
Abstract
Introduction:
Partial or complete obstruction of the urinary tract is a common and challenging urological condition that may occur in patients of any age. Serum creatinine is the most commonly used method to evaluate global renal function, although it has low sensitivity for early changes in the glomerular filtration rate or unilateral renal pathology. Hence, finding another measurable parameter that reflects the adaptation of the renal physiology to these circumstances is important. Several recent studies have assessed the use of new biomarkers of acute kidney injury (AKI), but the information among patients with stone disease and those with obstructive uropathy is limited.
Material and Methods:
A prospective cohort study was conducted to determine the urinary levels of kidney injury molecule-1 (KIM-1), Total and Monomeric neutrophil gelatinase-associated lipocalin (NGAL) in patients with hydronephrosis secondary to renal stone disease, congenital ureteropelvic junction obstruction or ureteral stricture. Comparison between patients with hydronephrosis and no hydronephrosis was carried out along with correlation analysis to detect factors associated with biomarker expression.
Results:
Urinary levels of KIM-1 significantly decreased after hydronephrosis treatment in patients with unilateral obstruction (1.19 ng/mL vs 0.76 ng/mL creatinine, p = 0.002), additionally KIM-1 was significantly higher in patients with hydronephrosis compared to stone disease patients without radiological evidence of obstruction (1.19 vs 0.64, p = 0.006). Total and Monomeric NGAL showed a moderate correlation with the presence of leukocyturia. We found that a KIM-1 value of 0.735 ng/mg creatinine had a sensitivity of 75% and specificity of 67% to predict the presence of hydronephrosis in preoperative studies (95% CI 0.58–0.87, p = 0.006).
Conclusion:
Our results show that KIM-1 is a promising biomarker of subclinical AKI associated with hydronephrosis in urological patients. NGAL values were influenced by the presence of leukocyturia, limiting its usefulness in this population.
Introduction
P
KIM-1, has a immunoglobulin-like domain, specifically located in the apical membrane of proximal tubular cells, and is highly expressed after cell injury. 5 –7 Some case–control studies have found elevated urinary levels of KIM-1 in patients with obstructive nephropathy compared to controls. 4,8,9 NGAL is polypeptide chain that belongs to the lipocalin superfamily, and has been involved in multiple processes such as apoptosis, innate immunity, and renal development. 10 –12 It has been found to be a sensitive and early marker of AKI, and as a marker of inflammatory and infectious processes. 13 –17 Three isoforms of NGAL have been studied, and the monomeric form appears to be most specific for tubular epithelial damage. 12,18,19
Postrenal causes of kidney injury, which are associated with bilateral or unilateral hydronephrosis, are of particular interest to urologists because appropriate and timely intervention can prevent renal failure. Moreover, the timely management of obstructive processes, especially if unilateral or associated with subclinical AKI, may be delayed in the absence of an abnormal SCr. The biomarkers of AKI may replace SCr as an objective measure of renal function, especially if found to be measurable in blood and urine hours before significant elevations of SCr, or during a subclinical AKI episode. Multiple clinical questions still remain, however, about their clinical usefulness, especially in urological patients. To assess the potential utility of these markers in urological patients, and based on the fact that urinary tract obstruction (UTO) may cause subclinical AKI, we conducted this prospective cohort study. The main objective was to determine the urinary levels of KIM-1, Total and Monomeric NGAL, before and after treatment, in urological patients with hydronephrosis, and in a group of patients with stone disease without hydronephrosis.
Materials and Methods
This prospective cohort study was approved by the Western University Health Science Research Ethics Board (REB #106204), and included three groups: patients with unilateral hydronephrosis (Group 1), patients with stone disease and no hydronephrosis (Group 2), and healthy subjects as controls (Group 3). According to previous data about KIM-1 concentration in urine from our center, 20 we estimated a sample size of 24 patients with hydronephrosis to detect a two-sided difference in KIM-1 levels before and after the intervention (α = 0.05, with a power of 0.90 and a calculated effect size of 0.7). 21 Group 1 consisted of 24 patients with unilateral hydronephrosis caused by intrinsic ureteric stricture or unilateral stone disease amenable to treatment by ureteroscopy (URS), percutaneous nephrolithotomy (PCNL), or pyeloplasty. Group 2 included patients with evidence of stone disease without radiological evidence of hydronephrosis requiring surgical treatment. All patients with bilateral stone disease, active urinary tract infection, preoperative presence of ureteric stent, use of indwelling bladder catheter, or recent history of sepsis were excluded from the study. A group of healthy subjects without history of renal stone disease and normal urinalysis and bilateral renal ultrasound was also included (Group 3).
Demographical, clinical, and radiological variables were prospectively collected. The grade of hydronephrosis was determined by evaluating preoperative CT scans or renal ultrasound images as described by Fernbach and Ito. 22,23 Comorbidities were evaluated using the Charlson Comorbidity Index (CCI). 24 SCr was measured in all patients before the surgical procedure and the estimated glomerular filtration rate (eGFR) was calculated using the CKD-EPI formula. 25 Mid-stream preoperative and postoperative urine samples were collected for urinalysis and creatinine measurement, which was used to normalize biomarker levels. All samples were centrifuged within 2 hours of collection at 1000 rpm for 1 minute at room temperature and aliquots of 1 mL were stored at −80°C for further biomarker analysis, as recommended by Parikh. 26 AKI marker analysis was performed after finishing the recruitment phase; it comprised three different ELISA assays that were run in duplicate with the recommended dilutions according to the manufacturer's instructions: KIM-1 (Human TIM-1/KIM/HAV; R&D Systems, Minneapolis, MN), Total NGAL, and monomeric NGAL (Bioporto Diagnostics, Hellerup, Denmark). All patients who completed the follow-up had postoperative imaging studies to rule out the presence of residual stones or hydronephrosis.
Baseline demographic, clinical, and biochemical characteristics were compared between the two groups and the controls. Dichotomous variables were analyzed using Chi-square and continuous variables were compared with Student T-test or Mann–Whitney U test. Median levels of preoperative and postoperative biomarkers were compared using Wilcoxon signed rank test. Correlations between ordinal and continuous variables with the urine marker levels were evaluated with Spearman Rank correlation. Receiver operating characteristics (ROC) curve analysis was used to determine the diagnostic performance of any biomarker to detect hydronephrosis. Statistical analysis was performed with SPSS v.20 (IBM, Armonk, NY), p values were derived from two-tailed test, and a p < 0.05 was considered statistically significant.
Results
From 66 initially recruited patients, 44 patients completed follow-up, 24 from Group 1 and 20 from Group 2. Eleven healthy subjects were included in Group 3 (Fig. 1). Stone disease was the most common cause of obstruction in the hydronephrosis group (22/24 patients), while one patient had congenital ureteropelvic junction obstruction and one had an acquired ureteric stricture. At last follow-up all Group 1 patients were stent free, 21 had negative studies for hydronephrosis and 7 had residual stone fragments.
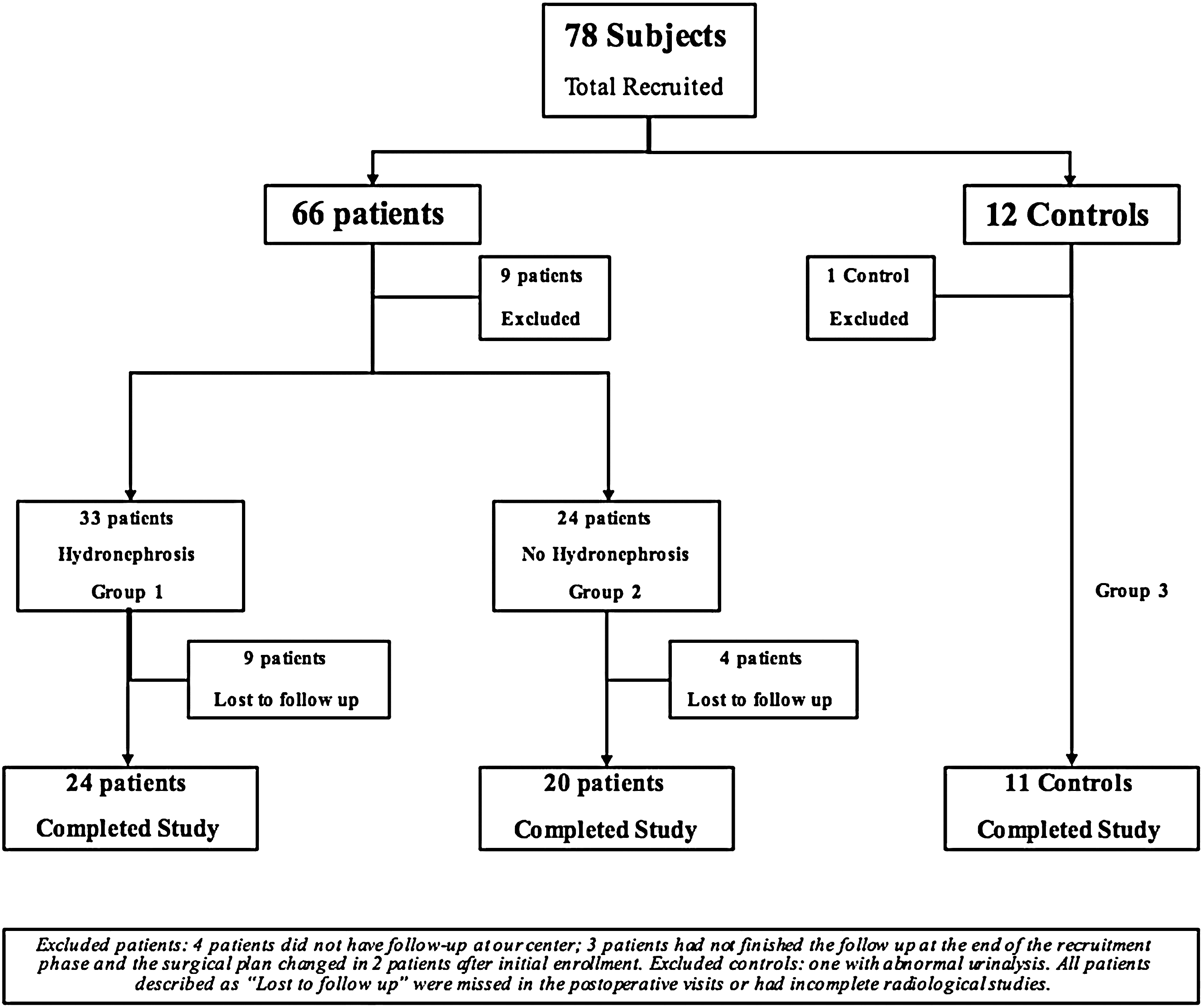
Flowchart of patients recruited and patients included in the final analysis.
Demographic characteristics were similar between patients and controls. Table 1 shows the clinical and radiological characteristics of the hydronephrosis group and the comparison in the urinary levels of AKI markers. The distribution of the three biomarkers median levels was statistically significantly different between Group 1 and controls (Fig. 2). Moreover, a Kruskal–Wallis analysis comparing the baseline levels of the three biomarkers showed significant differences (p < 0.01) between the three groups.

Boxplot graph showing the distribution of normalized values of biomarkers in patients with hydronephrosis and controls. NGAL = neutrophil gelatinese-associated lipocalin.
Chi-square test for categorical variables and Student T-test or Mann–Whitney-U test for continuous data. Bold values show statistically significant differences between both groups.
ABS = absolute; CCI = Charlson Comorbidity Index, eGFR = estimated glomerular filtration rate; mNGAL = monomeric neutrophil gelatinese-associated lipocalin; NORM = normalized values expressed in ng/mg creatinine; SCr = serum creatinine.
Postoperative assessment was conducted with a median of 68 days (IQR 47) after the surgical procedure. Except for three patients, all other individuals from Group 1 showed a decreased urinary level of KIM-1 in the postoperative visit compared to the preoperative concentration. One patient had Chronic Kidney Disease and residual hydronephrosis associated with a longstanding ureteral stricture, the other two only showed leukocyturia and residual stone disease. After resolution of the hydronephrosis, KIM-1 concentration in Group 1 decreased to levels that were statistically similar to those in the control group (0.76 ng/mL vs 0.36 ng/mL creatinine, p = 0.36). Figure 3 illustrates the change in the postoperative levels of KIM-1 after surgical management of the 24 patients in the hydronephrosis group compared to the preoperative assessment. KIM-1 levels were statistically significantly lower after treatment (p = 0.002). However, no significant differences in the Total and Monomeric NGAL levels were found (Table 2 and Fig. 4).
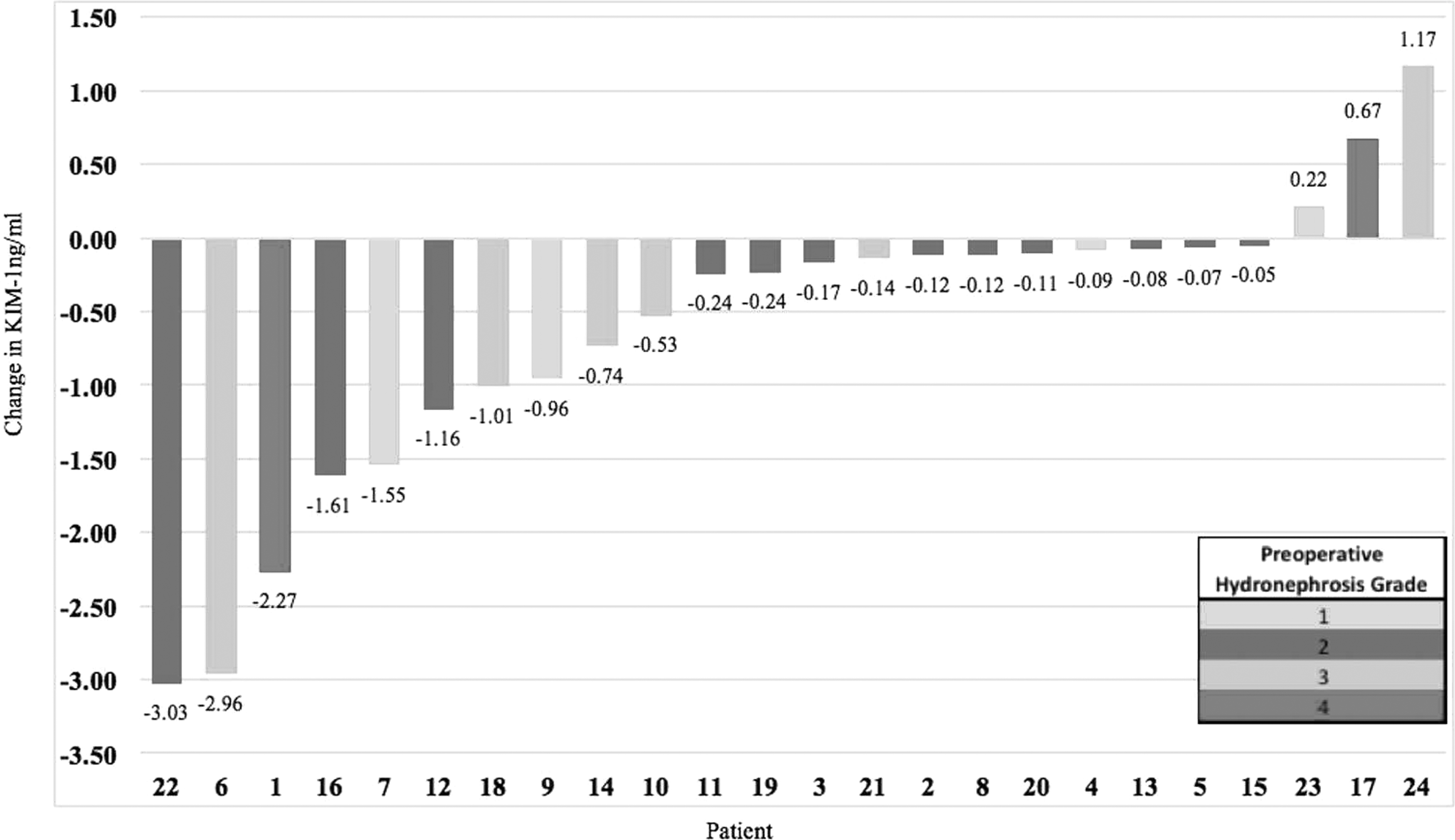
Waterfall plot showing the change in KIM-1 levels before and after treatment in all patients from the hydronephrosis group.
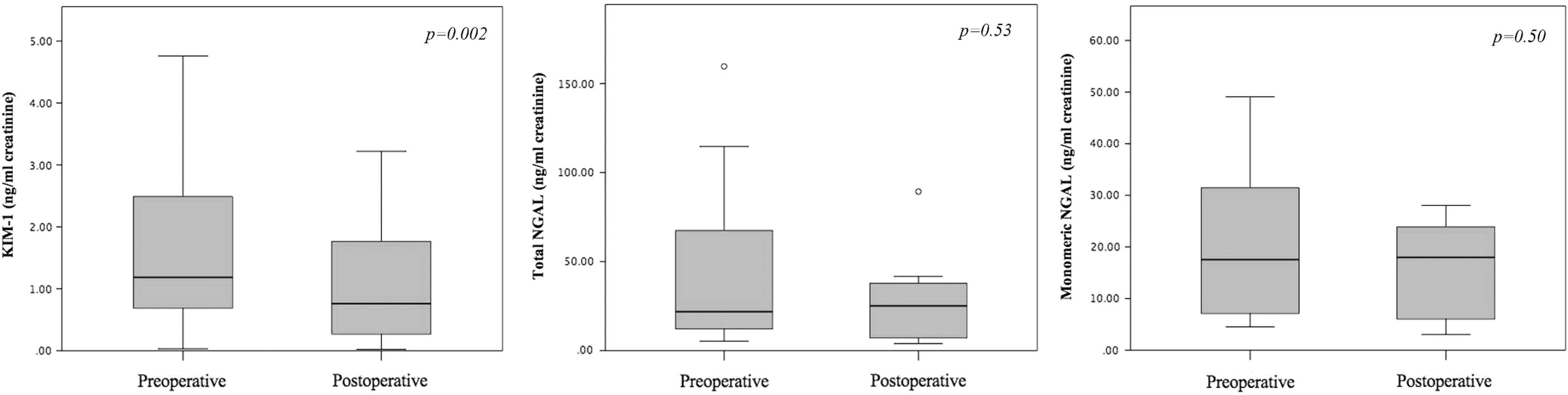
Boxplot graph showing the distribution of normalized values of biomarkers in patients with hydronephrosis before and after treatment.
Normalized biomarkers levels are express in ng/mg creatinine.
Wilcoxon signed rank test.
Considering that three patients had residual hydronephrosis and seven residual stone fragments after treatment, a post hoc analysis was performed by excluding these postoperative samples. Results were similar, showing only significant differences in KIM-1 levels, after comparing 24 vs 21 patients (residual hydronephrosis) and 24 vs 15 (residual hydronephrosis/stones).
Demographic, radiological, and biochemical characteristics of Group 1 and 2 are shown in Table 3. Both groups were comparable in terms of age, gender, comorbidities, and previous history of stone disease. Besides the obvious disparity in the hydronephrosis status, we found differences in the number of patients diagnosed after an episode of renal colic, the stone size, and the baseline SCr (p < 0.05). Patients with hydronephrosis had significantly higher levels of KIM-1 compared to patients without hydronephrosis (p = 0.006). Monomeric and Total NGAL did not show a significant difference between the two groups. After comparing the postoperative levels of biomarkers in the two groups, we did not find differences in KIM-1 (p = 0.81), Total NGAL (p = 0.89), or Monomeric NGAL (p = 0.37). Interestingly, baseline and postoperative KIM-1 levels expressed by Group 2 patients were similar to the median values observed in the control group (0.64 ng/mL vs 0.36 ng/mL creatinine, p = 0.88, 0.75 ng/mL vs 0.36 ng/mL creatinine, p = 0.36, respectively).
Categorical variables were compared using Chi-square test; continuous variables were compared with Student T-test or Mann–Whitney U test.
Bold values show statistically significant differences between both groups.
BMI = body mass index.
KIM-1 was the only biomarker showing a significant correlation with the grade of hydronephrosis (rs = 0.39, p = 0.002). None of the biomarkers showed a significant correlation with the renal function measured by SCr or eGFR. The grade of leukocyturia in the preoperative sample showed a moderate correlation with the levels of Total (rs = 0.43, p = 0.007) and Monomeric NGAL (rs = 0.45, p = 0.001), and similar correlations were found evaluating the postoperative urine sample. These associations remained significant after adjusting for age and comorbidities. Patients showing leukocyturia in the preoperative urine sample had significantly higher levels of Total and Monomeric NGAL (p = 0.016, p = 0.010) than those patients without leukocyturia, independently of the group they belonged to. KIM-1 was not associated with the presence of leukocyturia (p > 0.05). Using ROC curve analysis, we found that a KIM-1 value of 0.735 ng/mg creatinine had a sensitivity of 75% and specificity of 67% to predict the presence of hydronephrosis in preoperative studies, with an area under the curve of 0.73 (95% CI 0.58–0.87, p = 0.006; Fig. 5).
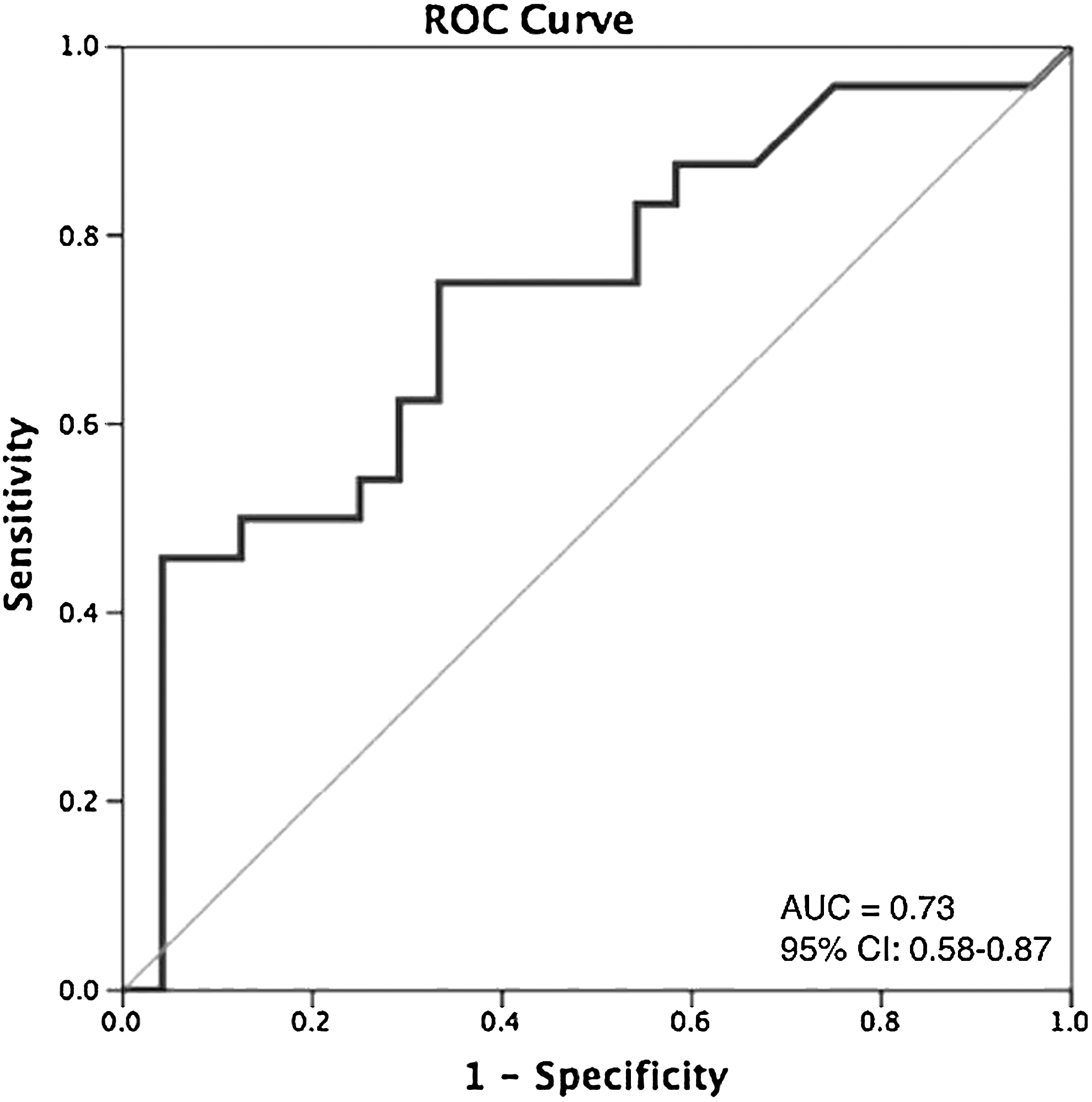
ROC curve for hydronephrosis detection using KIM-1 (0.735 ng/mg creatinine).
Discussion
We evaluated three AKI biomarkers in urological patients, including Monomeric NGAL previously reported to be more specific than Total NGAL for renal tubular injury. Patients with hydronephrosis had significantly higher levels of the three biomarkers compared to controls; they also showed higher levels of KIM-1 at baseline evaluation than after obstruction relief. Likewise, KIM-1 expression was significantly higher compared to patients with stone disease without obstruction. We also proved that the grade of hydronephrosis positively correlated with the expression of KIM-1. Total and monomeric NGAL levels were not affected by the presence of hydronephrosis, conversely their expression correlated with the grade of leukocyturia.
Elevated levels of urinary KIM-1 in patients with hydronephrosis supports the idea that UTO may cause subclinical AKI despite the presence of normal SCr levels. We acknowledge our results for the hydronephrosis group and Total and Monomeric NGAL could be due to the small sample size. The correlation observed with leukocyturia noted in this study and others warrants further investigation. 13,15,27
In a cross-sectional study, Urbschat and colleagues evaluated Total NGAL and KIM-1 in patients with “acute obstructive nephropathy.” Their results are in contrast to our findings: KIM-1 was similar between controls and patients, and NGAL was statistically significantly different. Outcomes might be distinct because all included patients were considered to have postrenal AKI, despite the presence of hydronephrosis or the SCr level. Additionally, subjects with renal colic without hydronephrosis were included in the study group, and they may have exhibited systemic inflammatory response symptoms (SIRS), which could affect NGAL levels. 28 We only included patients without an urgent indication for active management, excluding those patients with SIRS and eliminating a potential confounding factor for biomarkers' evaluation.
None of the three evaluated biomarkers showed a significant correlation with global renal function. 29 The absence of SCr values in the control group and in the postoperative evaluation is the most important shortcoming of this study. Despite the dropout rate, the number of patients included in the final analysis was sufficient to corroborate the findings according to the calculated sample size. While it is true that obstruction can affect the biomarkers' concentration in the bladder, it is more clinically relevant than measuring concentrations from the affected side. Whether KIM-1 has a protective role in cases of acute injury, or promotes a fibrotic process by its chronic expression during the obstructive process remains to be determined. 30,31
Conclusions
Our results suggest that urinary KIM-1 has the potential to become a useful biomarker for subclinical AKI associated with hydronephrosis. The significance relies not only in the possibility of identifying a urinary marker of obstruction, but also in the ability to measure the grade of renal injury allowing for modification of treatment paradigms.
Footnotes
Acknowledgments
The authors acknowledge that the unabridged version of this research has been submitted as a Master's in Science degree thesis of the first author in the Western University Electronic Thesis and Dissertation Repository. We also would like to thank Linda Nott, Patricia Rosas-Arellano, and all the Urology Clinic Staff for their commitment to this research project. The study was partially funded by an unrestricted Internal Research Fund award granted to the investigation team by the Department of Surgery, Schulich School of Medicine & Dentistry.
Author Disclosure Statement
No competing financial interests exist.