
Abstract
Introduction:
Traditional techniques for obtaining percutaneous renal access utilize continuous fluoroscopy. In an attempt to minimize radiation exposure, we describe a novel laser direct alignment radiation reduction technique (DARRT) for percutaneous access and test it in a bench-top model.
Methods:
In this randomized-controlled bench-top study, 20 medical personnel obtained renal accesses using both the conventional bullseye technique and the laser DARRT. The primary endpoint was total fluoroscopy time. Secondary endpoints included insertion time, puncture attempts, course corrections, and subjective procedural difficulty. In the laser DARRT, fluoroscopy was used with the C-arm positioned with the laser beam at a 30° angle. The access needle and hub were aligned with the laser beam. Effective caliceal puncture was confirmed with fluoroscopy and direct vision. The Paired samples Wilcoxon signed rank test was used for statistical analysis with significance at p < 0.05.
Results:
A total of 120 needle placements were recorded. Fluoroscopy time for needle access using the laser DARRT was significantly lower than the bullseye technique in all groups as follows: attendings (7.09 vs 18.51 seconds; p < 0.001), residents (6.55 vs 13.93 seconds; p = 0.001), and medical students (6.69 vs 20.22 seconds; p < 0.001). Students rated the laser DARRT easier to use (2.56 vs 4.89; p < 0.001). No difference was seen in total access time, puncture attempts, or course corrections between techniques.
Conclusion:
The laser DARRT reduced fluoroscopy time by 63%, compared with the conventional bullseye technique. The least experienced users found the laser DARRT significantly easier to learn. This novel technique is promising and merits additional testing in animal and human models.
Introduction
I
The two most common methods for establishing percutaneous renal access are the “bullseye” (eye of the needle) and the “triangulation” techniques. 5 Both of these techniques require fluoroscopic guidance. Interestingly, a prior survey distributed to active American Urological Association (AUA) members revealed that only 11% of urologists performing PCNL obtained their own percutaneous access without the assistance of an interventional radiologist. 6 This reluctance is likely multifactorial, but may be partially attributed to concerns regarding the potential for radiation exposure to the surgeon, the inherent difficulty of renal access, and the potential complications associated with this procedure. 7
Variations on the conventional bullseye technique designed to improve the accuracy, simplicity, and safety of renal access by the addition of retrograde ureteroscopy have been reported. 8 –12 However, these techniques still require a significant amount of radiation exposure to both the patient and the operating room staff. In its most recent guidelines, the International Commission on Radiation Protection recommended that radiation exposure not exceed 1 millisievert (mSv)/year in the general population. 13 However, McParland 14 have demonstrated that nephrostomy tube insertion alone requires a mean patient exposure of 6.9 mSv. Of particular concern are young patients and recurrent stone formers who ultimately undergo multiple diagnostic and surgical procedures and thus are subjected to even higher cumulative doses of radiation. This raises valid concerns in light of evidence linking radiation exposure of >5 mSv with an increased cancer risk. 15 For this reason, the United States Food and Drug Administration (FDA) has targeted fluoroscopy as an imaging modality that needs dose optimization and has encouraged the medical community to implement an “As Low As Reasonably Achievable” (ALARA) protocol in their practice. 16
In an attempt to minimize radiation exposure during percutaneous renal access, we describe a novel technique using direct alignment of the percutaneous access needle with a laser aiming beam attachment on the fluoroscopic C-arm system. This laser direct alignment radiation reduction technique (DARRT) is designed to further simplify renal access and to reduce radiation exposure to the surgeon and patient. In this study, the laser DARRT was compared with the bullseye technique using a prospective bench-top model for renal access.
Materials and Methods
In this prospective randomized bench-top study, 20 medical personnel (6 attending physicians, 5 resident physicians, and 9 medical students) were recruited to perform percutaneous renal access in a bench-top model using both the laser DARRT and the conventional bullseye technique. A collagen-based six-layered kidney model was designed to simulate the muscle and fascia layers penetrated during percutaneous renal access and included a transparent plexiglass base so that effective caliceal puncture could be visually confirmed after each trial (Fig. 1). In this model, the kidney was constructed out of dense gelatin, while the calices were made from three shortened fingers of a latex glove that was embedded in the gelatin kidney model. The palm of the latex glove simulated the renal pelvis, and the wrist of the glove was connected to an end-hole catheter for injection of half-strength contrast during needle insertion (Figs. 1 and 2). Three layers of carpet padding were used to simulate the skin and subcutaneous tissue, muscular and fascial layers of the flank, and Gerota's fascia. The outer and inner gelatin layers simulated the renal capsule and parenchyma, and the latex glove simulated the collecting system (Fig. 1). The model concept was based on a previously described effective model. 17

Renal bench-top model as seen from below with the upper pole

A clamp is positioned over the desired upper pole renal calix. Alignment of the laser beam with the tip of the clamp and the desired calix allows for orientation of the needle during insertion without the use of continuous fluoroscopy.
A GE OEC 9900 portable C-arm with an attachable laser aiming beam (GE Medical system, Inc. Salt Lake City, UT) mounted upon the image intensifier was used to direct caliceal puncture (Fig. 3). In the laser DARRT, fluoroscopy was used to select the needle entry site on the simulated skin above the calix of interest. The C-arm was then positioned with the laser beam on the simulated skin over the desired access site at a 30° angle to simulate percutaneous access in a clinical patient (Fig. 4).
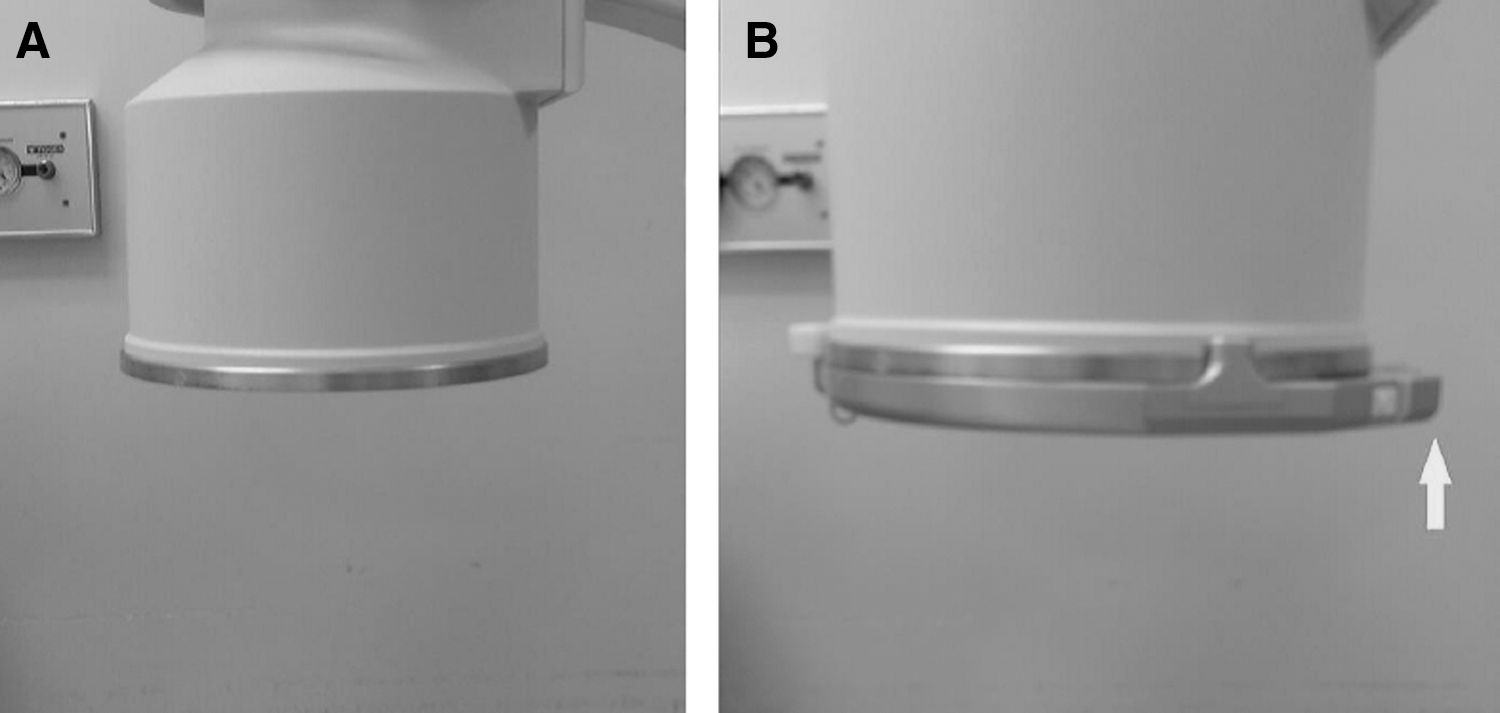

Operator placing the C-arm laser beam over the desired calix utilizing fluoroscopy.
An 18-gauge Chiba needle was placed with the tip at skin level at the site indicated by the laser aiming beam. While holding the tip in position in line with the laser beam, the needle was then rotated so that both the needle tip and hub were in alignment with the laser. This was confirmed by the illumination of the needle hub from the laser (Fig. 5). The needle was then inserted into the renal calix using tactile feedback, while maintaining alignment with the laser. The surgeon then rotated the C-arm 30° in the opposite direction to establish the needle depth. Effective caliceal puncture was confirmed by an objective reviewer by looking through the clear undersurface of the model.

Alignment and illumination of the needle hub by the laser allow advancement of the needle without fluoroscopy.
In the conventional bullseye technique, fluoroscopy was utilized to select the needle entry site above the calix of interest. The hub of the needle was grasped with a long Kelly clamp, and the needle was inserted using continuous fluoroscopy to maintain alignment. Needle depth and correct needle location were confirmed in an identical manner to the DARRT.
Each subject obtained needle access to the upper pole, interpolar, and lower pole of the kidney model using both techniques. Subjects were randomized to starting location and technique using a prospective crossover design. The primary endpoint was total fluoroscopy time. Secondary endpoints included insertion time, number of puncture attempts, number of course corrections, and subjective procedural difficulty, which were graded using a Likert scale from 1 to 10 (10 being the most difficult). The Paired samples Wilcoxon signed rank test was used for statistical analysis, with p < 0.05 considered significant.
Results
Overall, a total of 120 trials were performed (60 conventional and 60 laser DARRT), all of which ultimately resulted in effective caliceal puncture. Overall fluoroscopy time was significantly lower when using the laser DARRT than when using the conventional technique (6.77 vs 18.22 seconds; p < 0.001). When stratified by level of experience, all groups demonstrated a significant reduction in fluoroscopy time using the laser DARRT, including the attending physicians (7.09 vs 18.51 seconds; p < 0.001), resident physicians (6.55 vs 13.93 seconds; p = 0.001), and medical students (6.69 vs 20.22 seconds; p < 0.001) (Fig. 6).

Fluoroscopy time was significantly shorter with the laser DARRT compared with the bullseye technique for each group. DARRT = direct alignment radiation reduction technique.
When asked to rate the ease of performing the technique for each trial on a 1 to 10 Likert scale, the medical students rated the laser DARRT easier to use (2.56 vs 4.89; p < 0.001), while a nonsignificant trend toward ease of use was reported by the attending physicians (2.39 vs 3.44, p = 0.146) and resident physicians (3.60 vs 4.53, p = 0.144) (Fig. 7).

Medical students found the laser DARRT easier to use.
No difference was seen in total access time (118 vs 107 seconds; p = 0.317) (Fig. 8), puncture attempts (1.05 vs 1.07; p = 0.317), or course corrections (0.33 vs 0.30; p = 0.595) between the different techniques for the combined cohort.
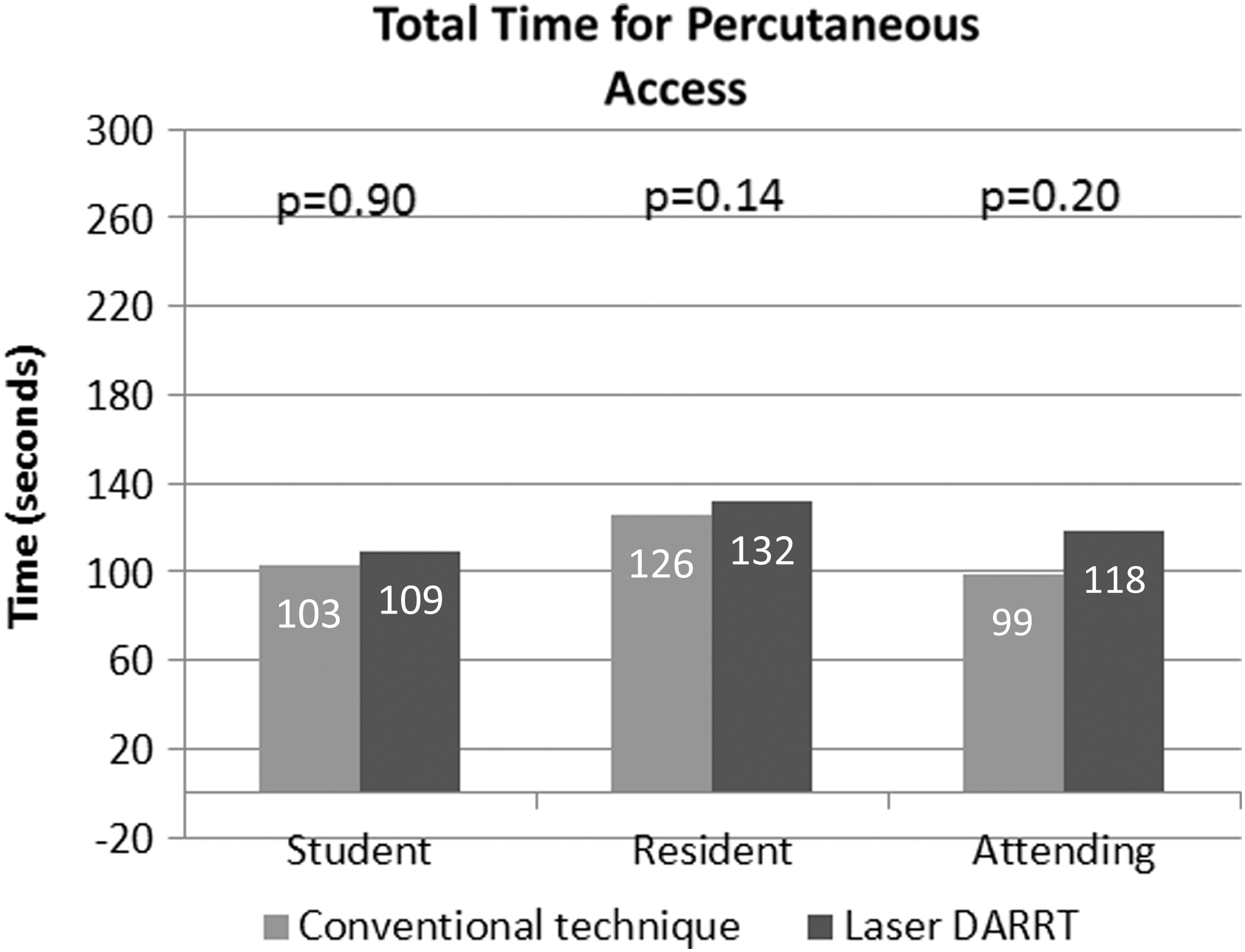
Total elapsed procedure time for percutaneous access did not differ between techniques.
Discussion
Since the introduction of PCNL in the 1970s, 1 various imaging modalities have been utilized to achieve accurate percutaneous renal access and to minimize associated complications. Currently, fluoroscopy is being widely used for guiding the “bullseye” and “triangulation” techniques to establish percutaneous caliceal access. Advantages of this modality include good image quality of the collecting system with the use of contrast and the ease of visualization of needle and nephrostomy tube during insertion. 18 A major drawback is the accompanying risk of ionizing radiation exposure to both the patient and operating room staff. In two published series of 282 and 100 patients undergoing PCNL, total fluoroscopy time averaged 10.19 and 4.5 minutes, respectively. 19,20 Lipkin et al. 21 simulated PCNL in a 73 kg adult male phantom using median fluoroscopy times of 386.3 and 545.0 seconds for left and right PCNL, respectively, and calculated effective doses of 8.11 and 7.63 mSv.
Long-term follow-up of the Japanese atomic bomb survivor cohort demonstrated 44 excess solid cancer deaths out of a total of 3277, for those exposed to 5 to 100 mSv. This study also reported that for those exposed at age 30, the risk of solid cancer is elevated by 47% per Sv at age 70. 22 Subsequently, the stochastic (nondose related) genetic effects and cancer risks of radiation exposure cannot be overlooked. 23,24
In addition, radiation exposure is known to be associated with increased cardiovascular mortality rate. Excess relative risk of mortality rate due to stroke and heart disease has been estimated at 9% and 14% per Gy, respectively, at more than 50 years of follow-up in the Japanese atomic bomb survivor cohort. 25
Previous authors have described the use and success of laser guidance systems to achieve accurate target localization and reduce overall radiation doses. In an attempt to improve access precision, Ritter et al. 26 used a laser guidance system combined with a multiplanar CT reconstruction to perform percutaneous renal access. The disadvantage of this technique was the considerable increase in radiation exposure compared with standard fluoroscopy and the need for additional equipment in the operating room. Another study by Moser et al. 27 demonstrated that their novel laser guidance system reduced patient radiation exposure and improved accuracy of CT-guided spinal injections, when compared with the traditional free-hand technique. Also, similar to our study, laser targeting with C-arm reduced fluoroscopy time by 19% to 39% during orthopedic surgical procedures upon the hip and ankle. 28 In addition, Collins et al. 29 demonstrated that laser-guided targeting in a turkey breast and olive phantom was more user friendly, easier to perform, and required less procedural time with novice users, when compared with free-hand puncture.
With percutaneous renal access being mostly a free-hand procedure, our study reflects the effective application of laser guidance in the urologic setting and also demonstrates both radiation reduction and ease of performance in novice users. In addition, the laser DARRT does not require continuous fluoroscopy during needle advancement. This may allow the surgeon to feel the subtle tactile feedback as the needle passes the renal capsule and enters the collecting system that may be difficult to appreciate if the surgeon is holding the needle with a clamp or other tool to move the surgeon's hand out of the radiation beam. Recurrent stone formers, young adults, children, and pregnant patients may benefit the most from use of the laser DARRT PCNL. However, all patients, surgeons, and operating room staff could also benefit from the reduced radiation exposure associated with this technique. In addition, the simplicity of the technique could facilitate training of inexperienced surgeons and could potentially allow a greater number of urologic surgeons to obtain their own access in the operating room.
Despite the initial effective application of this novel technique, the results must be viewed in light of the limitations of this study. First, this was a proof-of-concept bench-top study. The model does not completely take into account several variables that would be encountered during in vivo testing, such as respiratory motion, tract length, and patient body habitus. In addition, the use of an artificial kidney model may not completely reproduce the exact characteristics of living tissue, although the interface between the gelatin parenchyma and the surgical glove representing the collecting system was quite realistic. In future clinical testing, coordinating laser localization and needle insertion, while anesthesia performs breath holding, would be a crucial step to control kidney motion. In addition, this technique requires the use of an attachable laser aiming beam that may not be available in all centers. Also, since this study measured only the ability of the surgeon to insert the needle into the desired calix, it did not determine the total fluoroscopy time required for PCNL in either technique. In addition, this study did not take into account the obstructing effect of a large staghorn calculus and the added difficulty that may be encountered while trying to pass the wire down into the ureter. This limitation could potentially be overcome by using a retrograde ureteroscopic-assisted technique for wire capture and delivery into the proximal ureter, as has been previously published. 8 –12 Finally, one limitation of the laser aiming beam is that it projects a faint square in the center of fluoroscopy screen, but as the surgeon is aware of this limitation, it has little impact upon the ability to interpret the image. Despite these limitations, the laser DARRT shows promise as a method to facilitate needle access of the kidney that is easy to learn and reduces radiation exposure in surgeons of all experience levels.
Conclusion
The laser DARRT for percutaneous renal access reduced fluoroscopy time by 63%, compared with the conventional bullseye technique in this preliminary bench-top study, without increasing total access time, number of puncture attempts, or number of course corrections. The least experienced users found the laser DARRT significantly easier to learn. This is a promising new technique that merits additional testing in animal and human models.
Footnotes
Author Disclosure Statement
Dr. D. Duane Baldwin: Lecturer for Cook, Research grant from Teleflex, consultant for Bard, consultant for Boston Scientific, MedDevCo chief science officer. For all remaining authors: No competing financial interests exist.