
Abstract
Objective:
To investigate the effectivity of 4.5F ultrathin ureteroscope (UT-URS) without any need for active or passive dilation in the treatment of adult patient population in whom ureteral orifices cannot be engaged using conventional URS.
Materials and Methods:
Among a total of 512 adult patients who had undergone URS between April 2012 and November 2015 in our department for diagnostic or therapeutic purposes, 43 (8.4%) patients required ureteral dilation because we could not engage ureteral orifice. In adult patients in whom we could not engage ureteral orifice with 7.5F and 8F semirigid URS, we tried to complete the operation using 4.5F UT-URS without resorting to dilation. Age and gender of the patients, indication for operation, stone size, location, operative times, laterality of stone(s), stone-free rates, length of hospital stay, and complications were recorded.
Results:
Mean age of the patients was 34.5 ± 11.2 (21–66) years. The patients had undergone operations for ureteral stone (n = 39), unexplained hydronephrosis (n = 2), and ureteral stenosis (n = 2). Mean stone size was 8.2 ± 2.3 (4–18) mm. Mean operative time was 64.2 ± 13.5 minutes. In 37 of 39 patients, a complete stone-free rate (94.8%) was achieved. Mean length of hospital stay was 8.9 ± 5.8 hours.
Conclusion:
It has been demonstrated that in an adult patient population in whom ureteral orifices cannot be engaged using conventional URS, ureteral access could be achieved with 4.5F UT-URS without any need for dilation. At the same time, use of 4.5F UT-URS resulted in an acceptable treatment success and lower complication rates in most of these patients without the need for a second session.
Introduction
N
We want to dismiss these debates and bring a new perspective to difficult cases with stenotic ureteral lesions. In our department, as a standard procedure, we are using 7.5F to 8.5F ureteroscopes for adults and the 4.5F ultrathin ureteroscope (UT-URS) for pediatric cases.
New publications are available about the use of 4.5F UT-URS in the pediatric age group. In our article, where we shared experiences of our department with this instrument in patients younger than 3 years of age and indicated lower complication rates, rapid ureteral engagement and nearly 94% stone-free rates were achieved. 10 In another study, 4.5F UT-URS and 7.5F URS were compared in the pediatric age group by our team. 11 In this study, the advantages of UT-URS, including no need for ureteral dilation, minimal requirement for fluoroscopic guidance, lower intraoperative and postoperative complications, and higher stone-free rates, have been demonstrated. After years of experience in children, in recent years we have started to use 4.5F UT-URS in challenging cases in an adult patient population. In challenging adult cases that do not develop serious complications as perforation and avulsion, we think that the use of 4.5F UT-URS is a good alternative to active or passive dilation, in addition, it provides opportunity for the completion of the treatment.
In this study, we aimed to present our 4.5F UT-URS treatments and their outcomes without resorting to active or passive dilation within the last 4 years in adult patients who were scheduled for URS for diagnostic purposes or stone treatment, where we could not engage into the ureter with conventional instruments or patients who had undergone failed URS attempts in other centers and then had been referred to us.
Materials and Methods
Among a total of 512 adult patients who had undergone URS between April 2012 and November 2015 in our department for diagnostic or therapeutic purposes, 43 (8.4%) patients required ureteral dilation because we could not engage ureteral orifice. Thirty-four of these patients were cases with primary URS, and 9 patients were referred to our department from other centers because of failed URS procedures. In adult patients in whom we could not engage ureteral orifice with the 7.5F and 8F (Storz Ureteroscopy; KarlStorz, Tuttlingen, Germany) semirigid URS, we tried to complete the operation using the 4.5F (ultrathin ureterorenoscope 4.5F; Richard Wolf GmBH, Knittlingen, Germany) URS without resorting to dilation. In patients who were referred from an external center because of failed URS, we started to perform 4.5F UT-URS. In such failed cases, if ureteral calibration was adequately dilated, we switched to conventional URS and these patients were excluded from the study.
Age and gender of the patients, indication for operation, stone size, and location were recorded. Location of the stone was determined based on direct urinary kidney, ureter, and bladder radiograph (KUB), urinary ultrasound (US), IVP, and/or noncontrasted CT. The patients for whom 4.5F UT-URS was used were divided into subgroups according to etiologies. Before the procedure, negative urine cultures were achieved in all patients, and the patients received antibiotic prophylaxis. All operations were performed by the same surgeon. All operations were performed under general anesthesia with the patients in the lithotomy position. Before proceeding with URS, all patients underwent cystoscopy, and a 0.038-inch hydrophilic guidewire (Sensor™ Guide Wire; Boston Scientific, Natick, MA) was advanced through a 7.5F or 8F ureteroscope to engage ureteral orifice. In cases with stenotic ureteral orifice or any ureteral segment, a second guidewire was passed through an endoscope to achieve the procedure. If this step failed, then we switched to 4.5F UT-URS so as to perform the procedure.
None of our patients received active or passive dilation, and for ureteral engagement, a 0.038-inch hydrophilic guidewire was advanced under fluoroscopic guidance. Isotonic saline was used for irrigation. We did not have an automatic irrigation pump; instead, a Y-type transurethral resection bladder irrigation set (Y-TUR set) with its own pump was used to gain better visualization by squeezing the pump manually. For fragmentation of the stone, holmium:YAG (Ho-YAG) laser with a 150 μ Ho-YAG laser fiber was used. The fragmentation procedure was continued till stone particles were broken into fragments smaller than 1 mm in size. In cases of need, the stone fragments were taken out with a 3F basket catheter (G0197; Boston Scientific) or stone forceps. Operative times, laterality of stone(s), stone-free rates, length of hospital stay, and complications were recorded. Complications were categorized based on the Clavien classification. 12 Postoperatively, according to the patient height, 4.7F 26 or 28 cm Double-J stents were implanted in all patients. On postoperative day 1, KUB was obtained to determine stone-free status. The patients were called for a control visit at the end the first postoperative month and their Double-J catheters were removed. Three months after removal of the Double-J catheter, the patients were investigated radiologically (US and/or IVP) for the presence (if any) of ureteral stenosis and hydronephrosis.
Results
The mean age of the patients (male n = 34 and female n = 9) was 34.5 ± 11.2 (21–66) years. The patients had undergone operations for ureteral stone (n = 39), unexplained hydronephrosis (n = 2), and ureteral stenosis (n = 2). The patients had proximal (n = 10), midureter (n = 11), or distal (n = 18) ureteral stones. The mean stone size was 8.2 ± 2.3 (4–18) mm (Table 1).
In 34 patients whose stenotic ureters did not permit access to ureteral stone with 7.5F to 8F URS, ureterovesical stenosis (n = 27), complete ureteral stenosis (n = 2), narrowing of a short ureteral segment (n = 2) or postoperative stenosis of the distal one-third of the ureter following pelvic surgery (n = 1), and complete ureteral stenosis due to a presence of a bifid system (n = 2) were detected. In nine patients referred from an external center, access to the stone could not be achieved and Double-J stenting could not be performed in seven patients, while the procedure failed because of partial ureteral rupture in two patients (Table 2). Percutaneous nephrostomy had been applied in four patients, including two patients who developed perforation. The remaining five patients did not undergo percutaneous nephrostomy or Double-J stent implantation.
URS = ureteroscopy; UT-URS = ultrathin ureteroscope; UV = ureterovesical.
Mean operative time was 64.2 ± 13.5 minutes. Right UT-URS in 24 and left UT-URS in 19 patients were performed. In 37 of 39 patients, a complete stone-free rate (94.8%) was achieved. Mean length of hospital stay was 8.9 ± 5.8 hours (Table 3).
Ho-YAG = holmium:YAG.
ESWL was performed after Double-J placement in one of two patients, in whom the stone migrated into the kidney. The other migrated stone was treated by flex-URS after 1 month of stented period. Mild hematuria was seen in two patients who were treated conservatively. One patient had high fever during postoperative period and treated with appropriate antibiotherapy. In seven cases, ureteral laceration occurred due to the use of conventional URS (Table 4).
All of these lacerations occurred during usage of conventional semirigid ureterorenoscopes.
UTI = urinary tract infection.
Discussion
In line with developing technology, endourologic instruments were miniaturized, which enabled surgeons to perform surgery with more comfort and safety. The first URS had been performed by Young nearly 100 years ago and the 12F pediatric cystoscope had been used. Nowadays, instruments nearly one-third of those previously used have been introduced into clinical practice.
Although ureteroscopy has been used with more than 90% success rates, in the literature, complication rates ranging between 9% and 25% have been also reported. 13 –15 These complications can be classified as intraoperative, early postoperative, and long-term complications. Intraoperative complications may be seen, including stone migration (4.26%), diffuse bleeding (0.1%), mucosal injury (1.5%), ureteral perforation (0.6%), and ureteral avulsion (0.1%). 14 During the early post-URS period, fever and urosepsis (1%), renal colic (2.2%), persistent hematuria (2%), and in the long term, ureteral stenosis (0.1%) and persistent vesicoureteral reflux (0.1%) can be seen. 14
In our cases, the stone migrated into the renal collecting system in two cases (5%, Clavien 3). Moderate hematuria developed in two (2.5%; Clavien 1) patients who were conservatively treated. In two patients followed up with conservative treatment, moderate hematuria developed (5%, Clavien 1). In one patient, high fever was observed during postoperative period (2.5%, Clavien 1). In seven patients, mucosal injury occurred (16%, Clavien 1). All of these lacerations occurred during usage of conventional semirigid ureterorenoscopes. Although the complication rate related to the usage of 4.5F UT-URS was 11.6% (n = 5), we think that some of these complications such as stone migration occurred due to usage of conventional semirigid ureterorenoscopes before application of 4.5F UT-URS.
A limited number of data are available about the use of 4.5F UT-URS in adults. Atis and colleagues who evaluated the effectiveness of 4.5F UT-URS on 104 patients compared 4.5F UT-URS and 8.5F URS and indicated that patients in the 4.5F UT-URS group required ureteral balloon implantation less frequently and had lower complication rates with similar stone-free rates and operative times. 16 While Kocaoglu and colleagues evaluated the effectiveness of 4.5F UT-URS in prepubertal 36 patients, and reported 97.4% stone-free rates without any need for ureteral dilation, 17 Atar and colleagues compared 7.5F and 4.5F UT-URS in prepubertal 69 children and reported stone-free rates of 92% and 78% in the 4.5F UT-URS and 7.5F UT-URS groups, respectively. They indicated statistically significant advantages favoring 4.5F UT-URS, including higher stone-free rates, lower complication rates, and decreased requirement for fluoroscopy. 11
Yaycioglu and colleagues compared the outcomes of 7.5F and 10F URS on 1000 cases and found higher success rates in the 7.5F group with lower complication rates, but without any statistically significant intergroup difference. 18
The present study has been performed in a special patient group. We achieved 94.8% success rate in the same session in 43 patients included in the study following failed URS procedures, which would lead to Double-J stent implantation or percutaneous nephrostomy to be performed in a second session if 4.5F UT-URS was not realized. We think that since 4.5F UT-URS is thinner than the mostly applied 4.7F Double-J stent catheters, it is effective in the achievement of success rates comparable to overall URS rates in patients who experienced failed 7.5F URS procedures.
In patients whose ureteral orifices cannot be engaged with conventional instruments or in patients who present difficulties for URS, ureteral balloon dilation or stepwise mechanical dilation apart from Double-J stent implantation have been frequently used methods. In a global ureterorenoscopy study performed on 9681 cases, Perez Castro and colleagues indicated the requirement for balloon or dilation in proximal (40%), midureter (23%), distal ureter (21%), and multiple stones (29%) in indicated percentages of cases. 15 We prefer to decrease calibration of our ureterorenoscope rather than increasing it in our adult patient group (Fig. 1) Thus, we think that we can save money, spare time spent for dilation, and also avoid complications related to dilation. In addition, a potential advantage of such a small ureteroscope could be the small rate of postoperative strictures.
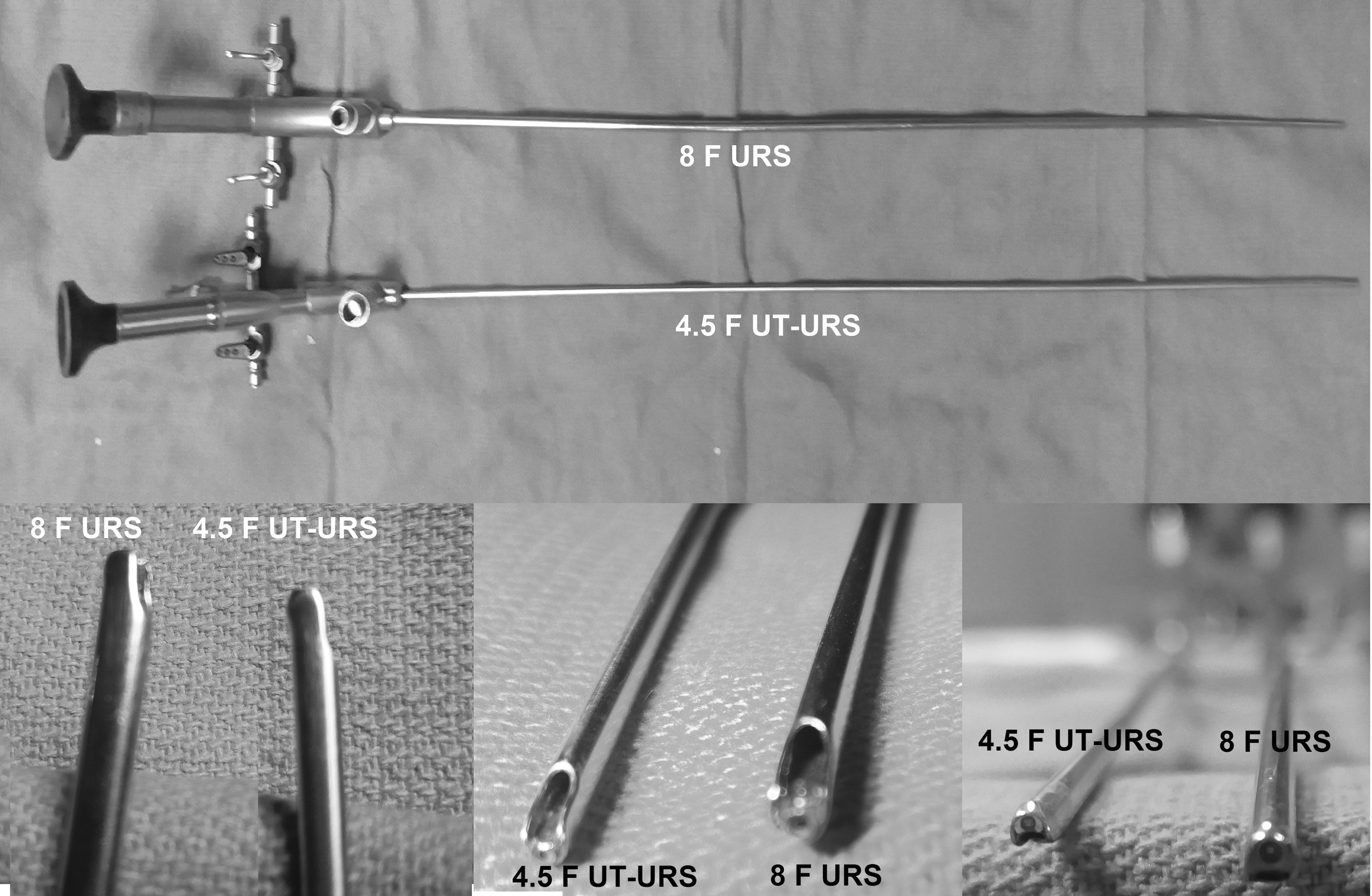
Appearance of different size ureteroscopes.
The most important limitation of our study is its retrospective design. The scarce number of patients is our other limitation. Besides, application of 4.5F UT-URS presents some difficulties. Its small caliber provides major advantages especially in stenotic ureters; however, inadequate irrigation through its narrow working channel (3.3F) and its low image quality are disadvantages of this instrument. Due to insertion of forceps or lithotripters through the working channel, irrigation fluid hardly enters the ureter with a further decrease in image quality. To solve this problem, we increased the irrigation pressure by the pump of Y-TUR bladder irrigation set as mentioned in the Methods section. Because of these disadvantages, we have not routinely used 4.5F UT-URS for adult patients. Another question is what is the cost of these instruments and is this procedure cost-effective than an active or passive dilatation? The cost of a 4.5F UT-URS is ∼20,000 dollars in Turkey. However, endourologists, who are frequently faced with pediatric urolithiasis patients, should have a miniaturized ureteroscope for pediatric ureteral stones. Therefore, we recommend to get a 4.5F UT-URS not only for adult patients but also for pediatric patients.
As an outcome of this study, it has been demonstrated that in the adult patient population in whom ureteral orifices cannot be engaged using conventional URS, ureteral access could be achieved with 4.5F UT-URS without any need for dilation. At the same time, the use of 4.5F UT-URS resulted in an acceptable treatment success and lower complication rates in most of these patients without the need for a second session. Still, large-scale prospective studies should be performed on this issue.
Footnotes
Author Disclosure Statement
No competing financial interests exist.