
Abstract
Background:
The management of locally recurrent renal-cell carcinoma (RCC) following cryoablation remains a clinical dilemma. There is limited data regarding the management of locally recurrent disease in the setting of patients who have failed initial percutaneous cryoablation (PCA). We evaluate and report our experience with salvage PCA for local recurrence following renal cryoablation failure.
Patients and Methods:
We reviewed our experience with patients who underwent salvage PCA for local biopsy proven RCC recurrence following primary cryoablation procedures. Complications and oncologic outcomes were evaluated. Recurrence-free survival after primary and repeat cryoablation was plotted using the Kaplan-Meier curves.
Results:
A total 250 patients underwent primary cryoablation for RCC and 20 (8%) patients were identified who underwent repeat PCA for 21 locally recurrent tumors. The mean tumor size was 2.4 cm. Biopsy revealed clear cell in 14 patients, three papillary and four chromophobe RCC. All repeat cryoablation procedures were completed successfully, with no treatment failures on postprocedure imaging. There were no complications or deaths. With the median follow-up of 30 months (range 7–63), 3 (15%) patients experienced local recurrence. One patient had an enhancing lesion at 13 months following repeat PCA and underwent a third PCA. Two patients had recurrence at 6 and 35 months respectively and underwent successful laparoscopic partial nephrectomy. Local recurrence-free, metastasis-free and cancer-specific survival rates were 85%, 100%, and 100% respectively. Limitations include retrospective design and small number of patients.
Conclusions:
Repeat PCA after primary cryoablation failure is feasible, has a low complication rate, and acceptable short-term oncologic outcomes. Further studies with durable follow-up are required.
Introduction
A
Several recent studies have reported short, intermediate and long-term oncological outcomes in patients with SRM treated with focal ablation compared to extirpative therapy. 9,10 Ablative modalities have the advantage of significantly fewer postoperative complications compared to radical or partial nephrectomy, and recent studies have demonstrated equivalent long-term cancer-specific outcomes in patients with SRM. 7,11,12 Despite excellent cancer-specific survival, there is a well-documented incidence of local tumor persistence/recurrence with ablative procedures that exceeds that of extirpative options.
As such, the treatment of locally recurrent RCC following cryoablation remains a clinical dilemma. To date, there is limited data available regarding the management of locally recurrent disease in the setting of patients who have failed initial cryoablation. Our objective of this study was to evaluate and report our experience with salvage percutaneous cryoablation (PCA) in the management of locally recurrent RCC.
Patients and Methods
After obtaining Institutional Review Board approval at each participating center, we performed a retrospective review of patients who underwent PCA between January 2005 and July 2012 at two academic institutions. We reviewed and analyzed patient demographics and clinical characteristics as well as intraoperative and postoperative complications. Patients with locally recurrent disease after previous laparoscopic or PCA were included in this study. All patients were confirmed to have recurrent disease on contrast-enhanced CT imaging. CT-guided biopsy of the recurrent lesion was performed on all patients at the time of the secondary cryoablation to confirm the histopathology. All patients who underwent repeat ablation were included in our standard follow-up protocol. The decision to perform a repeat ablation was based on a decision made after an extensive discussion between the surgeon and patients on different treatment options available. Complications were graded according to Clavien grading system. 13
Percutaneous cryoablation
Our technique of PCA has been previously described. 14,15 All procedures were performed collaboratively and included the participation of an interventional radiologist and a urologist. All salvage ablation procedures were done percutaneously under CT guidance with local anesthesia and intravenous sedation. 15
Follow-up
All patients underwent initial contrast-enhanced CT imaging immediately at the termination of the salvage procedure to assess technical success and potential perioperative and immediate postoperative complications. We obtained follow-up contrast-enhanced CT or MRI 3 to 6 months after ablation and annually thereafter. If there was any sign of residual or recurrent disease, additional imaging was performed. We defined treatment failure or residual disease as persistent tissue enhancement within the ablated tumor area on CT imaging within 24 hours after ablation or first imaging after the procedure. We defined local tumor recurrence as new tissue enhancement within the ablated tumor area or a progression of the tumor size after 6 months following the procedure with negative initial imaging.
Statistical analysis
Descriptive data are presented as medians and ranges or counts and percentages. Recurrence-free survival after primary and repeat cryoablation was estimated and plotted using the Kaplan-Meier curves. Survival estimates are presented with 95% confidence intervals (CIs). Statistical analysis was performed using Stata version 12.0 (College Station, TX).
Results
Patient demographics and clinical characteristics
A total 250 patients underwent primary cryoablation for renal cortical neoplasms. Patient demographics and clinical characteristics of the initial cohort are presented in Table 1. Of these, 211 (84.4%) patients underwent PCA and 39 (15.6%) underwent laparoscopic cryoablation (LCA). With a mean follow-up of 32 months, 20 patients (8%) were identified to have 21 recurrent tumors and subsequently underwent repeat PCA. Of the 20 patients with local recurrence, 16 patients had failed prior PCA and 4 had failed prior LCA. Histopathology at the time of repeat cryoablation revealed 14 clear cell RCC, 3 papillary RCC, and 4 chromophobe RCC. There were nine patients with ASA grade II and 11 with ASA grade III. Seven (33%) tumors were located in the upper pole, seven (33%) inter-polar, and seven (33%) in the lower pole. Seven (33%) tumors were located anteriorly and 14 (67%) posteriorly.
Bolded p values are significant.
RCC = renal-cell carcinoma.
Procedure results and complications
All repeat cryoablation procedures were successfully completed without evidence of treatment failure as confirmed by contrast-enhanced CT imaging immediately at the termination of the salvage procedure. There were no minor or major complications. All patients were discharged home the same day of the procedure.
Oncologic outcomes
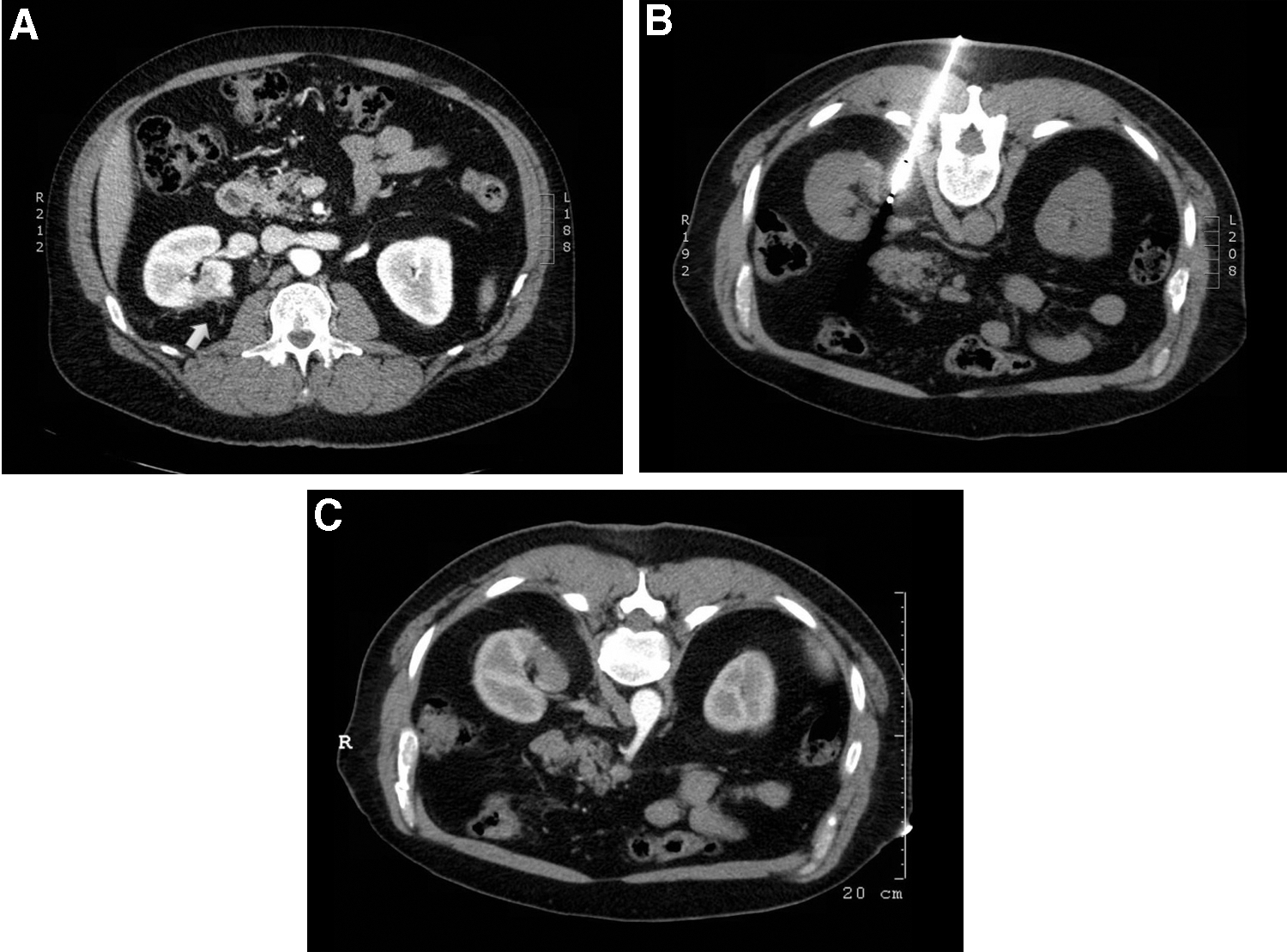
Imaging follow-up was available on all patients who underwent repeat PCA. The 20 patients with failures had a median follow-up of 30 months after second ablation (range 7–63 months). In this group three (15%) patients were identified to have a second local recurrence after repeat PCA. All three secondary failures were noted to have chromophobe RCC at the time of biopsy. These histopathology results were concordant with initial biopsy results at the time of primary cryoablation. One patient was identified to have an enhancing lesion at 13 months following repeat PCA which was ultimately managed successfully with a third PCA. This patient had no evidence of recurrence on contrast-enhanced CT at 26 months after the third PCA (Figure 1). An additional two patients developed tumor recurrence at 6 and 35 months following repeat PCA. Both of these patients successfully underwent uncomplicated laparoscopic partial nephrectomy. With a follow-up of 18 and 24 months respectively, both patients remain without evidence of disease.
Survival outcomes
Kaplan-Meier survival analysis depicts local recurrence-free survival for 250 patients after primary cryoablation and 21 biopsy proven RCC tumors after repeat PCA (Fig. 2). No patients with biopsy proven recurrent RCC died during the course of follow-up. Estimated overall and cancer specific survivals at 3 and 5 years after repeat PCA were 100% and 100%, respectively. Estimated local recurrence-free survivals at 1, 3 and 5 years after repeat PCA in the 21 biopsy proven RCC tumors were 95% (95% CI = 69, 99), 82% (95% CI = 52, 94) and 82% (95% CI = 52, 94), respectively.

Kaplan-Meier estimates of recurrence-Free Survival after primary and repeat cryoablation.
Discussion
The European Association of Urology and American Urological Association Guidelines on the management of SRMs now include cryoablation as an alternative first line treatment option for suboptimal surgical candidates with significant medical comorbidities. 7,16 With our increased institutional experience and promising oncological outcomes, indications for cryoablation have been expanded to younger and healthier patients wishing to avoid extirpative surgery. Thermal ablation has a lower perioperative complication rate than extirpative surgery; however, ablation has been associated with a higher risk of local recurrence when compared to extirpative options.
The 5 and 10 year cancer-specific survival rates associated with thermal ablation have been shown to be equivalent to radical and partial nephrectomy, demonstrating 100% for patients undergoing renal cryoablation. 11 Despite no significant differences between extirpation and thermal ablation in long-term overall survival and disease-specific survival, ablation therapy has been associated with a diminished long-term local recurrence free survival rates of 90% to 100% in patients with up to 10 year follow-up. 7,11,12,17 The recurrence-free survival rate is significantly lower than that associated with extirpative surgery, which manifests a local recurrence free survival greater than 97% in most series. However, most recent large cohort multicenter studies on long-term outcomes of cryoablation has demonstrated recurrence free survival of 95% to 98%. 11,12
The working group of Image-Guided Tumor Ablation defines local tumor recurrence as any persistent or recurrent disease in the treated kidney or associated renal fossa after initial treatment. 18 Currently there are no guidelines for the management of locally recurrent RCC after thermal ablation. Furthermore, there are no formal guidelines for the management of local recurrence after any nephron-sparing approaches for RCC. This has led to controversy regarding the most appropriate salvage treatment therapy. The management of recurrent disease after PCA poses a great challenge to urologists and interventional radiologists. Several management options exist, including active surveillance, repeat ablation, partial and radical nephrectomy. In our cohort of 250 patients who underwent primary cryoablation for RCC, 20 (8%) patients were identified to have a biopsy proven recurrent disease. While all 20 patients were offered active surveillance as an option, they all elected to pursue active treatment strategies.
Open and laparoscopic surgical management of locally recurrent RCC following extirpative as well as ablative procedures can be difficult due to the extensive local fibrosis and eradication of anatomical surgical planes. Salvage surgical treatement is particularly a great challenge for LPN. 19 –22 Nguyen and colleagues were first to report their experience on surgical salvage of local tumor recurrence following primary renal thermal RFA. 21 In their series, six post-RFA LPN were attempted for RCC recurrence, but was successfully completed in only one patient. The remaining five patients underwent conversion to radical nephrectomy due to extensive local scarring. Furthermore, they reported a relatively high perioperative complication rate in these postablation patients undergoing extirpative surgery. Similarly, several other studies have reported that LPN following thermal ablative treatment is technically challenging, and associated with increased complication rates, higher estimated blood loss, longer operative times and higher recurrence rates. 19,20,22,23 Of note, in the current series, two patients underwent salvage partial nephrectomy after two PCA procedures. Both procedures were minimally technically challenging and were successfully accomplished without complication.
According to a literature review performed between 2000 and 2006 by Long and colleagues, repeat cryoablation is the most commonly used treatment modality following failed prior cryoablation. 24 Approximately 66% to 73% of patients who fail thermal ablation are managed by repeat focal therapy. 25 The literature is sparse with limited data regarding patient characteristics, perioperative complications and oncologic outcomes in those undergoing repeat PCA. Overall, salvage PCA has demonstrated an improved safety and convalescence profile compared to salvage LPN. Due to the truly minimally invasive nature of PCA, repeat ablation has gained increased popularity among urologists. 26 Compared to the challenges during LPN, PCA does not provide any additional technical challenges compared to primary ablation. 27 Indeed, repeat PCA procedures are typically considered less technically challenging than initial procedures. The technical simplicity of salvage PCA is likely due to the presence of landmarks, which result from the postablation tissue reaction, facilitating tumor targeting. Additionally, salvage cases typically have a smaller residual tumor volume. Additional advantages of using PCA in this patient population include an expeditious convalescence, significantly shorter procedure times, diminished pain, and the ability to perform the procedure under moderate sedation thus providing a viable treatment option for patients with significant comorbidities and avoiding the risks associated with general anesthesia. With regards to the complications of salvage PCA, Hegg and colleagues reported a major complication rate of 5.7% in patients who underwent repeat PCA after local recurrence following LPN. 27 In our series, all patients were discharged within 24 hours of the procedure. There were no complications, and no patient required a blood transfusion. All procedures were performed in less than 2 hours under local anesthesia with sedation.
In terms of the oncologic efficacy of repeat PCA, we demonstrated a 100% cancer-specific survival rate. With a mean follow-up of 30 months the recurrence-free survival was 85%. Three patients failed secondary treatment and experienced a second local recurrence following salvage cryoablation. All three patients were found to have biopsy confirmed chromophobe type RCC. One patient underwent a third cryoablation and two patients opted for and underwent laparoscopic partial nephrectomy. All three patients had no evidence of local or distant metastasis at follow-up.
Although chromophobe RCC is generally known to be an indolent malignant RCC sub-type with a better overall prognosis compared to conventional RCC, 28,29 all three patients who experienced a secondary recurrence were confirmed to have chromophobe histopathology. This finding may be biologically important with regards to cryoablation for RCC, but the limited number of patients in this series makes definitive conclusions challenging.
Matin and colleagues reported their multi-institutional experience of 46 patients after salvage energy ablative therapy, of these, 37 had no further evidence of disease following the repeat treatment. Although the study did report the largest series of salvage ablative therapy, the authors did not specify how many patients received RFA or cryoablation, which does not aid in the determination of the efficacy of RFA vs cryoablation for salvage treatment. Thus, with the mean follow-up of 2 years, the overall incidence of recurrent disease after salvage energy ablative therapy was 4.2% and metastatic-free survival rate was 97.4%. 30 Long and colleagues review of current literature found that 2.5% of 336 patients who had undergone initial PCA for RCC subsequently underwent repeat PCA for tumor recurrence. Despite the limited number of patients reported in the literature, repeat PCA is increasingly gaining popularity with very encouraging oncologic results. Our recurrence-free survival in the salvage setting was 85%, and all three patients were managed with repeat third ablation or partial nephrectomy with no evidence of disease recurrence on subsequent imaging follow-up. Overall and cancer specific survival rates demonstrated to be 100%. However, there remains the need for prospective multi-institutional studies to identify the ideal candidates for salvage cryotherapy.
Limitations of the current study include the short-term nature of our follow-up. Longer follow-up studies with larger sample sizes are required to elucidate whether repeat ablation is efficient and reliable treatment option in this patient population. Additionally, we did not evaluate renal functional outcomes, as the majority of renal functional follow-up data was unavailable. The primary objective of the paper was feasibility, safety and oncologic outcomes.
Conclusions
Salvage percutaneous renal cryoablation for locally recurrent disease after primary ablation failure is technically feasible, has a low complication rate, and demonstrates acceptable short-term oncologic outcomes. Further studies with larger numbers of patients and durable follow-up are required to elucidate the role of PCA in this patient population.
Footnotes
Acknowledgment
We acknowledge that the abstract included in this manuscript has been previously published in multiple conference proceedings.
Author Disclosure Statement
No competing financial interests exist.