
Abstract
Introduction and Objectives:
Computed tomography (CT) is one of the most commonly used diagnostic modalities for urinary stone disease. In this study we developed a CT and clinical parameter-based prediction model for shockwave lithotripsy (SWL) outcome in proximal ureteral stones.
Materials and Methods:
Data from 223 patients with single proximal ureteral stones treated with SWL between January 2009 and January 2015 were reviewed retrospectively. Clinical parameters including age, sex, body weight, and body mass index (BMI) were analyzed in combination with stone-related CT parameters (stone diameter, height, volume, location, Hounsfield units [HU], stone-to-skin distance [SSD]), and secondary signs (hydronephrosis, perinephric edema, and rim sign). Based on the cutoff values determined by c-statistics, a scoring system for the prediction of SWL outcome was developed.
Results:
The success rate was 65.9% (147/223), and in a univariate analysis body weight, BMI, SSD (vertical, horizontal), HU, stone diameter, height, volume, and all secondary signs were significantly associated with the success of SWL. However, on multivariate analysis only BMI (odds ratio [OR] = 1.322, confidence interval [CI] 1.156, 1.512, p = 0.00), stone diameter (OR = 1.397, CI 1.259, 1.551, p = 0.00), and perinephric edema (grade 0–1 vs 3–4, OR = 2.831, CI 1.032, 7.764, p = 0.043) were independent predictors of SWL success. The prediction model based on the logistic regression analysis was as follows: SWL success = 1/[1 + exp (−10.165 + 0.279 × [BMI] + 0.334 × [diameter] + 1.040 [perinephric edema])], having an area under the curve of 0.881. In the prediction model based on these parameters, scores of 0, 1, 2, and 3 correlated with SWL success rates of 98.5%, 65.7%, 31.4%, and 0%, respectively.
Conclusions:
BMI, stone diameter, and perinephric edema were independent predictors of SWL outcome and a prediction model based on these parameters will facilitate decision-making for SWL in proximal ureteral stones.
Introduction
S
In this study, we investigated the prognostic value of various anthropological and stone-related parameters on computed tomography (CT) images for the success of SWL of proximal ureteral stones. Also, based on the parameters whose significance was confirmed by logistic regression, we established a predictive model and scoring system for successful disintegration of proximal ureteral stones by SWL.
Materials and Methods
We retrospectively reviewed the medical records of 745 consecutive patients treated by SWL for ureteral stones between January 2009 and January 2015. Inclusion criteria included unilateral single proximal ureteral stone, CT scan performed in 1 week before SWL, and stone without any history of stone-related operation or concomitant medical expulsive therapy. According to the above criteria, 223 patients were included in the final dataset.
All patients were imaged with a 64-channel unenhanced helical computed tomography system (Brilliance CT; Philips Healthcare, Cleveland, OH). Dimensions were measured using electronic calipers on CT images, and volumetric stone burden (VSB) was defined as D 2 × H × 5 mm × π × 1/6 in which D = the longest transverse diameter and H = stone height (number of axial cut images of the stone, slice thickness = 5 mm). 5 Estimated stone location was defined as the number of axial cut images from the uretero-vesical junction to the lowest edge of the stone (slice thickness = 5 mm). 5 Skin-to-stone distance (SSD) was measured as described by Pareek et al. 6 Rim sign on CT images was graded as described previously (Fig. 1A, B; 0 = absent, 1 = soft tissue attenuation <2 mm, grade 2 = soft tissue attenuation between grade 1 and 2, and 3 = soft tissue attenuation of 4 mm in diameter). 5 Perinephric edema was defined as follows (Fig. 1C, D; 0 = absent, 1 = 1 or 2 small pockets of fluid <1 cm in diameter, 2 = fluid collection of grade 1–3, and 3 = >2 large pockets of fluid ≥1 cm in diameter). 5 Hydronephrosis was classified as reported previously (Fig. 1E, F; 0 = absent, 1 = prominence of the intrarenal pelvis or mild ureteral dilatation, 2 = dilatation of the renal calices or moderate ureteral dilatation, and 3 = severe dilatation of the collecting system). 5

Representative pictures of rim sign [
All stones were treated with an electroconductive-type Sonolith Praktis lithotripter (EDAP TMS, Lyon, France) under intermittent fluoroscopic guidance. A maximum of 3000 shocks was applied in each session or until complete disintegration of the stone. Failure of stone disintegration was defined as the presence of stone fragments larger than 3 mm on plain abdominal radiography after three sessions of SWL.
Student's t-test and a chi-squared test were used for inter-group comparisons and Pearson's correlation analysis was conducted to identify relationships between two variables. Logistic regression was performed to identify predictors of stone disintegration by SWL and to develop models for the prediction of SWL outcome. The predictive probability of each equation was assessed by calculating area under the curve (AUC) of receiver operator characteristic (ROC) curves. All values are expressed as mean ± standard deviation and p < 0.05 was considered to indicate statistical significance. For the statistical analysis, SPSS ver. 20.0 (IBM Corp, Armonk, NY) was used.
Results
The overall success rate of stone disintegration was 65.9% (n = 147). The mean age of the patients was 51.3 ± 15.2 years and there were no significant differences in age and male to female ratio between the disintegration success group (group 1) and the failure group (group 2). The mean body weight and body mass index (BMI) of patients in group 1 were 62.6 ± 11.8 kg and 23.5 ± 2.8 kg/m2, respectively, and were significantly lower compared to those of group 2 (68.5 ± 11.7 kg and 25.2 ± 3.3 kg/m2 respectively, p = 0.00, Table 1).
Data are presented as the mean ± SD.
Significant difference between success and failure group.
BMI = body mass index.
Stone diameter (p = 0.00), stone height (p = 0.006), SSD (vertical [p = 0.025], horizontal [p = 0.01]), HU (p = 0.001), hydronephrosis (grade 2 vs 3, p = 0.002), perinephric edema (grade 0–1 vs 2–3, p = 0.00; grade 1–2 vs 3, p = 0.001), and rim sign (grade 0–2 vs 3, p = 0.028) showed significant differences in SWL success rate between the two groups (Table 2).
Data are presented as the mean ± SD.
Significant difference between success and failure group.
ESL = estimated stone length; VSB = volumetric stone burden; SSD = skin-to-stone distance; HU = Hounsfield unit; SD = standard deviation.
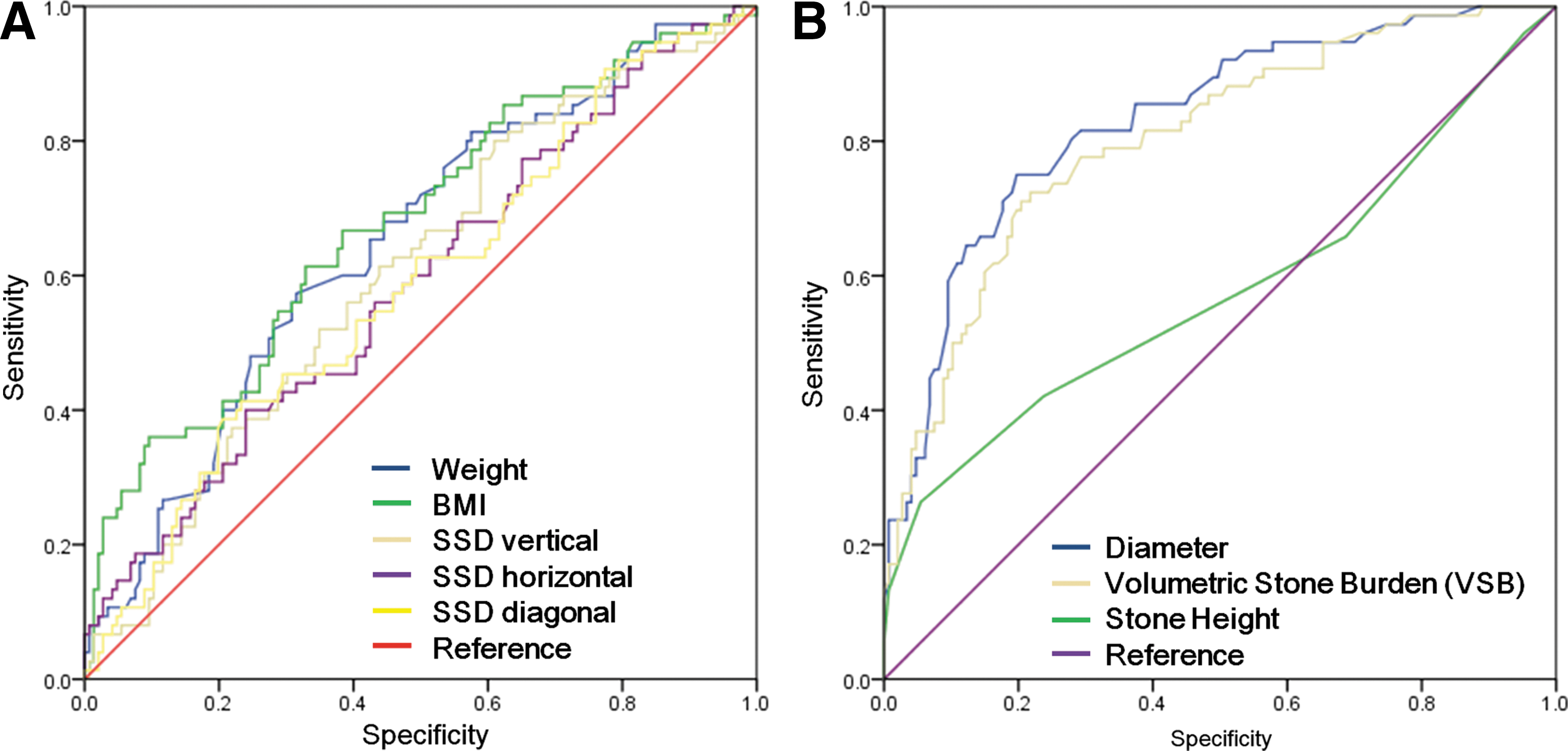
Because body weight, BMI, and SSDs reflect the distance between electrode of SWL (F1) and stone (F2) and showed a strong correlation (r = 0.518–0.822, p = 0.00, Table 2) with possible multicollinearity, only BMI was included in the multivariate analysis. BMI had a larger AUC (0.675) than body weight (AUC 0.648), SSD vertical (AUC 0.604), SSD horizontal (AUC 0.587), and SSD diagonal (AUC 0.586) according to c-statistics (Fig. 2A). For the same reason we used only stone diameter—which had a larger AUC (0.832) than other stone burden-related parameters including stone height (AUC 0.586) and VSB (AUC 0.804)—was used in the multivariate analysis (Table 3; Fig. 2B). Multivariate logistic regression analysis showed that BMI (odds ratio [OR] = 1.322, confidence interval [CI] 1.156, 1.512, p = 0.00), stone diameter (OR = 1.397, CI 1.259, 1.551, p = 0.00), and perinephric edema (grade 0–1 vs 3–4, OR = 2.831, CI 1.032, 7.764, p = 0.043) were independent predictors of successful stone disintegration by SWL (Table 4, upper panel). Because c-statistics suggested cutoff values of 7 mm (diameter) and 650 (HU) for differentiating group 1 from group 2 with the highest sensitivity and specificity, we dichotomized these two variables using the corresponding cutoff values and performed a multivariate analysis. BMI (OR = 1.265, CI 1.113, 1.438, p = 0.00), stone diameter (OR = 10.825, CI 5.308, 22.076, p = 0.00), and perinephric edema (OR = 3.520, CI 1.409, 8.797, p = 0.007) were found to be independent predictors of stone disintegration (Table 4, lower panel). The predictive model for successful stone disintegration based on these variables was as follows: stone disintegration rate = 1/[1 + exp (−10.165 + 0.279 × [BMI] + 0.334 × [diameter] + 1.040 [perinephric edema])] when continuous values of stone diameter and HU were used. In contrast, when dichotomized stone diameter (≥7 mm vs <7 mm) and HU (≥650 vs <650) values were used the predictive model was as follows: stone disintegration rate = 1/[1 + exp (−7.869 + 0.235 × [BMI] + 2.382 × [diameter] + 1.259 [perinephric edema])]. The area under ROC curve for each model was 0.881 and 0.761, respectively (Fig. 3).
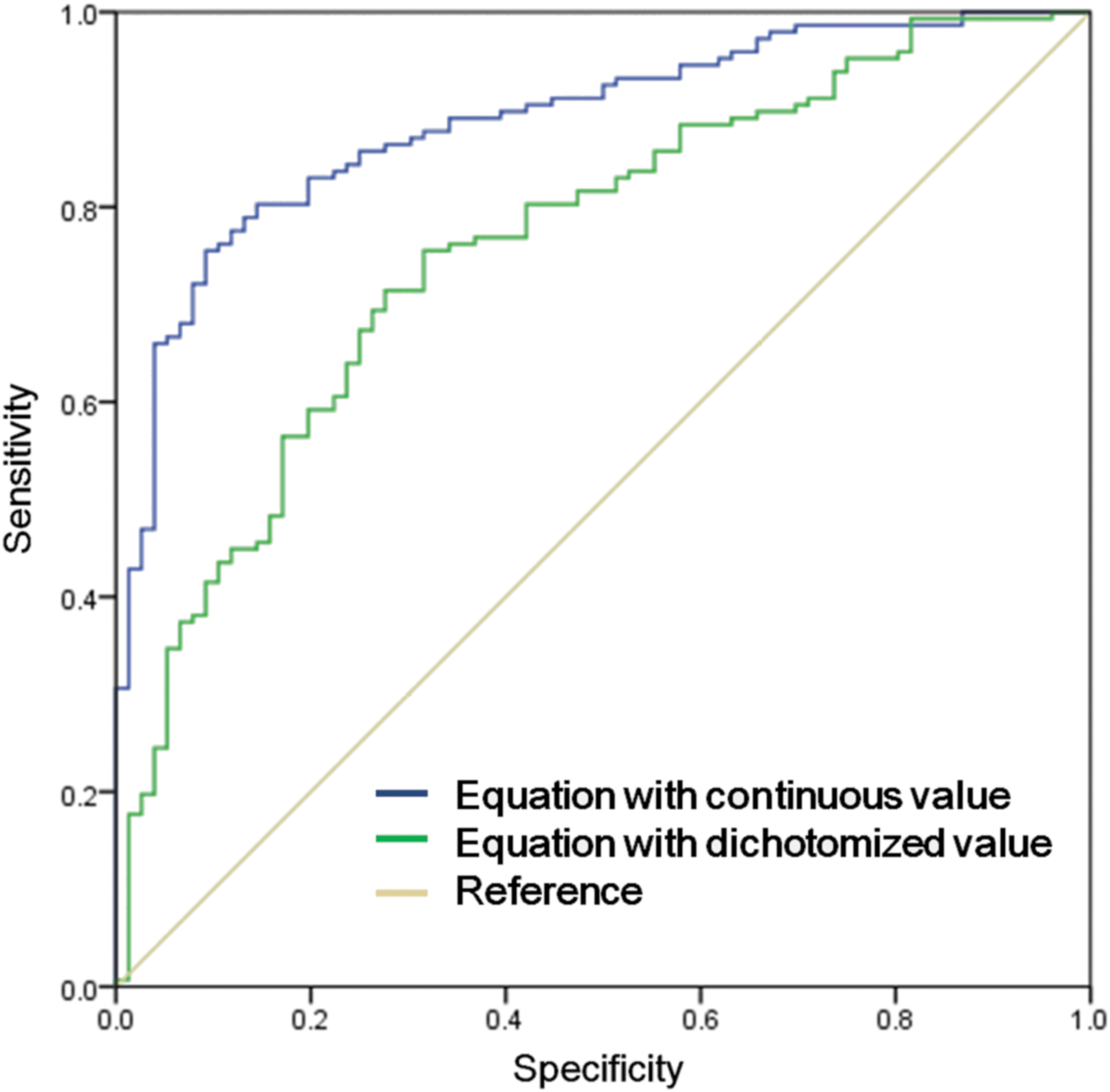
ROC curve of equations for three variables (BMI, stone diameter, and perinephric edema) for the probability of complete stone disintegration. The AUC of the combined variables was 0.888, compared to 0.761 for dichotomized variables (BMI <25 kg/m2 vs ≥25 kg/m2; and stone diameter <7 mm vs ≥7 mm).
r = correlation coefficient.
BW = body weight.
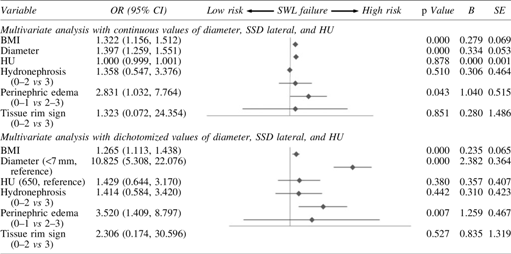
OR = odds ratio; CI = confidence interval; β = coefficient of regression; SE = standard error.
When cutoff values of 7 mm (stone diameter), ≥grade 2 (perinephric edema) and ≥25 kg/m2 (BMI) were used to calculate score based on the number of cutoff values a stone fell below, the success rate of stone disintegration for scores of 0, 1, 2, and 3 were 98.5%, 65.7%, 31.4%, and 0%, respectively (Table 5).
Discussion
Recent advances in endoscope technologies and intracorporeal lithotripsy equipment have broadened the indications of URSL, which is superior to SWL for almost all of the urinary tract from the kidney to the distal ureter. 7,8 For example, according to a meta-analysis performed in 2007 by the joint EAU and AUA Nephrolithiasis Guideline Panel, the stone-free rate of URSL is superior or at least comparable to that of SWL for stones at all ureteral segments, with the exception of proximal ureteral stones <10 mm in size. 9 It was also reported that a stone-free rate of 68% after the first treatment with SWL decreases markedly to 46% and 31% in the second and third sessions, respectively. 10 Thus, it is clinically important to identify patients with ureteral stones who have a high probability of achieving a stone-free status by SWL.
Currently, CT is one of the most frequently used imaging modalities for the diagnosis of urolithiasis and provides greater patient- and stone-related information compared with conventional radiographs, such as kidney, ureter, and bladder radiograph and intravenous pyelogram. Thus, many studies of the use of CT-related parameters as predictors of successful treatment of urolithiasis have been conducted. 11 –16 In this study we analyzed predictors of successful SWL of ureteral stones using clinical and CT-related parameters while limiting the cohort to patients with solitary proximal ureteral stones, in which SWLs has an efficacy comparable to URLS.
The results of our analysis with stone size (diameter, stone height, and VSB) and density (HU) are in agreement with previous reports of significant differences in stone size-related parameters and HU between SWL success and failure groups. 11,13,17 –21 Because all size-related parameters had high correlations with each other (Table 3), to avoid the problem of multicollinearity between these parameters, we included only transverse diameter in the multivariate analysis, as this showed the largest AUC of the three parameters as determined using c-statistics (Fig. 2B). Because c-statistics showed that 7 mm was the cutoff value of stone diameter with the optimal sensitivity and specificity for successful stone disintegration, we dichotomized patients into two groups based on stone diameter (≥7 mm vs <7 mm) and assessed the difference in stone disintegration rate between the two groups using multivariate analysis. Although univariate analysis showed that HU is a significant predictor of stone disintegration, as reported previously, in multivariate analysis we found no meaningful difference in HU between the success and failure groups. Because 650 HU was the optimum cutoff value and had the highest sensitivity and specificity on ROC analysis, we categorized patients into two groups according to stone HU value (≥650 mm vs <650 mm). However, there was no significant difference in stone disintegration rate between the two groups by multivariate analysis.
In our study, a univariate analysis showed that body weight, BMI, and SSD (vertical and horizontal) had a significant negative impact on stone disintegration rate, which is in agreement with prior reports of the influence of BMI and SSD on SWL. 22 However, the clinical significance of these factors in SWL is controversial. 23 For example, Pareek et al. 6 reported that SSD ≥10 cm is significantly related to SWL failure for lower pole renal stones and both BMI and HU are independent predictors of success in SWL. Weld et al. showed that SSD was a predictor of only calyceal stones, not for stones in the renal pelvis or the ureteropelvic junction. 6,24 Also, El-Nahas et al. found that SSD is a significant predictor of SWL success in a univariate but not multivariate analysis. 16 These variable results might be due to the different characteristics of the study cohort and the SWL machines and protocols used. However, another possible cause is interactions among these variables. Although the mechanism of the effects of BMI and SSD on the efficacy of SWL has not been fully elucidated, it is thought to be primarily due to alterations in the distance between electrode (F1) and stone (F2) and variations in intervening tissue composition, such as muscle and fat tissue, between two points. 16,25 –27 Thus, these parameters could be influenced by the co-factors that affect F1 to F2 distance and tissue composition, such as body weight and habitus, and so have a high probability of being correlated. To test this hypothesis we assessed the relationship between these parameters, and found relatively strong correlations among body weight, BMI, and SSD, as reported previously (Table 3). 28 Based on these findings we included only BMI, which had a higher AUC than body weight and SSD, in the multivariate analysis (Fig. 2A).
Secondary signs of ureteral stones have been reported to be associated with a higher likelihood of the presence of underlying ureteral lesions such as ureteral stricture, ureteral polyp, and submucosal stone thus having a significant influence on the outcome of SWL or URSL. 5,29,30 In this study, on univariate analysis all secondary signs on CT images—including hydronephrosis, perinephric edema, and rim sign—were significantly associated with the outcome of SWL. However, in a multivariate analysis only perinephric edema (grade 0–1 vs 2–3) was an independent predictor of success of SWL. The perinephric edema defined as fluid collection in the perinephric space identified on CT images has been reported to be associated with spontaneous passage of urinary stone and success rate of URLS. 5,30,31 However, to the best of our knowledge this study constitutes the first report on the predictive role of perinephric edema for SWL outcome in proximal ureteral stone.
Recently, Tran et al. developed the Triple D Score based on CT-based parameters—such as stone volume, density, and SSD—and showed that this scoring system could be used for decision-making for SWL in renal and ureteral stones. 32 To develop this model, they first determined the optimum cutoff values of each parameter using an ROC curve (150 μL for stone volume, 600 HU for stone density, and 12 cm for SSD) and the calculated D score for each targeted stone based on whether the measured value of each parameter was lower or higher than the cutoff value. Then, the individual scores of the three parameters were integrated into a single score (Triple D score), which facilitated stratification of patient suitability for SWL. However, in their model the parameter selection procedure was not statistical but rather arbitrary. Also using the same cutoff value for each parameter such as SSD in both renal and ureteral stones might be controversial. In this study, we developed a similar scoring system that can be used for the prediction of successful disintegration of stones in the proximal ureter. As a first step we performed a correlation analysis and finally selected three parameters (BMI, stone diameter, and perinephric edema) with a minimal probability of multicollinearity. Also, we limited the application of these parameters to only proximal ureteral stones. Logistic regression analysis showed that the predictive model based on these three parameters had high predictive probability (AUC 0.825). Next, we developed a scoring system based on these three parameters in a similar way as the Triple D score. When cutoff values of 7 mm (stone diameter), ≥grade 2 (perinephric edema) and ≥25 kg/m2 (BMI) were used to calculate the total score, the success rate of stone disintegration for total scores of 0, 1, 2, and 3 were 98.5%, 65.7%, 31.4%, and 0%, respectively. These results suggest that other treatment options, such as URSL, should be strongly considered as the primary treatment modality in the presence of two or more positive parameters simultaneously (total score of 2 or 3), correlated with success rates of 31.4% and 0%.
Although this study yielded some promising results, it was not without limitations. The most important limitation concerns the definition of treatment failure as the presence of stone fragments after three sessions of SWL. As described previously, performing more than three sessions of SWL is not effective for stone disintegration and less cost-effective than URLS. Based on these findings, we limited the definition of success of SWL to the first three sessions. This means that some patients might have undergone further sessions of SWL and achieved complete stone disintegration. Another limitation of this study was limited number of SWL model (only electroconductive-type Sonolith Praktis lithotripter) tested, a problem inherent in the nature of single-center retrospective study. So we admit the possibility of different results when other brands or types of lithotripters were employed.
Conclusion
In conclusion, patient and CT-based parameters—including BMI, stone diameter, and perinephric edema—are independent predictors of the outcome of SWL of proximal ureteral stones. A scoring system based on these parameters enabled differentiation of patients likely to have favorable outcomes from those with low chances of complete stone disintegration, thus facilitating treatment planning in patients with proximal ureteral stones.
Footnotes
Author Disclosure Statement
No competing financial interest exist.