
Abstract
Purpose:
Shockwave lithotripsy (SWL) is a widely utilized form of treatment for urolithiasis. There are new evidence-based recommendations regarding pre-SWL patient work-up and the performance of SWL. The purpose of this study is to determine practice patterns for SWL and to determine if regional variation exists between Canada and the United States.
Materials and Methods:
A 19-question survey was prepared. Canadian urologists were surveyed through e-mail correspondence. In the United States, members of the Endourologic Society and members of two large stone management groups were surveyed. Canadian and American results were compared using the chi-square and Fisher's exact tests.
Results:
Ninety-four Canadian urologists and 187 U.S. urologists completed the survey. Practice patterns differed between countries. Intravenous sedation was more commonly used in Canada (Canada 94.7% vs United States 17.9%, p < 0.001); routine antibiotics were more commonly given in United States (Canada 2.1% vs United States 78.1%, p < 0.001); a shock rate of 2 Hz was more common in Canada (Canada 76.6% vs United States 16.2%, p < 0.00001); rate of discontinuing ASA for renal and ureteral stone treatment was higher in the United States (renal Canada 88.3% vs United States 95.7%, p < 0.02; ureteral Canada 62.4% vs 90.3%, p < 0.0001); and ureteral stents were more commonly used if treating a large stone or patients with solitary kidneys in the United States (large stones Canada 58.2% vs United States 88.8%, p = 0.0001; solitary kidney Canada 50.6% vs 66.3%, p = 0.02).
Conclusions:
This study highlights the absence of standardization of SWL. Significant regional differences exist in practice patterns and performance of SWL between Canadian and American urologists.
Introduction
S
This study was performed to identify Canadian and American practice patterns with respect to the preprocedural work-up and performance of SWL to determine if lithotripsy centers in Canada and the United States utilize similar treatment strategies. The secondary aim was to investigate the technical performance of SWL and the incorporation of evidence for optimal SWL performance at SWL centers in Canada and the United States. We hypothesize that there is great variability in the technical performance of SWL in both countries and wish to raise the question: are best practice guidelines for SWL supported to optimize treatment outcomes, minimize patient morbidity and, subsequently, minimize costs to our healthcare systems?
Materials and Methods
This study utilized a 19-question survey (Fig. 1). The survey covered three main domains of SWL: the preprocedural work-up of the patient, the technical performance of SWL (e.g.: shock power, number, and rate of delivery), and measures taken to prevent complications (e.g.: holding antiplatelet medications, use of stents, and antibiotic usage). The survey was administered to Canadian urologists at each of the 16 stationary lithotripsy units in Canada. American urologists working with two large mobile lithotripter partnerships (Midwest Stone Management, Fortec Lithotripsy) were surveyed using paper surveys and members of the Endourologic Society were surveyed using SurveyMonkey®.
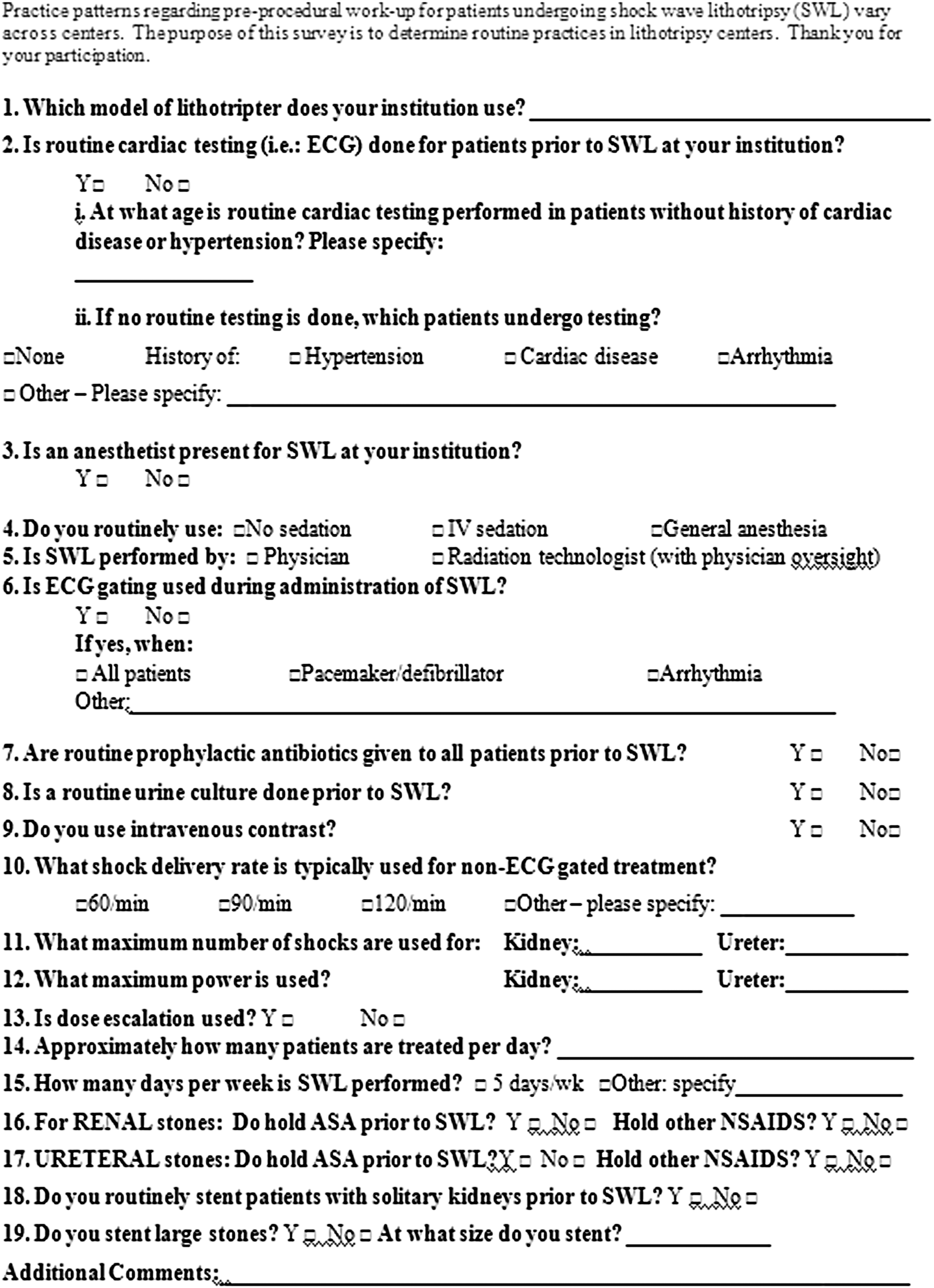
SWL practice pattern survey. SWL = shockwave lithotripsy.
Responses from Canadian and American urologists' were compared using Fisher's exact test or chi-square test as indicated. All statistical analyses were performed using SAS version 9.2 software (SAS Institute, Inc., Cary, NC).
Results
A total of 97 Canadian urologists from 16 centers and 187 American urologists completed the survey. Sixty-seven percent of Canadians surveyed were in academic practice. Approximately 30 percent of American urologists surveyed were in academic practice.
Canadian results
Sixty-two percent (10/16) of Canadian centers perform electrocardiograms (ECGs) before SWL based on an age-based cut-off for those with no cardiac risk factors, with a median age of 50 years or older to have a routine ECG. Other centers would perform ECGs in patients with a history of hypertension (31%), history of coronary artery disease (50%), arrhythmia (56%), or “medically complex” patients (6%) regardless of age.
Fifty-one percent of centers routinely perform a urine culture to screen for asymptomatic bacteriuria before SWL, and only 2% of Canadian urologists surveyed routinely used prophylactic antibiotics before SWL. Ninety-five percent use intravenous sedation/analgesia during SWL (instead of general anesthesia) and 68% routinely have an anesthetist present during treatment.
Gating (delivery of shockwaves during the refractory period of the cardiac cycle) was reported to be used by 78% of urologists in Canada if treatment was causing arrhythmia, but it was not used routinely. The majority, 76%, of Canadian urologists routinely use a shock rate of 2 Hz (120 shockwaves/min), while 26% use a rate of 1.5 Hz, and 16% routinely use 1 Hz. There was some variability in shock rate with some urologists decreasing from 2 to 1.5 Hz for stones larger than 1 cm. For renal stones, most (64%) urologists stopped treatment at a max of 3000 shocks; for ureteral stones, 69% halt at 3000 shocks and 29% go as much as 3500 to 4500 shocks.
Eighty-eight percent and 62% of Canadian urologists routinely hold acetylsalicylic acid (ASA) before treatment of renal stones and ureteral stones, respectively. Fifty-one percent will routinely stent patients with solitary kidneys before SWL and 58% will stent patients with large stones (typically with a cut-off of >1.5 cm).
American results
Forty-nine percent of American urologists reported that an ECG was performed before SWL with a median age of 50 years or older receiving an ECG. Regardless of age, the percentage of respondents reporting that an ECG is performed before SWL if the patient had a history of hypertension was 31%, coronary artery disease, 59%, and arrhythmia, 59%.
Seventy-eight percent of American urologists reported using routine prophylactic antibiotics. Intravenous sedation was used by 17.9% of American urologists with the vast majority (82%) performing SWL under general anesthesia; 98% of American urologists reported having an anesthetist present during SWL.
Gating was reported to be used by 12% of American urologists routinely and by 73% if an arrhythmia developed during treatment. Sixteen percent of American urologists routinely use a shock rate of 2 Hz, 45% use a rate of 1 Hz, and 41% reported using a rate between 1 and 1.5 Hz (typically 1.5 Hz or 90 shockwaves per minute), with some respondents reporting lowering the rate depending on the size of the stone. The number of shocks delivered was generally greater for mid/distal ureteral stones with a median of 3000 shocks vs a median of 2800 shocks for stones in the kidney/proximal ureter. Twenty-four percent and 40% would go above 3000 shocks in the kidney/proximal ureter and mid/distal ureter, respectively.
Ninety-six percent of American urologists routinely hold ASA before SWL for renal stones; 90% hold ASA for ureteral stones. Sixty-six percent of American urologists will stent patients with solitary kidneys and 89% will stent patients with large stones, with a median size to stent of 1.3 cm.
Variation Between Canada and United States
Table 1 summarizes differences between Canadian and American urologists.
Chi-square test.
Fisher's exact test.
C+S = culture and sensitivity; IV = intravenous.
Discussion
SWL is a commonly used stone treatment; until recently, there was a relative absence of evidence-based guidelines regarding the performance of SWL. The recent EAU guidelines are evidence based and may be helpful in standardizing SWL treatment. 8 Our study found that there was considerable variability among urologists regarding the performance of SWL with variability between countries as highlighted in Table 1.
Both the AUA and EAU guidelines recommend screening for asymptomatic bacteriuria before any stone treatment; however, we found that only 51% of Canadian urologists and 55% of American urologists use urine cultures before SWL. Screening for asymptomatic bacteriuria may be underrepresented in this survey as some centers screen with urinary dipstick or urinalysis and not urine cultures in all cases. The AUA guidelines for antibiotic use were updated in 2008 to discontinue recommendation of routine prophylactic antibiotics during SWL. 9 This recommendation appears to have been adopted by Canadian urologists with only 2% using routine antibiotics; however, 78% of surveyed American urologists reported using routine antibiotics.
The 2007 AUA Urolithiasis Guidelines state that SWL is useful for patients “desiring minimal anesthesia” 5 since SWL can be performed using intravenous sedation and analgesia protocols instead of general or regional anesthesia utilized for ureteroscopy or more invasive stone treatments. However, the vast majority, 82% of surveyed American urologists use general anesthesia routinely for SWL compared with only 5% of Canadian urologists. There are, however, potential benefits of SWL under general anesthesia with increased treatment success rates because of decreased patient motion. 10,11
All Canadians used a dose escalation protocol, compared with 87% of Americans. Dose escalation protocols have been theorized to decrease the risk of renal damage during SWL, 12,13 which has been shown in animal models with variable clinical results as outlined in the review by McClain and associates. 14
There is evidence that if SWL is performed while a patient is on antiplatelet medications (ASA and clopidogrel), there may be increased risk of bleeding complications such as subcapsular or perinephric hematomas. 15 –19 Rates of performance of SWL while patients are on antiplatelets were higher in Canada compared with the United States with 88% of Canadian urologists discontinuing ASA for renal stones vs 96% of American urologists. Treatment on nonsteroidal anti-inflammatory drugs (NSAIDs) was more common with 62% of Canadians and 85% of Americans holding NSAIDs before treatment of renal stones. NSAIDs are used at some centers, typically outside North America, in SWL analgesia protocols. 20 –23
SWL efficacy is improved when delivered at a slower shock rate (i.e.: 1–1.5 Hz) compared with 2 Hz. There are randomized controlled trials supporting this for both renal and ureteral stones, 24,25 which have been confirmed by meta-analyses. 26,27 The cost-effectiveness of SWL is also improved when a slower shock rate is utilized because of improved stone fragmentation. 28 Despite this evidence, 76% of Canadian urologists routinely use a rate of 2 Hz. Only 16% of American urologists routinely reported using 2 Hz, with 45% using a rate of 1 Hz and another 41% using a rate between 1 and 1.5 Hz. The drawback of slower shock rate is increased treatment time.
Stents are typically used before SWL to relieve symptomatic obstruction, in cases of infection, or are inserted prophylactically in an attempt to prevent Steinstrasse and post-SWL complications. However, stents may decrease the clearance of stone fragments after SWL. 29 There are cases where pre-SWL stenting may be desired to prevent obstruction—namely solitary kidneys and patients with large stones. Fifty-one percent of Canadian urologists would routinely stent a patient with a solitary kidney vs 66% of American urologists and 58% of Canadian urologists reported routinely stenting patients with large stones vs 89% of American urologists.
This study is limited by its nature as a survey and the differing administration between the Canadian and American groups. The response rate in Canada was excellent (94%); however, the U.S. data were determined by multiple methods, including Endourologic Society survey, and by surveying members of two large stone treatment groups in the United States. As such, no true sample size was calculated for a response rate for urologists in the United States. The results may not be generalizable to all urologists across the United States. The Canadian group also had higher respondents in academic practice (67% of Canadians surveyed vs 30% of Americans surveyed). However, despite more Canadians being in academic practice, Canadians did not follow all evidence-based best practices such as using a lower shock rate of 1 to 1.5 Hz. Despite these limitations, our study suggests that there are significant variations in the performance of SWL between Canada and the United States, including some practice patterns that may result in less than optimal treatment outcomes or potential increased risk for complications. There has been an absence of Canadian guidelines regarding performance of SWL; however, recently published guidelines for treatment of ureteral stones includes some information on improving SWL outcomes. 30
Conclusions
This study found that there are statistically significant differences in SWL practice patterns in Canada compared with the United States, based on survey responses. American urologists who were more likely to use general anesthesia with routine prophylactic antibiotics, at a slower shock rate, were more likely to stent patients with solitary kidneys or large stones and were less likely to treat patients on ASA compared with Canadian urologists. We believe this study supports the use of evidence-based guidelines to standardize pre-SWL work-up and the technical performance of SWL to maximize patient outcomes and minimize potential morbidity and complications.
Footnotes
Acknowledgments
The study authors acknowledge the Endourologic Society, as well as the Midwest Stone Management and Fortec Lithotripsy, with dissemination of the survey to the American respondents.
Author Disclosure Statement
Dr. Honey discloses a financial relationship with Cook Medical. Dr. Pace discloses a financial relationship with Cook Medical. None of these relationships poses a conflict of interest for this research. Drs. Lantz, McKay, Ordon, and Monga have no disclosures.