
Abstract
Purpose:
Pretreating a pig kidney with 500 low-energy shock waves (SWs) before delivering a clinical dose of SWs (2000 SWs, 24 kV, 120 SWs/min) has been shown to significantly reduce the size of the hemorrhagic lesion produced in that treated kidney, compared with a protocol without pretreatment. However, since the time available for patient care is limited, we wanted to determine if fewer pretreatment SWs could be used in this protocol. As such, we tested if pretreating with 300 SWs can initiate the same reduction in renal lesion size as has been observed with 500 SWs.
Materials and Methods:
Fifteen female farm pigs were placed in an unmodified Dornier HM-3 lithotripter, where the left kidney of each animal was targeted for lithotripsy treatment. The kidneys received 300 SWs at 12 kV (120 SWs/min) followed immediately by 2000 SWs at 24 kV (120 SWs/min) focused on the lower pole. These kidneys were compared with kidneys given a clinical dose of SWs with 500 SW pretreatment, and without pretreatment. Renal function was measured both before and after SW exposure, and lesion size analysis was performed to assess the volume of hemorrhagic tissue injury (% functional renal volume, FRV) created by the 300 SW pretreatment regimen.
Results:
Glomerular filtration rate fell significantly in the 300 SW pretreatment group by 1 hour after lithotripsy treatment. For most animals, low-energy pretreatment with 300 SWs significantly reduced the size of the hemorrhagic injury (to 0.8% ± 0.4%FRV) compared with the injury produced by a typical clinical dose of SWs.
Conclusions:
The results suggest that 300 pretreatment SWs in a voltage ramping treatment regimen can initiate a protective response in the majority of treated kidneys and significantly reduce tissue injury in our model of lithotripsy injury.
Introduction
P
As a practical matter, the time, which can be devoted to an individual patient's treatment, is limited and few urologists have the flexibility to adopt procedures that increase the length of time devoted to a lithotripsy session. Because of this limitation on time, we sought to identify other treatment protocols that would result in significant protection against SW injury while also limiting any increase in treatment duration. Toward this goal, we initiated a series of experiments using a pause-less voltage ramping treatment procedure. These experiments consisted of an initial dose of low-energy SWs (12 kV), followed immediately by a clinical dose of 2000 SWs at 24 kV with all SWs being delivered at 120 SWs/min. 6
When we pretreated with only 100 low-energy SWs before a clinical SW dose, lesion size remained high and was similar to kidneys that did not receive pretreatment. However, when 500 low-energy pretreatment SWs were used, we observed a significant reduction in lesion size. 6 Using this information, we hypothesized that a threshold exists somewhere between 100 and 500 pretreatment SWs that would still produce protection from renal injury while further limiting treatment duration. In the present study, we chose to test 300 pretreatment SWs as the threshold value for initiating protection from injury since it represents the midpoint between 100 and 500 pretreatment SWs.
Materials and Methods
Extracorporeal shock wave lithotripsy experiment
The surgical and animal treatment protocols used to assess renal injury in this study were carried out in accordance with the National Institutes of Health Guide for the Care and Use of Laboratory Animals and were approved by the Institutional Animal Care and Use Committee of the Indiana University School of Medicine and Methodist Hospital. The design of the extracorporeal shock wave lithotripsy (SWL) experiment and all surgical procedures used during the experiment followed the same methods used in previously published studies. 6 –8
Fifteen female farm pigs, weighing ≈15 kg each (Hardin Farms, Danville, IN), were anesthetized, and each animal was placed in an unmodified Dornier HM-3 lithotripter (Dornier Medical Systems, Kennesaw, GA). A lower pole calix of the left kidney of each animal was targeted for lithotripsy treatment by retrograde infusion of X-ray contrast (Isovue-300; Bracco Diagnostics, Princeton, NJ) and imaging with the biplanar X-ray system of the HM-3. The targeted kidney received 300 SWs at 12 kV (120 SWs/min) followed immediately by 2000 SWs at 24 kV (120 SWs/min) focused on the lower pole of one kidney. There was a short 10-second pause between SW doses to allow time to increase the SW kV level from 12 to 24 kV.
Renal function was measured during the experiment and these functional assessments followed previously described protocols. 7 In brief, inulin and para-aminohippuric acid (PAH) were infused into the pigs and blood samples were taken from a femoral artery catheter. Timed urine collections were taken from catheters inserted into both ureters. Colorimetric assays were then used to measure the renal clearance of inulin, which was used to estimate glomerular filtration rate (GFR), and the renal clearance of PAH, which was used to estimate effective renal plasma flow (ERPF). Renal function measurements were taken both before and at 1 hour after SW treatment.
Lesion analysis
At the end of the experiment, the kidneys were perfusion-fixed in situ with 2.5% glutaraldehyde in 0.1 M cacodylate buffer (pH = 7.4). After the kidneys were removed, they were submerged in fresh fixative for subsequent determination of lesion size. Nine of the fifteen pigs underwent lesion size analysis where Microfil (Flow Tech, Inc., Carver, MA) was injected into the vasculature of the selected kidneys and the kidneys were dehydrated, embedded in paraffin, and then serially sectioned into 40 μm-thick slices. Digital photographs were taken of the slices every 120 μm. The hemorrhagic lesion observed in the sections was used to determine lesion volume and expressed as percent of the FRV of renal parenchyma for each kidney. 9 Mean lesion size ± SEM was calculated in the treated pigs and compared with lesion sizes produced in treatment groups that have been previously published (typical clinical treatment group and 500 SW pretreatment group). 6 Both of these groups were treated on the same Dornier HM-3 and the pigs used were of similar size as the animals in the present study.
Statistical analysis included paired t-tests used to compare measurements at baseline and at 1 hour after SW treatment. A Wilcoxon rank sum test was used to compare the lesion sizes between the SWL-treated groups. Two-sided P-values <0.05 were considered statistically significant.
Results
Pig body weights, kidney weights, baseline arterial blood pressures, and mean blood pressure change were similar between the groups (Table 1). GFR fell significantly in the 300 SW pretreatment group by 1 hour after lithotripsy treatment. A significant fall in GFR after SW treatment was also observed in animals receiving 500 pretreatment SWs and in animals without pretreatment (Fig. 1). ERPF, on the other hand, did not change significantly in the 300 SW pretreatment group (Fig. 2). We normally observe a fall in ERPF after SW treatment whether using low-energy pretreatment protocols or protocols without pretreatment. In this case, however, the posttreatment EPRF measurement was more variable than normal preventing us from reaching a significant difference when analyzed.
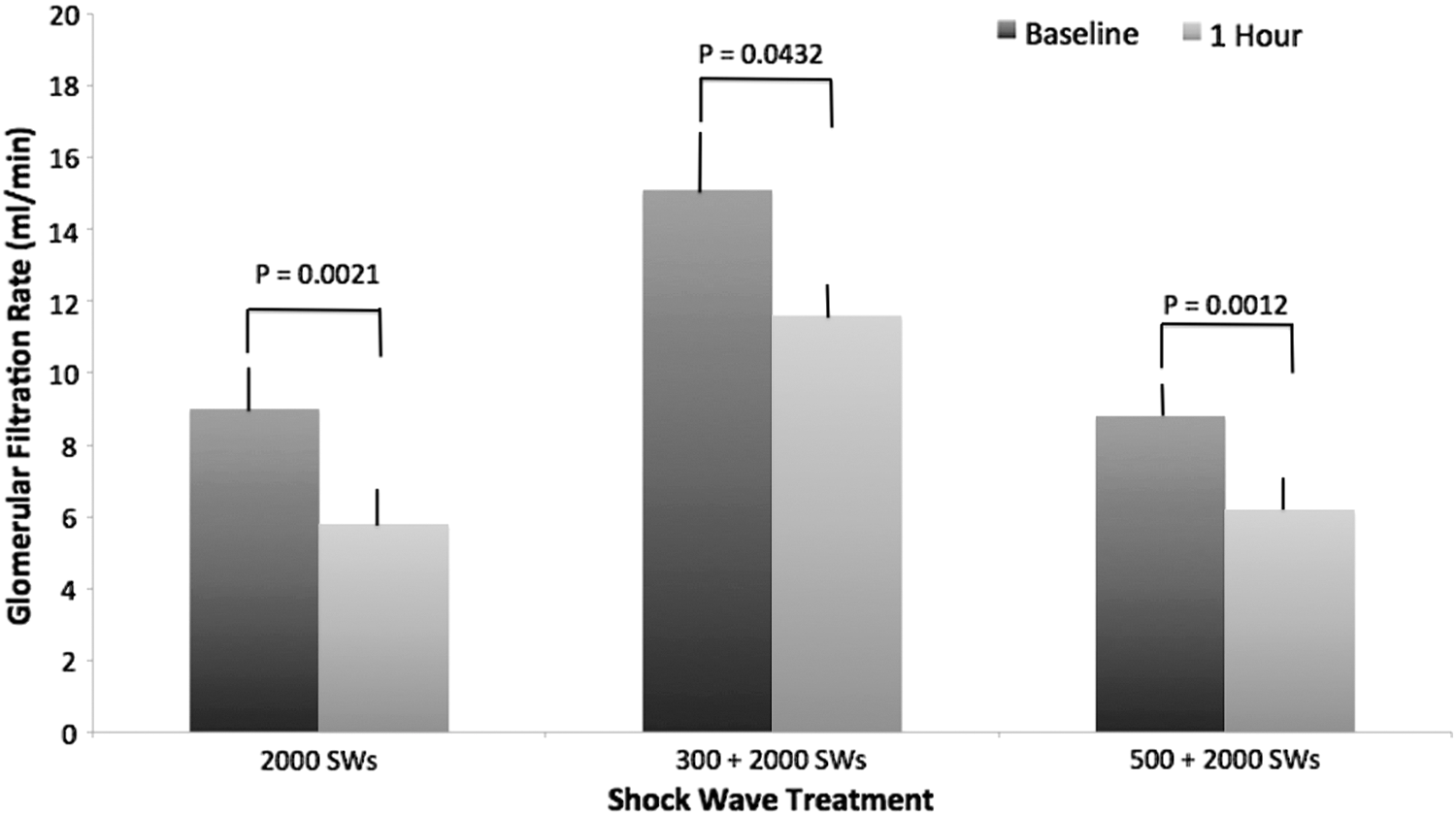
Bar graphs of GFR measured before and after lithotripsy from the different treatment groups. Values from the clinical treatment (2000 SWs) and 500 pretreatment SW groups were previously published. 6 In all cases, GFR fell significantly between baseline and 1-hour post treatment. GFR = glomerular filtration rate; SW = shock wave.
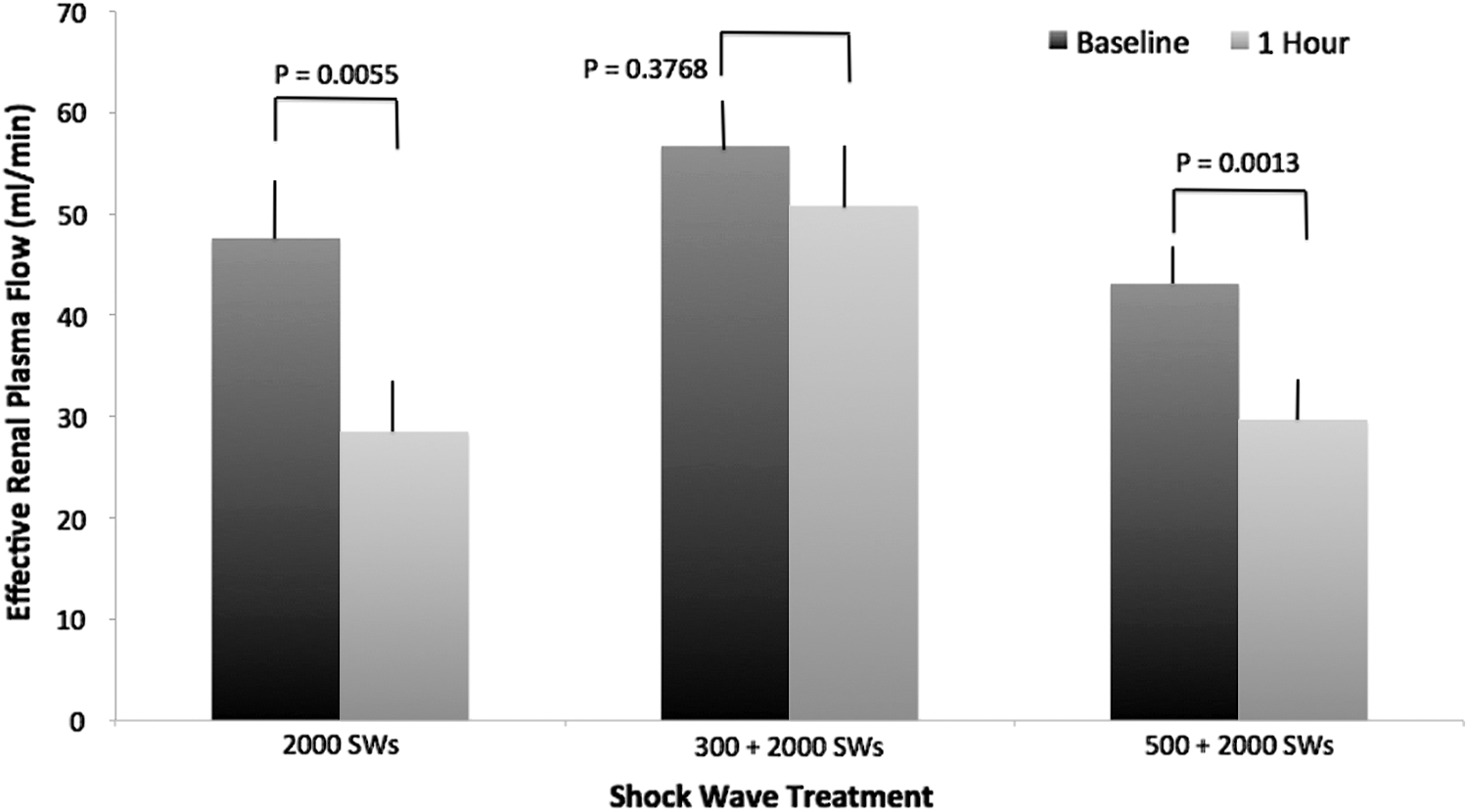
Bar graphs of ERPF measured before and after lithotripsy from the different treatment groups. Values from the clinical treatment (2000 SWs) and 500 pretreatment SW groups were previously published. 6 The change in ERPF was not significant in the 300 low-energy SW pretreatment group. The other groups did show a significant fall in plasma flow after treatment. ERPF = effective renal plasma flow.
Pressure change refers to change in mean blood pressure (baseline to 1-hour post lithotripsy) during experiment. Values from the clinical treatment and 500 pretreatment SW groups were previously published. 6
SW = shock wave.
Overall, low-energy pretreatment with 300 SWs significantly reduced the size of the hemorrhagic injury compared with the injury produced by a typical clinical dose of SWs (Fig. 3). However, not all kidneys reacted the same way after pretreatment. Six of nine kidneys had a lesion size of less than or equal to 0.1% FRV. One kidney had a lesion size of 0.71% FRV, while two kidneys had larger lesions of between 2.5% and 3.5% FRV, which are values near the average lesion size for animals without pretreatment. The most common response (67%), however, was for pretreatment with 300 SWs to produce a small renal hemorrhagic lesion (of 0.1%), which is near the lower limit of our ability to detect a hemorrhagic lesion. Moreover, the mean lesion size produced in the 300 pretreatment SW group was similar to the mean lesion size produced in animals given 500 pretreatment SWs previously reported in this animal model. 6
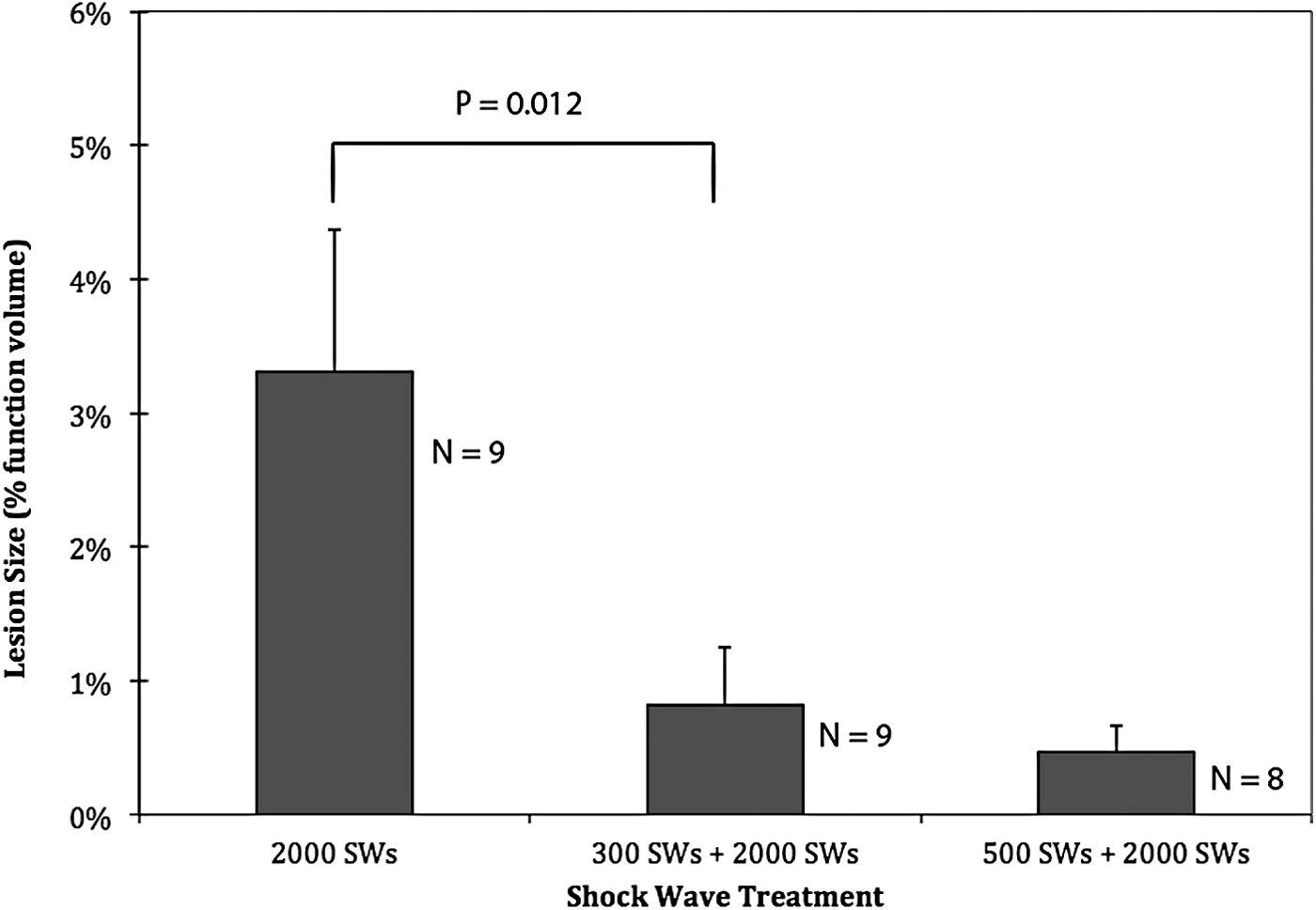
Bar graph of lesion sizes from the different treatment groups. Values from the clinical treatment (2000 SWs) and 500 pretreatment SW groups were previously published. 6 Pretreatment with 300 low-energy SW significantly reduced the size of the measured hemorrhagic lesion compared with group with no pretreatment (far left bar). The 300 low-energy pretreatment animals actually received a total of 2300 SWs, which are 300 more SWs than the animals in the clinical treatment group. No significant difference was found between the 300 low-energy pretreatment group and the 500 low-energy pretreatment group (far right bar). Group sample size (N) is noted next to each of the bars.
Discussion
The present results indicate that 300 pretreatment SWs in a pause-less voltage ramping protocol are sufficient to initiate a protective response in our model when using the Dornier HM-3. Because this protocol incorporates stepwise SW voltage ramping, it raises the possibility that clinical extracorporeal lithotripsy treatments, which use multistep voltage ramping, may also trigger protection in patients. In this regard, a study by Lambert and colleagues, who measured microalbumin and B2 microglobulin biomarkers, showed that patients treated with multistep voltage ramping had less renal injury than patients treated with a fixed SW voltage when given the same number of SWs. 10 Clark and associates have also reported a reduction in tissue injury markers, in pigs, when using a voltage ramping protocol that mimicked a clinical treatment. 11 . This occurred despite the fact that the ramping procedure he employed used a greater number of SWs (2100 SWs) compared with the nonramping procedure (2000 SWs).
There is also a recent prospective randomized clinical study that suggests that voltage ramping can directly impact hemorrhage in the kidney. Skuginna and coworkers have reported a significant change in the rate of renal hematomas in patients after SWL when using a stepwise voltage ramping protocol. They saw a reduction in hematomas when using voltage ramping compared with a nonramping procedure. 12
Is there a threshold number of pretreatment SWs, which can assure that renal protection will be initiated and will minimize the hemorrhagic lesion in our animal model? For the majority of animals in the present study that threshold appears to be as low as 300 pretreatment SWs. However, not all animals responded to the same extent from this pretreatment. To illustrate what we mean by this statement, in the original study where we were just beginning to explore the idea of SW pretreatment protection, delivering 500 low-energy SWs to a kidney followed by a pause and then 2000 high-energy SWs produced an average lesion size of 0.28% ± 0.33% FRV. 5 This value can be considered typical of kidneys protected from SWL injury. If we arbitrarily designate, for the sake of this illustration that only lesion values within two standard deviations from this mean as protected, then 0% of kidneys treated with only a clinical dose of 2000 high-energy SWs would be considered protected. 5 When 100 low-energy pretreatment SWs were delivered before administering 2000 high-energy SWs as part of our pause-less voltage ramping protocol, 25% of the treated kidneys would be considered protected. 6 Increasing the number of low-energy pretreatment SWs to 300 (in this study) or to 500 (reported earlier) resulted in an increase in the percentage of kidneys considered protected from 78% to 87%. These data indicate that as the number of pretreatment SWs increases from 0 toward 500, the number of protected kidneys progressively increase. The data from the present study also suggest that there is a point somewhere between 100 and 300 pretreatment SWs where the number of protected kidneys goes from being a minority of the kidneys to a majority of kidneys. The reason why some treated kidneys undergo renal protection from hemorrhagic injury at a given pretreatment SW level while other kidneys do not is unknown, but could be related to how the protection phenomenon is initiated.
The mechanism(s) responsible for initiating renal protection when using SW voltage ramping is unknown. However, we have shown previously that pretreatment with 500 low-energy SWs with a 3-minute pause followed by a clinical dose of SWs caused a vasoconstrictive response in the treated kidneys (assessed by renal resistive index [RI] measurements). 13 This enhanced vasoconstrictive response occurred earlier in the treatment group using ramping than in kidneys given only a clinical dose of SWs without pretreatment. We hypothesized that this pretreatment protection results from vessel constriction making blood vessels stiffer and less susceptible to rupture by SWs. 6 What is yet to be determined is the factor(s) that trigger this vasoconstriction and how we can manipulate this protective mechanism to consistently reduce renal injury during SWL.
In addition to the question listed above about the nature of the protective mechanism, there remain other questions related to our voltage ramping protocol. First, it is not known if the same mechanism of protection observed in the study cited above also occurs in patients. To help answer this question, Lee and colleagues recently reported that they observed vasoconstriction in patients undergoing SWL with voltage ramping, by following renal RI changes with doppler ultrasound. 14 They observed a significant rise in RI occurring 14.5 minutes after the start of SW treatment. We have reported that significant changes in RI occur around 15.5 minutes after the start of SW treatment when using voltage ramping in our pig model. 13 These time periods are close, which raises the possibility that the mechanism producing the change in RI is similar between patients and our pig model.
A second question associated with SW ramping is whether lithotripters other than the Dornier HM-3 also elicit a protective response when a kidney is exposed to a SW ramping protocol. Again, the results of Lee and coworkers suggest that this phenomenon may be widespread since they used a Dornier Compact Delta II and a Healthtronics LithoTron and they reported similar RI changes as observed with our HM-3. 14 It should be noted that the Compact Delta II is an electromagnetic machine that generates a SW by a completely different mechanism from the HM-3 (electrohydraulic). And the results of Skuginna and associates, even though they did not measure RI, support the notion that renal protection occurs in other lithotripters since their observation of fewer renal hematomas in their voltage ramping group fits our hypothesis that voltage ramping reduces hemorrhage in the kidney. 12 In their study, they used a Storz Modulith SLX for treating their patients. This correlation in observations of RI changes and also expected amounts of hemorrhage between widely different SWL machines increase the likelihood that a similar protective response with SW ramping may occur with other lithotripters.
In conclusion, contemporary SWL treatment is a compromise of factors related to how to optimize stone fragmentation, patient safety, and physician effort. The current study indicates that using 300 low-energy pretreatment SWs in a voltage ramping protocol can significantly reduce injury in the majority of treated kidneys. Drawing on information from patient studies, it appears that the response of human kidneys to SW ramping is similar to that found in our pig model. As such, the current study can be used as a guide to help reduce patient injury while limiting the length of time devoted to treatment. This can be done by selecting 300 or more pretreatment SWs as part of a pause-less stone treatment protocol, thereby avoiding the use of an extended time pause between initial pretreatment SWs and the main body of treatment shocks.
Footnotes
Acknowledgment
This project was supported by a grant from the National Institutes of Health (P01-DK43881).
Author Disclosure Statement
No competing financial interests exist.