
Abstract
In recent years, laparoscopy and robot-assisted procedures have become more commonplace in urology. Incorporation of these techniques into clinical practice requires extensive knowledge of the surgical approaches and complex instrumentation unique to minimally invasive surgery. In this review, focus will be directed to laparoscopic trocars including differing subtypes, placement in select urologic procedures, and proper use with emphasis on the avoidance of complications. Differing methods for the development of pneumoperitoneum and the associated risks of each will be discussed. The aim of this article is to provide a complete review of laparoscopic trocar use for the practicing urologist.
Introduction
N
Instrumentation
Skin preparation
Skin antisepsis before manipulation is aimed at the reduction of pathogenic skin flora responsible for surgical site infections (SSI). A number of solutions have been used in this regard; the most common contemporary forms are chlorhexidine or povidone-iodine based. Randomized comparison in clean contaminated surgery saw a significant reduction in the rate of superficial and deep incisional infections in the chlorhexidine group. 1 Unfortunately, only a small proportion of enrolled patients underwent urologic procedures (6.4% chlorhexidine vs 8.0% povidone-iodine). A 2015 Cochrane review found low quality evidence supporting the use of alcohol-based chlorhexidine vs povidone iodine in the limited of SSI. 2 While data supporting skin preparation before laparoscopic or robotic procedures are sparse, a chlorhexidine-based preparation is typically used for all such procedures at our institution, unless a contraindication to use exists.
Establishment of pneumoperitoneum
Multiple entry methods exist for the initial establishment of pneumoperitoneum for laparoscopy and robotic procedures, each with their own purported benefits to increase efficiency and limit the rate of associated complications. Indeed, greater than 50% of major complications related to these procedures arise during insufflation attempts and initial trocar placement. 3 –5 A recent Cochrane review with 46 randomized control trials (RCTs) evaluating 13 methods of laparoscopic entry techniques found insufficient evidence to determine the most optimal approach. 6 However, it is prudent to be aware of alternative techniques when faced with challenging situations.
Blind (veress needle) access
The most common method of peritoneal insufflation introduction is with blind Veress needle entry. Although frequently used, it is not without risk, and may account for more than 50% initial entry complications, with major injuries occurring in 0.9/100,000 cases. 7,8 However, it has been shown to be safe in patients with a history of prior abdominal surgery, if placed away from the area of prior instrumentation. 9
The Veress needle is unique due to its two-cylinder design consisting of an outer short and an inner long component. The inner cylinder has a retractable blunt tip, which retracts, deploying the outer sharp edge, when contacting resilient structures, allowing passage through the abdominal wall. When the blunt tip has re-engaged after passage through the abdominal fascia a “click” may be audible. This, in conjunction to tactile feedback, allows the physician to determine when to stop needle advancement.
Generally an umbilical entry site is chosen, as there is no muscular layer to traverse. The abdominal wall may be elevated, either with use of towel clamps or manually. Doing so will increase the distance between the parietal peritoneum and the abdominal viscera. If prior umbilical surgical scars or hernias are encountered, or if the patient is obese (>30 body mass index [BMI]), the Veress may be introduced at Palmer's point, which is located 3 cm below the left costal margin in the midclavicular line.
Needle placement must be confirmed and a number of methods may be employed for this purpose including needle aspiration, injection and recovery, the so-called “drop test,” and the initial intraperitoneal pressure test. Analyses comparing these methods of confirmation found the initial intraperitoneal pressure test to be the most reliable, though all may assist with the avoidance of iatrogenic injury. 10
Successful placement of a Veress needle suggests that the site of puncture is free of any adhesions or bowel and hence safe for initial trocar placement. In cases where planned intial trocar placement is away from the Veress needle point of entry, a second Veress may be used to to confirm whether or not planned trocar site is safe. A method employed at our institution involves the placement of a second Veress needle, with the stopcock open, in the proposed location of the initial trocar and after insufflation through the primary Veress has been initiated. Audible gas from the second Veress confirms intraperitoneal placement of the initial Veress needle and the absence of substantial adhesions in this location. 11 The abdomen is then insufflated to a pressure determined by the surgeon. Our preferential insufflation pressure is 15 mmHg.
Direct trocar access
Though the most frequently utilized method of entry, the Veress technique still requires three blind steps. Infrequently used, though only requiring one blind step, the direct trocar insertion technique requires elevation of the anterior abdominal wall with one hand or with preplaced towel clamps, while blindly advancing the trocar with a twisting motion into the peritoneum. Visual inspection with the camera confirms proper placement before the onset of insufflation. This technique is concerning however, as the lack of pneumoperitoneum allows for little margin of error and can easily result in bowel or vascular injury. This method may also be combined with an optical access trocar, though this is usually done into an insufflated abdomen (see below).
Open (Hasson) access
Many surgeons, despite the increased time it takes to perform, prefer as an alternative to the Veress, the Hasson technique. Briefly, this involves an open skin incision, which is then deepened down to the underlying fascia. The fascia is incised, just enough to permit port placement. Stay sutures are often placed on either side of the fascia to assist with securing the trocar and closure at the conclusion of the procedure. The peritoneum is then elevated and incised and a blunt tip trocar is placed. A number of Hasson trocars are equipped with a balloon that is inflated within the peritoneum, preventing dislodgement or loss of insufflation.
Open hand assist
Surgeon preference and case-specific variables may dictate the need for hand-assisted techniques. A number of devices are available for this purpose, including the GelPort (Applied Medical Resources Corporation, Rancho Santa Margarita, CA) and Endopath Dextrus (Ethicon, Somerville, NJ). The benefit of these ports is the ability to rapidly insert one's hand, laparoscopic ports, or remove specimen while maintaining pneumoperitoneum.
These ports also may be inserted at the start of the operative procedure and facilitate initial port placement and subsequent insufflation. Generally, an incision is made at a predetermined location corresponding to the size of the surgeon's hand, the fasica is incised, and the peritoneum is entered. The inner ring of the port is inserted and a hand is used to inspect for intraperitoneal contents trapped between the ring and the abdominal wall. The outer ring is pulled up and rolled down to form a tight seal on the abdominal wall. The outer gel seal cap may be placed at this time. Once the surgeon's hand has been inserted, the area underlying preselected port sites may be palpated. Trocars may be introduced in the standard fashion until contact has been made with the underlying hand within the peritoneum, thus ensuring appropriate depth and avoidance of visceral injury. Insufflation may then be initiated.
Entry technique comparative outcomes
Much of what guides clinical application of surgeon-specific laparoscopic entry technique choice is anecdotal evidence and experience. Unfortunately, the mostly poor quality literature precludes the designation of a recommended technique. Recent Cochrane review analyzed 46 RCTs and 13 entry techniques. Generally, open techniques have a higher rate of successful entry vs closed techniques. Direct vision entry techniques (optical trocar) do not decrease the likelihood of visceral organ injury vs the Veress needle approach. Somewhat surprisingly, direct trocar access is associated with lower risk of vascular injury and failed entry vs the Veress needle approach. Additionally, open (Hasson) techniques are not associated with a reduction in organ injury of failed entry vs direct trocar entry. 6
Trocar selection and placement
A wide variety of trocar sizes, both in length and diameter, and designs exist. Use generally depends on the operative procedure being performed, surgeon preference, institutional availability, and specific experience. The majority of trocars contain similar components, namely a hollow working cannula, an inner obturator that is removed after port placement, an internal seal or valve preventing the loss of pneumopertioneum, and an external stopcock, through which insufflation may be managed. Not all trocars have stopcocks, an example being robotic 8 mm trocars for the S/Si robot. The goal of any trocar is to provide a simple means to readily access the operative field, while maintaining insufflation. Ideally, a trocar, regardless of type, would facilitate efficient access, while limiting associated complications, such as hernia, bleeding, and damage to surrounding structures.
Traditional laparoscopy and robot-assisted surgery requires proper spacing of trocars to triangulate instruments toward the target tissue. Generally spacing is optimized at 6 to 8 cm between individual trocars, improving ergonomics and lessening arm or instrument “clashing.” This distance is often approximated using the horizontal width of the surgeon's hand.
Reusable vs disposable
The decision to use reusable vs disposable trocars often is a monetary one. The cost of cleaning for repurposing must be weighed against that of new disposable equipment. Our practice commonly utilizes reusable, threaded, trocar-less, rotational access EndoTIP cannulas (Karl-Storz, Tuttlingen, Germany) in several sizes during a variety of procedures. For example, common port arrangement for laparoscopic nephrectomy involves use of a 10 mm EndoTIP cannula for endoscopic camera placement and 5 mm EndoTIP cannula for sub-xiphoid instrument port, in addition to the valveless Airseal® trocar (see below). These trocars have the added benefit of reduced axial forces, often negating the need for fascial closure. 12
Blunt tip vs bladed trocar
Many surgeons prefer the blunt, dilating trocars to their bladed, cutting counterparts. The advantage of these being the smaller fascial defect created, limiting both the need for closure in some cases and the development of port site hernias. 12 Blunt trocars may also be associated with less access-related bleeding, as vessels and muscle are pushed away, rather than cut. 13
In contrast, bladed trocars offer more rapid intraperitoneal access, but often at the cost of safety, particularly in those with a history of prior abdominal surgery. The majority of these come with a safety tip covering the sharp place and which allow deployment of the blade once resistance is encountered in a manner similar to the Veress needle design.
As mentioned above, Ternamian EndoTIP cannulas (Karl-Storz) are frequently utilized in our practice. As these cannulas are threaded and lack sharp points, coordinated rotation is utilized for abdominal entry. This helps to maintain fascial integrity, as tissues is displaced, rather than cut. The threaded outer lining also maintains trocar positioning and resists slipping.
Optical access trocar
Optical access trocars afford the surgeon the ability to insert the 0° endoscope directly inside the clear tip trocar, enabling visualization of all the abdominal layers during port placement. Examples include the bladeless Versaport (Covidien-Medtronic, Minneapolis, MN) and Endopath Optiview (Ethicon) and the bladed Visiport (Covidien-Medtronic). Optical trocars may be placed before or following the development of pneumoperitoneum. Though the concept of layer visualization would seem superior to blind placement of initial trocar or Veress needle, significant injuries are still possible. Retrospective analysis of the 12 mm Endopath Bladeless visual obturator trocar (Ethicon Endosurgery, Cincinnati, OH) insertion in the periumbilical region or lateral to the rectus muscle before insufflation revealed a 2.1% of large bowel injuries. 14
Valve-less trocar
Marketed as the Airseal (SurgiQuest, Inc., Milford, CT), the valve-less trocar system represents an alternative to conventional laparoscopic trocars and unidirectional insufflation systems. The system is comprised of three components: the Airseal intelligent Flow System Control Unit, Tri-Lumen Tube set, and the bladeless Access trocar. Within the trocar, recirculated CO2 creates a horizontal pressure barrier formed by a network of small nozzles and greater than that of the intra-abdominal pressure. Unlike conventional trocars, the Airseal trocar features no mechanical seals or valves and allows unobstructed access to the working cavity. Trocars are available in 5, 8, and 12 mm forms. The Tri-Lumen tubing contains single tubing for each for inflow and outflow of CO2 gas and a third lumen responsible for continuous pressure sensing. This allows maintenance of stable pneumoperitoneum during continuous aspiration. 15,16
Several studies have evaluated its use in contrast to that of conventional systems, with some finding reduced operative times, improved pressure maintenance, and lower CO2 consumption in favor of the Airseal system. 16,17 A prospective trial focusing on patients undergoing robot-assisted radical prostatectomy found improved insufflation pressure stability and reduced number of trocar manipulations among the Airseal arm. However, overall surgical time and CO2 consumption did not differ between the groups. 15
In our practice, the Airseal system is utilized with all laparoscopic and robotic procedures. The superb maintenance of pneumoperitoneum, especially in delicate situations (i.e., dissection of the renal hilum), makes this an ideal system that may overcome loss of peritoneum associated with overzealous suctioning. Further, the Airseal system allows smoke evacuation via the recirculation of intraperitoneal CO2 and the trapping of smoke, potentially resulting in improved visualization during cauterization without the need for a smoke evacuator. The valve-less trocar design also enables easier extraction of delicate tissue (i.e., lymph nodes) and needles.
Radially expanding trocar
Theoretically limiting the likelihood of incisional hernia, the radially expanding VersaStep (Covidien) is a unique form of dilating trocar. It stretches the fascial incision radially, yielding a smaller fascial defect. Initially a Veress type needle is placed and the abdomen is insufflated. Once a sufficient pressure is achieved, the needle is reinserted inside the radially expandable sleeve. After the sleeve is in position, the needle is removed and the cannula is inserted through the sleeve and locked in position. One benefit of this trocar is the low rate of insufflation leak during procedure, as the fascial defect is stretched to accommodate the trocar, rather than cut. In fact, the defect is 50% smaller than that created by cutting trocars. 18 It has been shown the limited defect size created reduces port site hernias, even in the absence of fascial closure. 19 Radially expanding trocars are not associated with a reduction in organ or vascular injury, when compared to traditional trocars. 6
Trocar–less instrument insertion
In some cases not requiring a large amount of instrument manipulation throughout the procedure, it is feasible to directly insert working instruments through a small puncture incision. In our practice, this is most frequently performed during right laparoscopic adrenal or renal surgery, for use in liver retraction. A small incision is made medial and cephalad to the right hand working port and a 3 or 5 mm locking grasper is inserted through the fascia under direct visualization. Doing so limits the need for an additional trocar site and maintains pneumoperitoneum while gaining needed visualization.
Laparo-endoscopic single site surgery
The goal of single site laparoscopy is the limitation of the number and size of the incisions vs that of conventional multiport laparoscopy, improving aesthetic outcomes, and the theoretical reduction in morbidity. Included in this category are needlescopic surgery (<3 mm instruments), single port or single incision laparoscopy (single port laparoscopic surgery, laparo-endoscopic single site surgery [LESS]) and natural orifice surgery. 20,21 We will only discuss LESS in this article. Optimal outcomes necessitate proper patient selection, especially when still within the learning curve of these complex techniques.
Conventional laparoscopy typically entails multiple trocars triangulated toward target tissue. In LESS the camera and operating instruments are inserted through a single port and are generally in parallel toward target tissue. The angle between left and right instruments is generally 10° or less. 22 Another consideration is the close approximation of the trocars may lead to “clashing” both inside and outside of the abdomen. Because of this, standard laparoscopic instruments are unwieldy, and articulating instruments are necessary.
Two methods exist for the arrangement of trocars in LESS; the multi-trocar and access port techniques. With the former, two or more trocars are inserted through a single fascial defect. Although standard laparoscopic trocars may be used, varying trocar housing length or the use of low-profile trocars, such as the Versaport Bladeless Optical Trocar (Covidien-Medtronic), may be helpful in avoiding external “clashing” if utilizing this technique. 22 Despite this, trocar maneuverability can become an issue and maintenance of pneumoperitoneum is often hampered by persistent gas leak. 22
A number of commercially available access ports, both reusable and disposable, exist for use in LESS, the benefit of each being the less complex insertion of subsequent trocars with maintenance of pneumoperitoneum. Some feature dedicated trocars embedded in the membrane (ex. GelPoint®; Applied Medical Resources Corporation), while others allow the surgeon the freedom to place conventional trocars E•Z Access (Hakko, Nagano, Japan). Much like the GelPort (Applied Medical Resources Corporation), these membrane devices may be placed to facilitate initial access and pneumoperitoneum, and facilitate specimen retrieval. Others, such as the Single Site Laparoscopy Access System (Ethicon Endosurgery, Inc.) feature access ports without the need for external trocars.
Closure of port sites
Although herniation may occur with port size as small as 3 mm, most surgeons would agree fascial closure is necessary in ports 10 mm or larger. 23 As standard suture closure can be difficult, especially in the obese, a number of devices have been developed to simplify this process. All operate under similar principles, essentially passing a suture through the fascia and pulling it through the contralateral side. Consistently found to be faster and less fraught with complications is the Carter-Thomason device. 24,25
Depending on the number and size of ports being utilized during a laparoscopic procedure, one or more may require fascial closure. At our institution, with adult patients, ports larger than 10 mm in size undergo fascial closure. Though a number of methods exist for this purpose, it is our experience that the most straightforward way this may be accomplished is using the Carter-Thomason device.
Our method involves 0 or 1–0 Vicryl suture, grasped in the middle of the strand. This is then passed laterally, adjacent to the trocar occupying the port being closed. Once the suture is visually noted within the peritoneum, the Carter-Thomason is removed, leaving the suture in situ. The device is then again passed on the contralateral aspect of the fascial incision and the suture is retrieved. It is advisable to have a laparoscopic grasper prepared to assist with this process, should difficulty be encountered coordinating the grasping of the suture. Certain cases may necessitate a figure of eight configuration for adequate closure, including 15 mm trocar ports, morbidly obese patients, or in cases where single suture closure is tenuous.
Comparison studies have demonstrated reduced operative time and a significant reduction in bowel and wound-related complications with use of the Carter-Thomason suture passer vs traditional hand suturing techniques. 26 Multiple commercially available products utilize the same principles as the Carter-Thomason suture passer but often with a plastic device that guides passage (ex. Endo Close™; Covidien-Medtronic), Carter-Thomason CloseSure System® (Cooper Surgical, Trumbull, CT).
Trocar site anesthesia
Though often associated with reduced pain vs open procedures, trocar site discomfort following minimally invasive urologic surgery may impact recovery and delay discharge. The value of local trocar site infiltration with anesthetic agents is contentious. Recent Cochrane review specifically assessing use in laparoscopic cholecystectomy found limited support for its use. 27 A randomized trial of patients undergoing transperitoneal laparoscopy (renal and adrenal surgery) found wound infiltration before skin closure with levobupivacaine was associated with increased narcotic requirement vs those patients receiving perioperative paracetamol or lomoxicam. 28 However, given the low associated risk, we routinely infiltrate trocar sites with bupivacaine 0.5% with epinephrine. We have found this, in addition to postoperative acetaminophen and narcotics, provides suitable analgesia for the majority of our laparoscopic and robotic procedures.
Site Selection
Anatomic landmarks
Description of port placement for all urologic procedures is beyond the scope of this article and may vary depending on surgeon preference. However, a number of anatomic landmarks must be appreciated to guide the precise placement of trocars.
The umbilicus and periumbilical area is clearly visible and centrally located in most patients, providing an ideal initial port placement site for a number of procedures. In nonobese patients, the distance between the skin and peritoneum is thinnest at the level of the umbilicus, facilitating easier access at this location.
The anterior superior iliac spine (ASIS) is another, easy to discern, site identified with port placement. In our practice, a 12 mm working port is placed medial and cephalad to the ASIS for laparoscopic transperitoneal renal surgery.
Transperitoneal Procedural Considerations
Prior abdominal surgery
Prior intra-abdominal surgery raises concern for adhesions and distorted anatomy that may complicate laparoscopy, leading to longer operative time, and increase likelihood for inadvertent injury. A recent prospective analysis of over 1100 patients undergoing minimally invasive radical prostatectomy (robotic and laparoscopic) revealed no increase in the rate of overall or abdominal perioperative complications. 29 However, one must take surgical history into consideration and perform a thorough physical examination before planning any procedure.
Morbid obesity
A surgeon is presented with a number of challenges when attempting laparoscopy in the morbidly obese patient. The morbidly obese patient is more likely to have medical comorbidities limiting their tolerance of surgery and increasing the likelihood of complications in the perioperative period. Increased body mass index (BMI) and visceral adiposity has been linked with longer operative times especially among nonexpert surgeons. 30,31 Despite this, laparoscopy is the approach of choice for a number of procedures, including appendectomy and cholecystectomy, as it is shown to be associated with a reduced length of stay. 32,33 Retrospective reviews of patients stratified according to BMI have shown equivalency in intraoperative variables (operative time, ischemia time), oncologic outcomes, and postoperative complication rates in both laparoscopic and robotic single-site nephron sparing surgery, suggesting feasibility of minimally invasive techniques in the obese patient. 34,35 In contrast, obesity has been linked to increased operative times in both laparoscopic and robotic radical prostatectomy. 36,37
The thick anterior abdominal wall and peritoneal layer complicates insufflation and the placement of trocars. Depending on the degree of adiposity, when placed in the lateral decubitus position, the pannus and umbilicus may fall away from the side of interest. In these instances, trocar placement should be shifted laterally and the umbilicus should not be used for access.
The Veress needle is safe to induce pneumoperitoneum, but the surgeon must be cognizant of the degree of adiposity and vary the angle of needle introduction accordingly, realizing that in the obese patient the angle may be 90°. 38 Hasson entry is an option, however, visualization may be hampered by depth of dissection, increasing operative time and limiting efficiency. Additionally, poor visualization may result in large fasical incisions, resulting in gas leakage throughout the procedure, though this may be ameliorated to some extent with the use of a balloon trocar. 39 With initial insufflation it may be helpful to temporarily increase pressure to 20 mmHg, which serves the dual purpose of elevating the large abdominal wall away from the peritoneal contents and increasing tension on the abdomen, facilitating subsequent trocar placement. 40,41 The surgeon must first review preexisting contraindications before increasing insufflation pressure.
Trocar insertion can be likewise fraught with difficulty. Incorrect insertion angle may result in skiving through abdominal fat. To eliminate this possibility, we bluntly dissect directly down with a Kelly clamp to the fascial layer after skin incision. The skin incision need not be extended larger than that needed to accommodate the trocar. The fascia may be palpated with a finger to confirm adequate dissection. The trocar is then placed directly through the fascia, limiting the need to traverse the outer fatty portions of the anterior abdominal wall.
Robotic procedures
Robotic assistance offers a number of benefits to simplify laparoscopic procedures including EndoWrist® (Intuitive Surgical, Sunnyvale, CA) instrumentation, 3-D visualization, and reduction in surgeon tremor and fatigue. This approach has become a mainstay in a number of urologic procedures, including radical prostatectomy, partial nephrectomy, and pyeloplasty, among others.
Robotic trocars are distinct from their laparoscopic counterparts. Depending on the da Vinci system used, the endoscope may be placed within a 12 mm port (S, SI Systems) or an 8 mm robotic trocar (Xi System). Robotic trocars are 8 mm in size with bladeless or blunt obturators and allow use of all EndoWrist instruments. A 12 mm robotic trocar is necessary if the EndoWrist robotic stapler is to be used. Specially designed 5 mm cannulas, and 8 to 5 mm reducers, may also be employed for use with 5 mm EndoWrist instruments, depending on surgeon preference. Alternative third party trocars are manufactured, including the Passport (Stryker Endoscopy, San Jose, CA), which features interchangeable bladed and blunt-tip entry options in a single trocar. If robotic positioning must be modified during the procedure or a portion of the case is to be performed laparoscopically (ex. nephroureterectomy), a robotic 8 mm port may be placed within a 12 mm port. A robotic instrument may be used through this port until reconfiguration of the robot or conversion to laparoscopy, at which point the trocar may be used for camera or large working instrument insertion.
Recommended site selection
Laparoscopic partial/Radical nephrectomy
The patient is placed in the modified lateral decubitus position (Fig. 1). A 10 to 12 mm camera port is placed initially, at the level of the umbilicus. Additional working ports are placed subxiphoid (5 mm) and cephalad to the ASIS on the appropriate side (12 mm). When working on the right side, liver retraction may be achieved either through an additional port placed superiomedially to thesubxiphoid trocar (if using a locking grasper) or cephalad to the 12 mm port (if using liver retractor). In the obese, ports should be shifted laterally to the rectus muscle, thus limiting the distance between skin incision and target tissue.
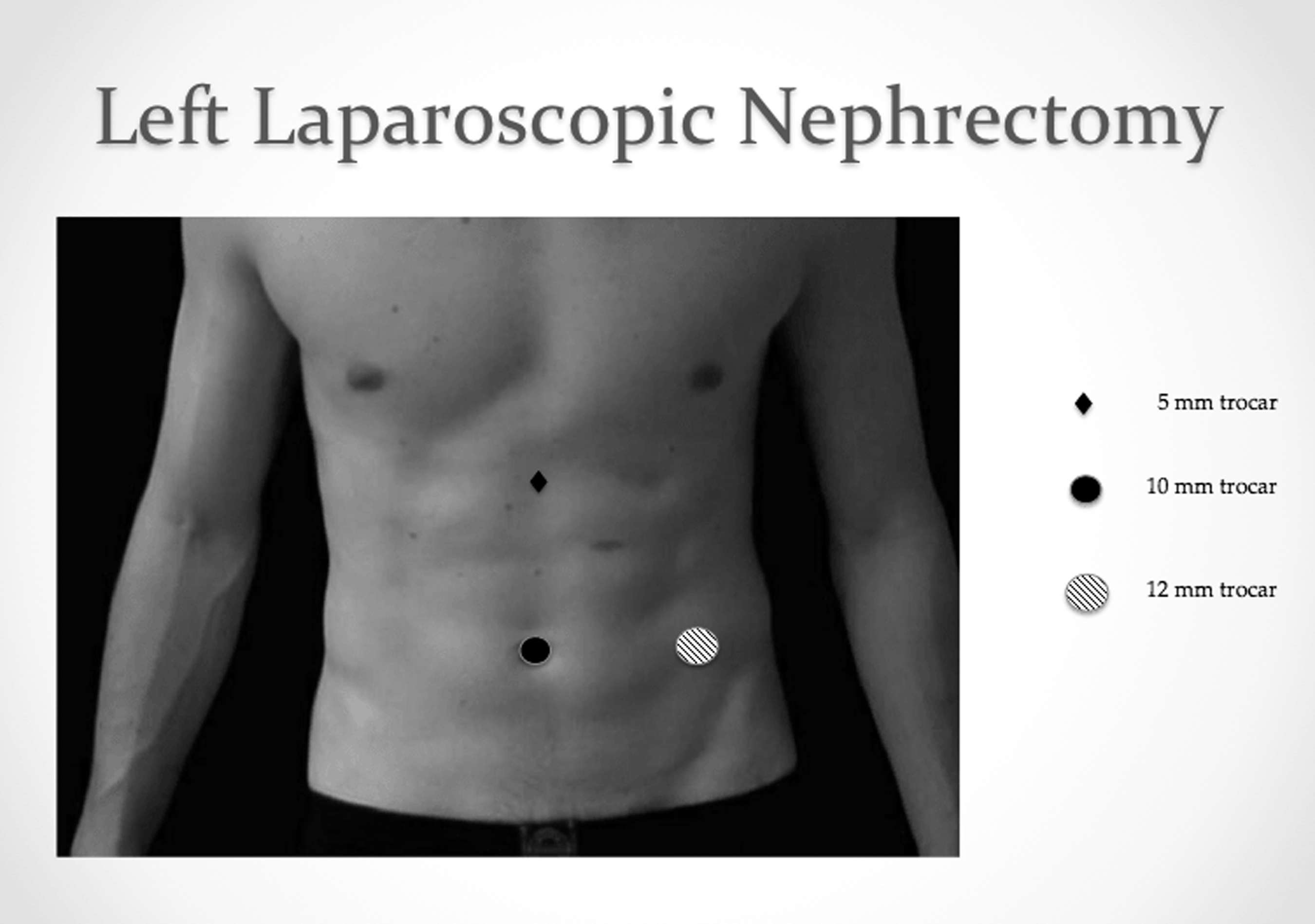
Left laparoscopic nephrectomy port placement.
Laparoscopic adrenalectomy
The patient is positioned in the modified lateral decubitus position. After adequate insufflation pressure is reached, a 10 to 12 mm trocar is placed in the midclavicular line below the costal margin on the appropriate side. Two additional 5 mm working ports are placed under vision to triangulate the target gland. The first may be placed just inferior to the costal margin, slightly off midline. A second 5 mm port is placed laterally, in the anterior axillary line. When operating on the right side, an additional sub-xiphoid 3 to 5 mm trocar may be placed, for use in liver retraction.
Laparoscopic/Robotic nephroureterectomy
Both robotic and laparoscopic procedures necessitate the patient be positioned in the modified lateral decubitus position. Proper patient positioning and port placement at the initiation of the procedure may obviate the need for repositioning during the distal ureteral dissection.
Port placement for laparoscopic procedures mirrors that of laparoscopic radical nephrectomy with an additional 12 mm port, placed in the midline between the umbilicus and pubis. This may be used by the assistant for additional retraction during the nephrectomy portion of the procedure, and by the surgeon during dissection of the distal ureter and bladder cuff. Again, lateralization of the ports may be necessary in the obese patient to limit working distance between port and target tissue.
Robotic nephroureterectomy (Fig. 2) may be performed without the need for robotic movement or patient repositioning with the following port configuration. The initial 12 mm (or 8 mm, if using the Da Vinci Xi system) camera trocar is placed just lateral to the rectus above the level of the umbilicus. Two additional robotic 8 mm trocars are placed in the mid-clavicular line, triangulating the target kidney. The final 8 mm port, representing the robotic fourth arm, is placed laterally, below the margin of the 12th rib. A 12 mm assistant port may be placed between the umbilicus and pubis. A 3 to 5 mm sub-xiphoid trocar may be inserted to facilitate liver retraction. After the completion of the nephrectomy portion of the procedure, the superior 8 mm robotic trocar is exchanged for a 12 mm port and will serve as the assistant port for the distal dissection. An 8 mm robotic trocar is inserted into the original 12 mm assistant port and will serve as access for the inferior robotic instrument.
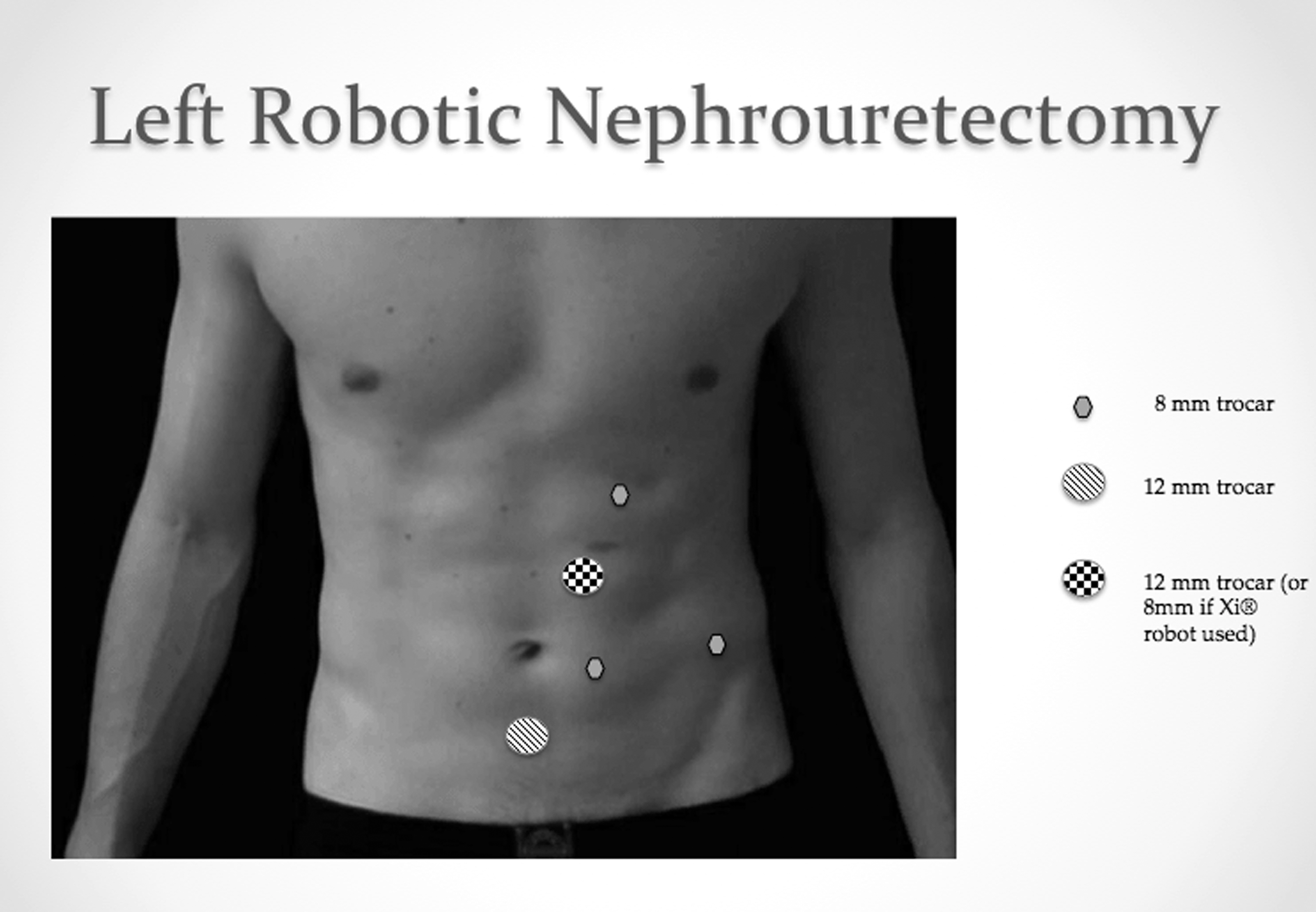
Left laparoscopic nephroureterectomy port placement.
Robotic Radical/Suprapubic prostatectomy
The patient is placed in the dorsal lithotomy position with steep Trendelenberg (Fig. 3). After induction of pneumoperitoneum, initial 12 mm (or 8 mm, if using the Da Vinci Xi system) camera trocar placement is performed at the umbilicus. At the same level, 8 mm robotic trocars are inserted lateral to the rectus. An additional 8 mm robotic trocar is placed laterally on the right, in the anterior axillary line. A 12 mm working port is placed in on the left, laterally, in the anterior axillary line. A second assistant working port is placed superior to and between the camera and left robotic arm ports.
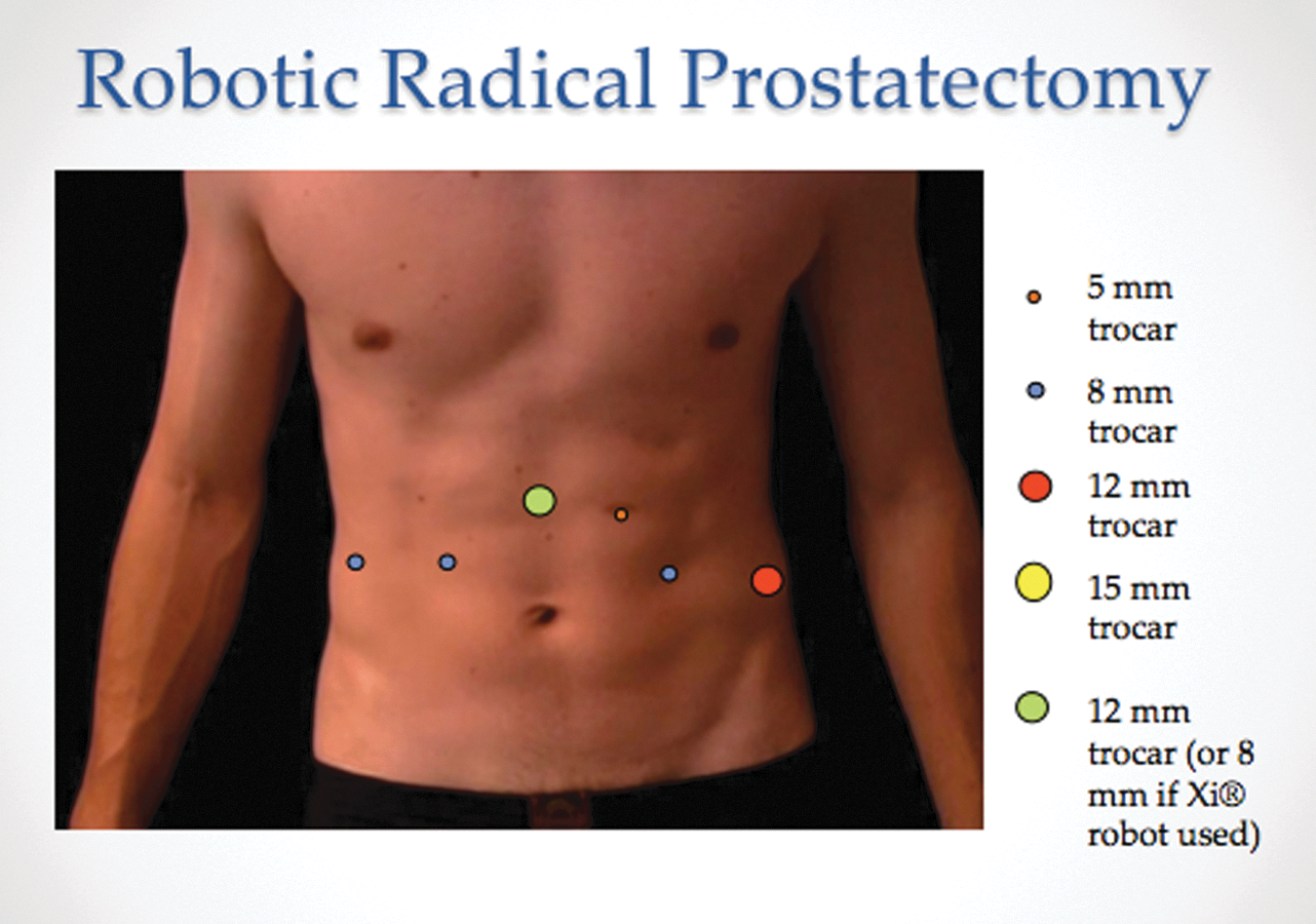
Robot-assisted radical prostatectomy port placement.
Robotic radical cystectomy
Patient positioning and port placement is similar to that of robotic radical prostatectomy, with slight modifications (Fig. 4). The patient is placed in the dorsal lithotomy position with steep Trendelenberg. After induction of pneumoperitoneum, initial 12 mm (or 8 mm, if using the Da Vinci Xi system) camera trocar placement is performed, typically at the level of the umbilicus. Limitations in the patient's body habitus or a planned extended nodal dissection may necessitate movement of the camera port cephalad. At the same level, 8 mm robotic trocars are inserted lateral to the rectus. An additional 8 mm robotic trocar is placed laterally on the right, in the anterior axillary line. A 12 mm working port is placed in on the left, laterally, in the anterior axillary line. A second assistant working port is placed superior to and between the camera and left robotic arm ports. An additional suprapubic 15 mm trocar is placed for robotic radical cystectomy, for insertion of the retrieval bag and specimen extraction.
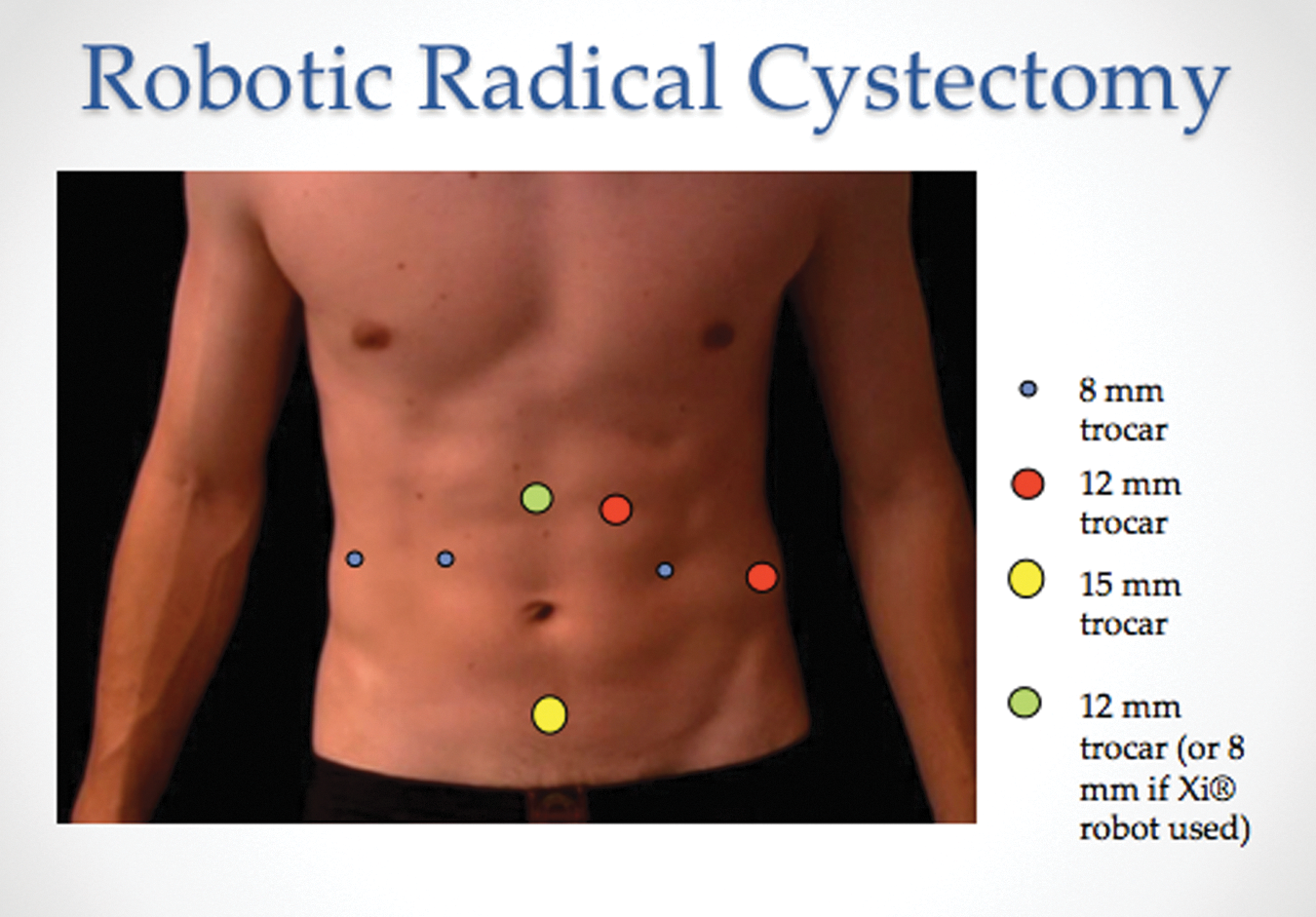
Robot-assisted radical cystectomy and urinary diversion port placement.
Laparoscopic/robotic inguinal lymphadenectomy
By utilizing techniques borrowed from blepharoplasty and retroperitonoscopy, space is created underneath Scarpa's fascia but above the fascia lata in the thigh. This affords direct access to inguinal nodes and allows dissection to be performed, while sparing patients a large inguinal incision and the associated risk of flap necrosis.
Port placement is planned based on the classic box drawn for the thigh flap. The camera port is placed at the inferio-medial aspect of the box with two robotic arms placed on the lateral aspect of the box and an assistant port placed at the most lateral-inferior aspect of the box. All ports are placed one handbreadth apart. The initial port site is incised and a flap is raised allowing for the passage of a retroperitoneal balloon dilator. The balloon dilator is advanced into the space and inflated to create ample space for the placement of the remainder of the ports. A balloon secured Hasson port is placed for the camera (and an extra-long Xi robotic port is telescoped into the 12 mm Hasson port). Insufflation pressure is typically set between 8 and 15 mmHg, to prevent tracking of CO2 beyond the intentionally dissected space.
Retroperitoneal considerations
Retroperitoneal laparoscopy and robotic surgery has become more common and is most commonly utilized for renal and adrenal surgery, and lymphadenectomy. Limitations of this approach include the lack of familiar landmarks and reduced working space, creating a rather steep learning curve. Despite this, studies have suggested reduced operative time, including shorter time to renal artery control, overall lower complication rates, and reduced length of stay in retroperitoneal laparoscopic nephrectomy vs traditional transperitoneal techniques. 42,43
Development of the retroperitoneal potential space requires more than insufflation alone, and balloon dilators are employed at the procedure onset. A number of balloon modalities exist with some, such as the Kidney Distension Balloon (Covidien, Mansfield, MA), allowing endoscope placement and direct visualization of inflation. The primary 12 to 15 mm incision for laparoscopic procedures is typically made below the 12th rib and carried down to the underlying retroperitoneum, ideally allowing palpation of the renal lower pole anteriorly and the psoas muscle posteriorly. Once placement is confirmed, balloon dilation may commence. Subsequent trocar insertion and insufflation occurs following the creating of the potential space. Port placement is commonly modified caudally for robotic procedures, to increase the distance between robotic arms and the target tissue. 44 The camera port is placed one fingerbreadth above the iliac crest in robotic retroperitoneal renal surgery. 45 Precise attention to port spacing is crucial given the limited working space of the retroperitoneum. Generally, a distance of at least 7 cm is required to avoid arm “clashing” in robotic procedures. Measurements should be taken after the establishment of pneumoretroperitoneum.
Overcoming complications
Although untoward injury may occur at any time during laparoscopy, the establishment of pneumoperitoneum and the initial placement of trocars represent the largest proportion of complications. The literature supports that as high as 50% of complications of laparoscopic surgery are associated with this stage of the procedure.
Bowel and solid organ injury
Bowel and other associated organ injury during laparoscopy is rare; bowel injuries occur in 1.3 out of every 1000 procedures. 46 However, the consequences, especially if unrecognized during surgery, may be devastating to the patient. Access injuries more commonly affect the small bowel, occurring in 41.8% of all bowel injuries. 47 Prior abdominopelvic surgery is thought to increase the possibility of bowel injury due to adhesion formation and anatomic distortion. However, recent series like that of Ball et al. demonstrated no access related intestinal injuries in 300 patients with prior history of either inguinal or abdominopelvic surgery who underwent minimally invasive trans or extra-peritoneal prostatectomy (lap and robotic). 48 Likelihood of gastrointestinal injury, especially with upper abdominal access, may be reduced with placement of an orogastric or nasogastric tube before needle or trocar placement. 49
Management of bowel injuries depends on both the mechanism and degree of injury. If Veress aspiration confirms gastrointestinal contents or asymmetric insufflation is detected, concerning bowel or visceral perforation, alternative entry should be pursued and the area examined once insufflation is safely achieved. Further manipulation of the Veress needle should be avoided if blood or succus is aspirated during placement. If alternative access cannot be achieved, conversion to open surgery is indicated. Often in the absence of full-thickness injury to the bowel wall with enteric spillage, these injuries may be managed conservatively, owing to the small diameter (∼2 mm) of the Veress needle. Larger injuries may necessitate oversewing of the injury or bowel resection. Depending on the experience of the surgeon, general surgery consultation may be advisable. Gallbladder and bile duct injury is an uncommon complication, occurring in 2 in 2866 transperitoneal procedures in one series and should be managed with intraoperative general surgical consultation. 50
Because of their larger diameter, it is often trocar entry that causes the majority of clinically relevant injuries. Whenever possible, trocars should be inserted under direct visualization and the vicinity inspected for related visceral injury. Recent Cochrane review comparing visceral injury complication rates among distinct trocar types found no significant difference in incidence between radially expanding and cutting trocars. 51 Unfortunately, existing evidence is of very low quality, owing to the low rate of reported visceral injury.
Vascular injury
Although relatively rare, occurring in 0.05% to 0.26% of cases, major vascular injury understandably may result in significant morbidity or mortality in some cases. 52 Up to 75% to 87.5% occur during the passage of the Veress needle or initial trocar placement. 53 –55 Several authors have argued that the incidence of vascular injury is greater in the closed-access (Veress needle) than open-access (Hasson) approach. 56,57 In a series of over 5000 patients who underwent laparoscopic urologic procedures there were three patients with major vascular injury related to the closed-access technique vs zero vascular complications in nearly 4900 open-access procedures. All major injuries, two to the abdominal aorta and one to the external iliac vein, in the closed-access group were sustained during placement of the initial trocar in laparoscopic nephrectomy. 58 However, Cochrane review failed to show a difference between entry technique and likelihood of vascular injury. 6 Meta-analysis examining the use of radially expanding vs cutting trocars found no difference in the rate of vascular injury in 473 patients studied in four RCTs. It is important to note the rate of major vascular injury was exceedingly low in these studies, with only one injury reported. Trocar site bleeding, not associated with major vascular injury, was less common with the use of radially expanding trocars vs cutting trocars (3.5% vs 11.5%) in five studies comprised of over 500 patients included in the review. 51
Genitourinary injury
Direct access related injury to the urinary bladder is uncommon in urologic laparoscopy. Minimization of potential risk by decompression through urethral foley placement at the procedure start is advisable. If confined to the dome, cystotomy repair may be pursued in the standard fashion. If concomitant extravesical ureteral or trigonal injury is suspected or observed, formal evaluation of the upper urinary tract should be performed with retrograde pyelography. Partial injury to the ureter may be managed with indwelling ureteral stent placement. Complete disruption may require ureteroneocystotomy or ureteroureterostomy, depending on the level of injury. Surgeon experience dictates the need for open exploration in these circumstances.
Trocar site hernia
Trocar site hernias (TSH) may have a variable presentation depending on the degree of herniation and the contents herniated. TSH may also be characterized as early, in which abdominal contents protrude through a peritoneal defect, or late, in which the peritoneum herniates with abdominal contents, depending on the remoteness to the surgical procedure. 59,60 Occasionally, patients may present postoperatively with acute bowel obstruction, frequently Richter hernia type, requiring urgent surgical intervention. However, the vast majority of patients present with tenderness localized to a prior port site and an equivocal exam, underscoring the need for a low threshold for cross-sectional imaging. Patients may also present weeks to months postoperatively with an abdominal bulge and no bowel obstruction. 60
Clinically significant TSH is a relatively rare occurrence, with prevalence between 0% and 5.2% in various studies. 59,60 Recent evidence suggests the rate of radiographic TSH after robotic procedures may be as high as 6.7% and occurring more commonly at larger trocar sites and those used for specimen extraction. 61 Surprisingly, single incision laparoscopy may be associated with an increased incidence of TSH vs conventional laparoscopy, when access is obtained at the umbilicus. 62
An increase in the size of port site can correlate to increase risk of TSH; incidence 0.23% and 1.9% at 10 and 12 mm trocar sites, respectively. In the urologic literature, a retrospective study of 1055 laparoscopic cases revealed a 0.7% rate of TSH. TSH occurs more frequently in hand-assisted laparoscopy vs standard laparoscopy, likely owing to the larger wound size and fascial defect. 63
The umbilicus is the most common location of port site herniation. 64 Larger trocars (≥12 mm), especially those of pyramidal cutting shape had a higher association with TSH in a systematic review. 59 In this article, multiple additional risk factors were suggested, such as long surgical duration and patient related factors such as old age and high BMI. However, most were supported by only one study. 59
Relatively sparse evidence exists regarding the prevention of TSH. The results of the aforementioned systematic review supported the closure of larger port sites (>10 mm), despite insufficient evidence. In our practice all port sites >10 mm are closed with slowly absorbable suture. Use of port size of 5 mm and less may help prevent TSH. Whatever the size, trocar sites should be inspected for herniated structures after the full evacuation of abdominal CO2 and before proceeding with wound closure. Whenever possible, all ports should be removed under direct visualization with pneumoperitoneum maintained. The camera is removed within the final trocar, so as to prevent the suctioning of bowel contents through the fascial defect during extraction.
Wound infection
Generally, laparoscopic procedures have a reduced incidence of infectious complications vs open procedures, occurring in 1.8% to 6.3% of cases. 65 –67 Hand-assisted laparoscopy has been associated with increased rate of wound infection-related complications, up to 6.8% in one series. 63 Despite this, the current American Urological Association recommended antibiotic prophylaxis regimen encourages a single dose of first generation cephalosporin for those procedures not entering the urinary tract (ex. radical nephrectomy). Conversely, first or second generation cephalosporins (alternatively aminoglycoside with either metronidazole or clindamycin) are recommended for all procedures with potential for urinary spillage (i.e., pyeloplasty, partial cystectomy). Likewise, in all procedures in which bowel is utilized, use of second or third generation cephalosporins (alternatively aminoglycoside with either metronidazole or clindamycin) is recommended. 68
Antibiotic prophylaxis choice should take into consideration patient specific risk factors that would increase propensity for infectious complications, including the development of wound infection. These risk factors encompass the general factors associated with poor healing or propensity to infection, including advanced age, immunodeficiency, smoking, presence of externalized catheter, and others.
Signs and symptoms of port site infection include wound drainage, incisional erythema, pain, and fever. 66 Treatment includes reopening of the prior incision, drainage, and packing. The incision should be probed to ascertain the integrity of the fascia. Infectious complications may be prevented with the use of standard sterile protocol and prophylactic antibiotic adherence. Specimen bag use during extraction, particularly in cases with known infected tissue, may be beneficial. 69
Footnotes
Author Disclosure Statement
No competing financial interests exist.