
Abstract
Introduction:
To detect safety and feasibility of miniperc and extracorporeal shockwave lithotripsy (SWL) for treatment of average-sized (1–2 cm), radiopaque lower pole calculi in a prospective randomized manner.
Patients and Methods:
In the period from January 2014 to June 2015, 150 patients were attached to this study with single lower pole radiopaque stone ranging from 10 to 20 mm. Patients were divided randomly into two groups using computer-generated randomization in an equal manner. First group patients were subjected to miniperc procedure, while second group patients underwent SWL. Patient's characters, stones' characters, fluoroscopic time, operative time, blood transfusion, hospital stay, retreatment, auxiliary procedure (AP), and complications using modified Clavien grading are tabulated and analyzed.
Results:
This study included two equal groups with 75 patients in each group. With regard to age (37.75 ± 11.25 vs 40.55 ± 10.55), body mass index (26.92 ± 2.26 vs 27.29 ± 2.87), and stone size (1.55 ± 0.28 vs 1.57 ± 0.26), there was no significant statistical difference in both groups. Stone-free rate (SFR) (76% vs 96%), operative time (44.81 ± 7.06 vs 93.37 ± 12.29 minutes), fluoroscopy time (53 ± 2.45 vs 180 ± 7.31 seconds), hospital stay (5.72 ± 1.01 vs 45.19 ± 8.48 hour), and blood transfusion were significantly more in the miniperc group. Retreatment rate (45.3% vs 2.7%) and AP (24% vs 4%) were significantly greater in the SWL group.
Conclusion:
SWL is less invasive than percutaneous stone removal, but it is also less effective for lower pole radiopaque calculi. Miniperc has better SFR and lower auxiliary and retreatment rates; however, it resulted in more drawbacks.
Introduction
Renal stone disease is a common medical problem with prevalence of 6% to 9% in men and 3% to 4% in women and this appears to be increasing.
1
Management of renal stones differs according to stone location, size, and type. Lower caliceal stone is an old dilemma (to manage or not, extracorporeal shockwave lithotripsy [SWL] and anatomical configuration of the lower calix that affect stone clearance). Another controversy is the treatment options of stone size between 1 and 2 cm in the lower calix.
2
Treatment options for 1 to 2 cm lower caliceal renal stones include miniperc, retrograde flexible ureteroscopy (F
Patients and Methods
In the period from January 2014 to June 2015, 150 patients were attached to this study from the outpatient clinic, Benha University Hospital, after giving written consent. The study was approved by the local ethics committee of Benha faculty of medicine. All adult patients with single, lower pole radiopaque stone ranging from 10 to 20 mm in the largest dimension were subjected to this study. Patients with active urinary tract infections (UTIs), uncorrectable coagulopathies, stone in caliceal diverticulum, renal failure, pregnancy, urinary tract tumors, and congenital anomalies in the kidney, such as horseshoe kidney, ectopic pelvic kidney, single kidney, and obstruction at any level of the urinary tract, were excluded from this study. Patients were randomly divided into two groups in an equal manner. First group patients were subjected to the miniperc procedure, while second group patients underwent SWL. All patients were assessed preoperatively by medical history, general and local physical examination, routine laboratory investigation, including urine analysis and culture, complete blood picture and coagulation profile, and renal and liver function. Radiological investigations included pelviabdominal ultrasound (US), plain X-ray urinary tract (PUT), intravenous urography, and noncontrast pelviabdominal spiral CT urinary tract in some cases. Patients were counseled concerning the pros and cons of miniperc and SWL for a given stone (Figure 1).
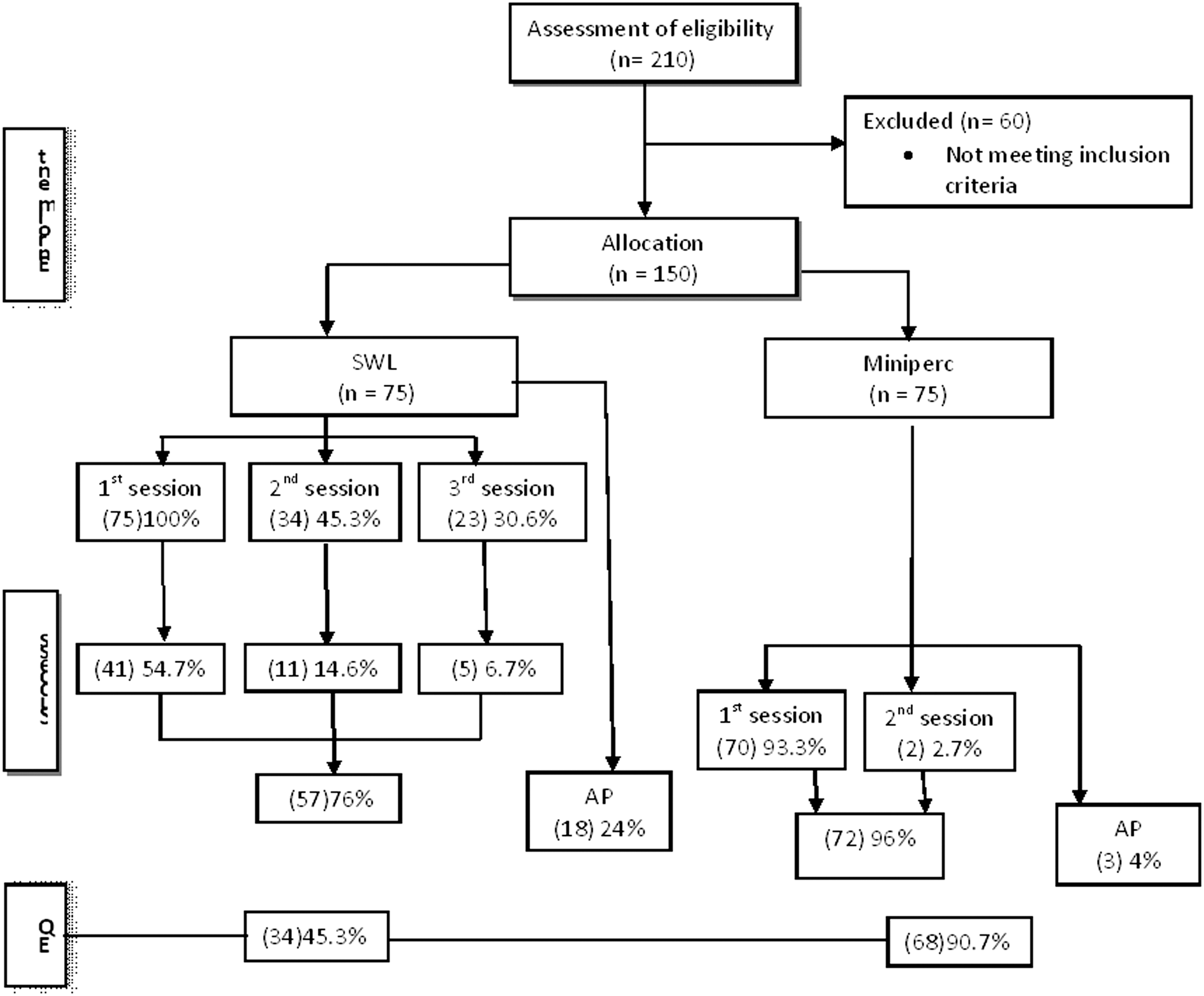
Patient flow diagram.
Miniperc technique
The procedure was done in supine position under general anesthesia (fentanil 2 μg/kg, then propofol was administered until loss of consciousness and maintained with a continuous infusion of 75 μg/kg/minute. Atracurium was given for endotracheal intubation at a dose of 0.5 mg/kg and maintained with a continuous infusion of 0.4 mg/kg/hour). Cystoscopy was done to insert a 6F ureteral catheter. The stone was localized using fluoroscopy and gaining access to the stone through the mid-axillary line. Then, dilatation was done using Amplatz dilators as much as 16F. Semirigid short ureteroscope (9–11F) was used as a miniperc device for stone retrieval and fragmentation by pneumatic lithotripsy and extraction of the fragments by forceps or tipless Dormia basket. At the end of the procedure, a 12F nephrostomy tube was fixed. Stone clearance was assessed at the end of the procedure by a combination of fluoroscopy and ureteroscopy. Routine PUT postoperative was performed if there was no confidence in the intraoperative assessment. If the patient was stone free, the ureteral and the urethral catheters were removed after 1 day, the nephrostomy tubes were clamped on the 2nd day for 2 hours, and removed if there was no leakage, pain, or fever.
SWL technique
In this group, all patients were subjected to SWL under light anesthesia (Midazolam, propofol infusion, and fentanyl) using the mobile electrohydraulic spark gap lithotripter (MT2-RX, BMA for design industry corp.). An average of 3000 shocks was delivered at an average energy level of 17 kV with a frequency of 60 to 90 shockwaves/min during each session. Two kidney, ureter, and bladder radiograph images (vertical and oblique positions) are taken before the SWL treatment to align the focal point of SWL. Patients were assessed 2 weeks after the session by PUT and pelviabdominal US, and if there were residuals, another sitting was done, as much as three sessions. The procedure was considered efficient if the patient was completely stone free or with presence of clinically insignificant residual fragment ≤3 mm.
Retreatment was outlined as using the original procedure for the second time, while an auxiliary procedure (AP) was outlined as using other techniques rather than the original one to achieve the patient's stone-free condition. The preoperative data (patient's characters and stones' characters) of both groups with regard to sex, age, body mass index (BMI), stone side, and stone size are recorded and tabulated. In addition, fluoroscopic time, operative time, blood transfusion, hospital stay, retreatment, and AP and complications using modified Clavien grading are recorded.
Statistical analyses
Software (SPSS, Version 16.0 for Windows; SPSS, Inc., Chicago, IL) was used for the univariate, bivariate, and stratified analyses of the data. Qualitative variables were analyzed by constructing contingency tables with Pearson x 2-test, Fisher exact test, and z-test, when conditions for the former were not met. Student's t-test was applied for the comparison of quantitative variables after establishing their normal distribution by mean and standard deviation. Differences were considered significant with p < 0.05 taken to indicate statistical significance.
Results
This study included 75 patients in the SWL group and an equal number in the miniperc group. With regard to age, sex, BMI, stone laterality, and stone size, there was no statistically significant difference between groups (Table 1). Operative time, fluoroscopy time, hospital stay, and blood transfusion were significantly higher in the miniperc group. Multiple sessions were needed in the SWL group, leading to significantly higher retreatment rate, 34 patients (45.3%) needed a second session, and 23 patients (30.6%) needed a third session. Two patients in the miniperc group needed a second session. This was due to dysfunction of the lithoclast machine during the study period.
Patient Demographics and Stone Criteria
Student's t-test.
Chi-square test.
BMI = body mass index; SD = standard deviation; SWL = extracorporeal shockwave lithotripsy.
The need for APs was greater in the SWL group. In the SWL group, stones were not fragmented in 7 patients, and significant residual fragments were recorded in 11 patients after three sessions. In total, 18 patients underwent miniperc as an AP.
SWL was planned for the two patients with significant residual fragments after miniperc. One patient had persistent urinary leakage after miniperc, which was managed by Double-J stenting.
SFRs after the first, second, and third sessions of SWL were 54.7%, 69.4%, and 76%, respectively. The overall SFR (postoperative 3 months) of SWL vs miniperc was (76%, 96%). The efficiency quotient (EQ) for both groups was determined by using the standard formula: EQ = percent of stone free × 100/(100% + percent of retreatment + percent of APs). The overall outcome in terms of the EQ was also significantly better for miniperc than for SWL (90.7% vs 45.3%) (Table 2)
Treatment Success
Student's t-test.
Fisher exact test.
Chi-square test.
Asterisks indicate significant difference.
EQ = efficiency quotient; SFR = stone-free rate.
Table 3 summarized the complications of both procedures according to modified Clavien classification. 12
Complications
MCG = modified Clavien grade; UTIs = urinary tract infections.
Discussion
The available treatment methods for 1 to 2 cm lower caliceal stones pose a dilemma for physicians and patients. 13 The aim of renal stone treatment is achieving the maximum SFR with the least morbidity. 14 SWL is an attractive treatment modality because of its wide availability, easy usage, safety, and efficacy. 15 Miniperc has fewer complications, less bleeding, less analgesic use, and longer operative times. 16 We performed a prospective randomized study of SWL vs miniperc for patients who had solitary radiopaque (1–2 cm) lower caliceal renal stone.
In our study, the duration of surgery was 44.81 ± 7.065 minutes for SWL and 93.37 ± 12.29 minutes for miniperc, which showed statistically significant differences between them, which was similar to the reported literature results. 2,16,17 The longer operative time in miniperc was due to diminished intraoperative field visibility, also the need for stone disintegration into small particles suitable for ureteroscopic graspers or baskets and the small sheath. Regarding the hospital stay, it was significantly shorter in the SWL group in comparison with the miniperc group (5.72 ± 1.01 vs 45.19 ± 8.48 hours), respectively. Because of noninvasiveness of SWL, also in miniperc group, there are nephrostomy tubes and the need for follow-up after blood transfusion. Recent studies showed that tubeless PNL procedures decreased the hospital stay significantly. 18,19 SFR after three sessions of SWL for lower pole (LP) calculi is 38% to 84.6%. 2,20 –25 SWL also has a 13.9% to 53.9% retreatment rate 2,3,26 and a 7% to 33% AP rate. 2,3 In SWL arm in our study, the mean stone size was 1.55 ± 0.28 cm and we reported the 3-month SFR of 76%. In addition, the retreatment rate and the need for AP were 45.3% and 24%, respectively. SWL is a noninvasive procedure with less clearance rate. 27 Nowadays, miniperc technique is a less invasive alternative to PCNL, 16,28 which was improved due to better instrumentation, imaging, and an experienced surgeon. 29
In miniperc arm in this study, we noticed the mean stone size was 1.57 ± 0.26 cm and SFR was 96%. The retreatment rate and the need for AP were 2.7% and 4%, respectively. Although significantly higher SFR in the miniperc group in comparison with SWL (96% vs 76%), we observed in this study significantly higher rates of retreatment and APs (p = 0.001) for SWL than for miniperc. In prospective and retrospective studies reported by Preminger, 30 PCNL is more effective at clearing stones of 10 to 20 mm (72–92% clearance) compared with SWL (21–44% clearance). Many series with miniperc reported SFRs that were in the range of 60 to 90%. 28 In 2012, Sabnis and coworkers 31 reported that SFR reach 100%. In the present study, the lower SFR in SWL was because of failure of fragmentation in 9.3% and the presence of significant residuals in 14.6%. The widely cited lower pole stone articles 9,32 demonstrated a low success rate (35–37%) with lithotripsy. The study by Albala and colleagues 32 revealed that SFRs for PCNL were significantly better than SWL (95 vs 37%). Many factors affect success of SWL (obesity, calculus density, stone–skin distance [SSD], and chemical composition 33,34 or clearance [unfavorable LP anatomy]). 35,36 Furthermore, anatomical factors did not interfere with SFR after miniperc such as in SWL. Miniperc had advantage over SWL in using direct electrohydraulic disintegration, which can disintegrate all types of stones with different densities and chemical structures. 37 SFRs can be influenced by different definitions as well as radiographic methods used in different studies. Many authors who used PUT to determine SFR (while others used CT, which is more sensitive) had lower SFRs, which may have some reporting bias. 38 It is generally agreed that the decreased efficacy of SWL is due to retention of stone fragments rather than to disintegration of the stone. 39
For SWL and miniperc, complications such as postoperative fever, UTI, hematuria, Steinstrasse, and need for blood transfusion among others have been reported at various rates of as much as 30%. 22,40 –42 In our study, we observed a higher incidence of complications (bleeding requiring blood transfusion, fever >38°C managed by antibiotics, and symptomatic UTI using antibiotics) for miniperc than for SWL. This reveals the extra-aggressive nature of miniperc when compared with SWL. All complications were treated with either medical treatment. We reported a 4% transfusion rate and 5.3% fever >38°C (managed by antibiotic) rates for miniperc, which are higher than published literature. This was explained by multistep dilatation (not a single one using Amplatz dilators as much as 16F) using semirigid short ureteroscope (9–11F) as a miniperc device for stone retrieval and fragmentation by pneumatic lithotripsy, which leads to more tissue trauma, inflammation, and cortical scarring leading to these results. Complications with stone passage take place when stones were treated by SWL, as Steinstrasse occurred at 5.3%, which was comparable with others. 43 URS was needed in three patients with obstruction, while in the last one, the stones passed spontaneously.
The limitations of this study are the small number of patients included and a single-institute study. In addition to the deficient data obtained by noncontrast CT, it affects SFR after SWL in the form of calculus density, composition, and SSD. In addition, electrohydraulic SWL was used in this study. There are other types of SWL devices clinically available. Hence, the results of this study may be limited to this particular device. In our study, we can use both modalities to get the best stone clearance. SWL was used to manage significant residual stones after miniperc, making it smaller. In addition, miniperc was used in management of significant residual calculi that failed to be disintegrated after SWL. Nowadays, in North America and some European countries, there is a decline in lithotripsy use and a compensatory rise in using F-URS. This may depend on many factors as patient choice, access to lithotripsy, F
Conclusion
This randomized prospective study suggests that while SWL is less invasive than percutaneous stone removal, it is also less effective for lower pole radiopaque calculi.
Miniperc has better SFR and lower auxiliary and retreatment rates. However, it resulted in more drawbacks, including longer operative time, hospital stay, radiation exposure, and more blood transfusion.
Footnotes
Acknowledgment
The authors are grateful to the residents in the Urology Department, Benha University Hospital, Benha, Egypt, for help in patients' recruitment and follow-up.
Author Disclosure Statement
No competing financial interests exist.