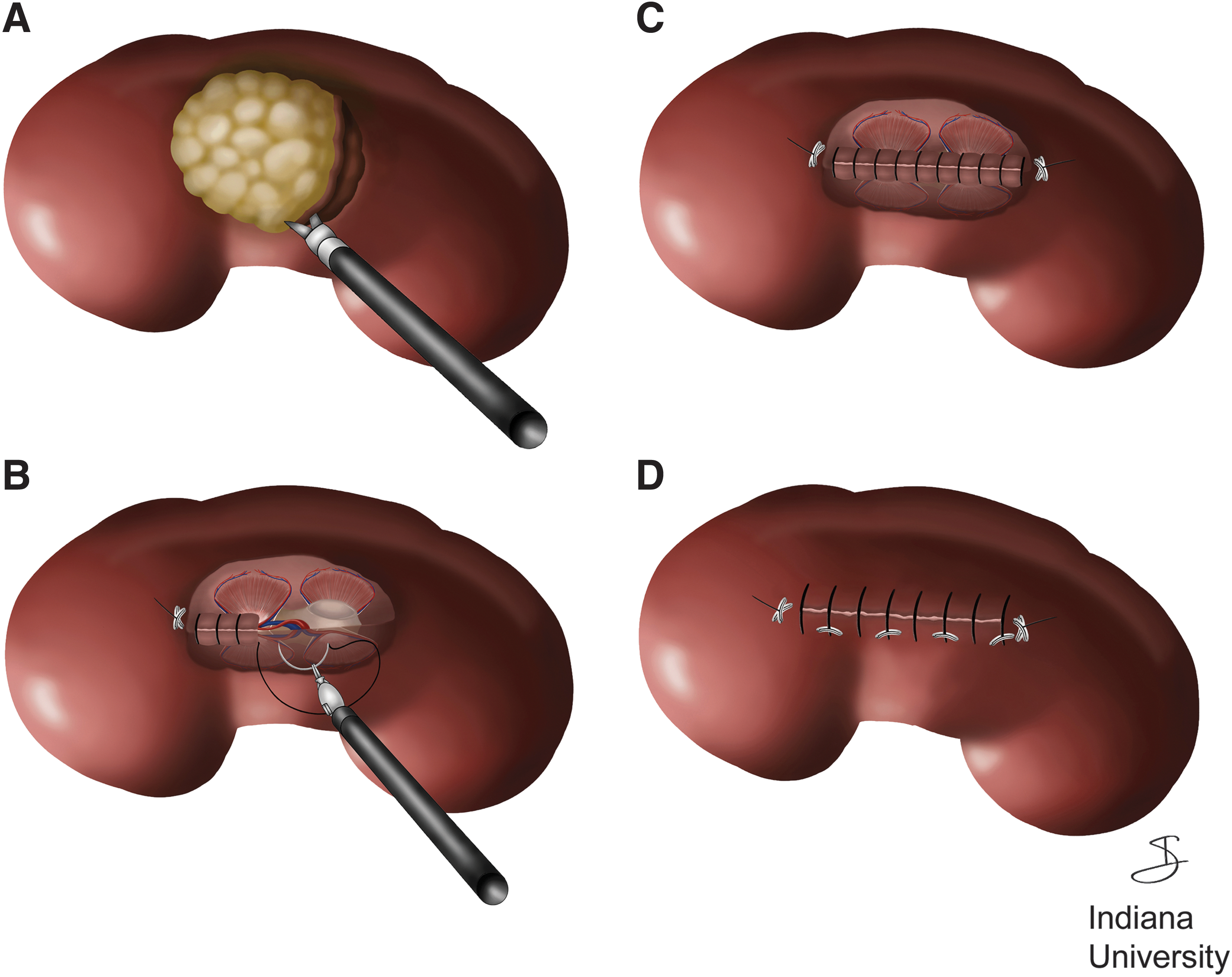
A more recent study had similar findings when comparing robotic base layer only (n = 15) to robotic base and cortical renorrhaphy (n = 30) for a single surgeon. 25 The base layer only group utilized a running base layer suture to ligate blood vessels before unclamping the renal hilum (Fig. 4). The cortical renorrhaphy group utilized a running sliding clip renorrhaphy technique. The cases were matched 1:2 by RENAL nephrometry scores. The %volume loss was improved for the base layer only group (9% vs 17%, p = 0.003). There was one pseudoaneurysm in the cortical renorrhaphy group and no urine leaks in the study. Three-dimensional models of the three largest %volume losses can be seen in Figure 5.
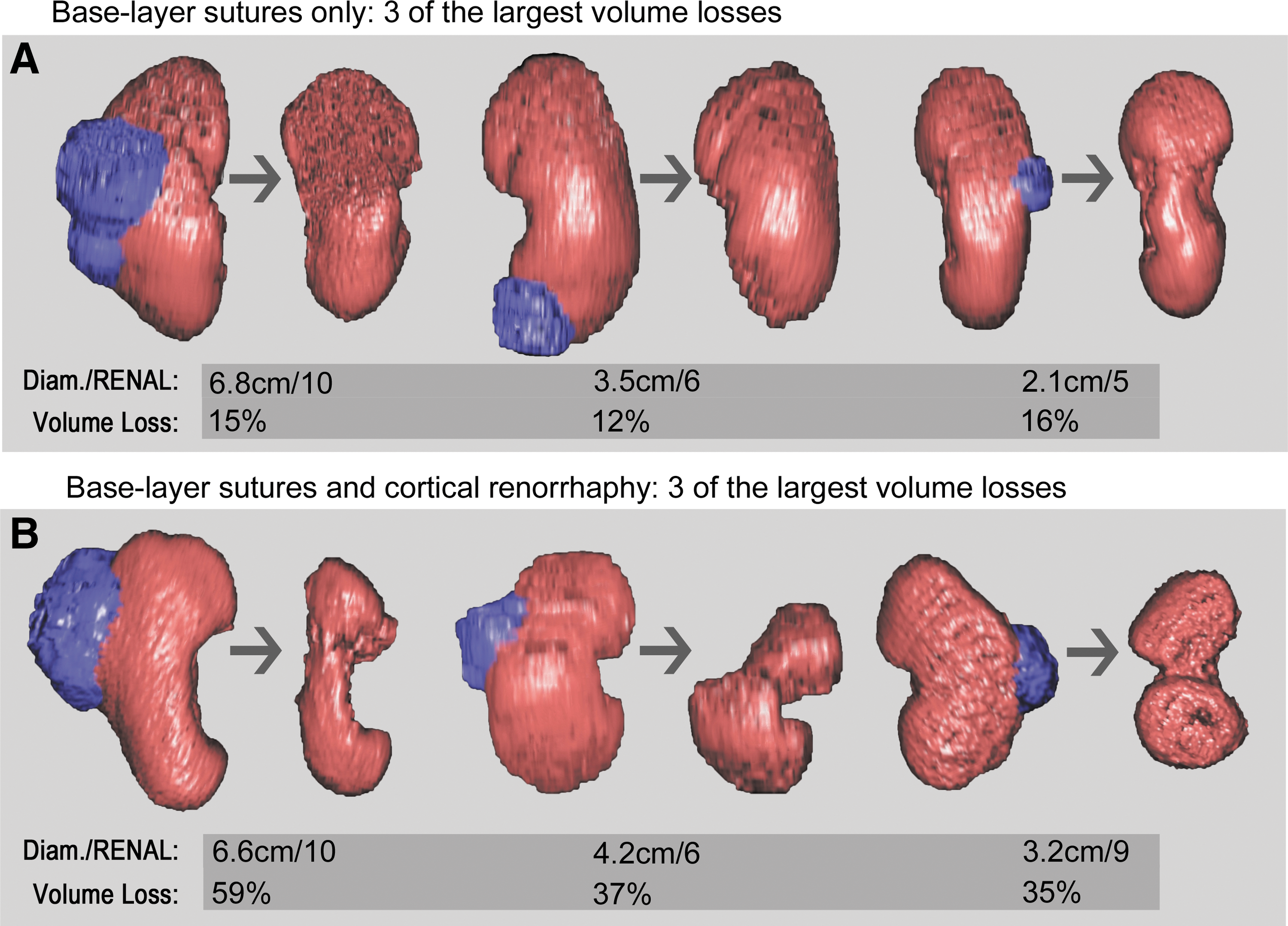
The preoperative and postoperative kidney models are shown for the three largest %volume losses for both
Another study showing a benefit to nonrenorrhaphy partial nephrectomy compared 38 nonrenorrhaphy cases to 118 renorrhaphy cases. 27 CT scans were available both preoperatively and at a mean of 8 months to calculate ipsilateral volume loss. The nonrenorrhaphy group showed improved volume loss (3.8% vs 15.6%, p < 0.001) and GFR loss (2.4% vs 8.9%, p = 0.03). Presence of renorrhaphy continued to be a predictor of volume loss on multivariable analysis (p < 0.001) and after propensity score analysis (p = 0.004). One weakness of the study was that nonrenorrhaphy cases were performed only by an open approach, while the renorrhaphy cases included both robotic and open. In addition, the ischemia time was longer in the renorrhaphy group, but ischemia time was not a predictor of %volume loss on multivariable analysis. The nonrenorrhaphy technique had two urine leaks and two bleeding complications compared with two and three for the renorrhaphy group.
In contrast, Takagi and colleagues 28 did not find a volume preservation benefit to nonrenorrhaphy when evaluating ≥T1b tumors operated on by an open approach. Cold ischemia was extended in both groups and longer in the renorrhaphy group (52 minutes vs 42 minutes, p = 0.02). The %volume loss was similar between nonrenorrhaphy (30%) and renorrhaphy (29%). The nonrenorrhaphy approach utilized soft coagulation rather than suture ligation. The authors discussed excessive coagulation as a possible cause for the lack of improvement in function. The nonrenorrhaphy group had two pseudoaneurysms and five urine leaks compared with two and two for the renorrhaphy group, respectively.
Conclusion
Studies evaluating renal function preservation after partial nephrectomy should control for reconstructive injury in addition to ischemia time and resected healthy margin. Cortical renorrhaphy is associated with renal volume and functional loss on retrospective studies and should be viewed as modifiable with either the open or robotic approaches. Minimizing or omitting cortical renorrhaphy is especially relevant in the setting of chronic kidney disease or solitary kidney. Newer biomarkers of renal injury should be used when studying predictors of renal injury.
Footnotes
Author Disclosure Statement
No competing financial interests exist.