
Abstract
Objectives:
To evaluate the impact of obesity on patients developing wound complications within 30 days of open and robotic radical prostatectomy using the National Surgical Quality Improvement Program (NSQIP).
Methods:
Patients undergoing radical prostatectomy in 2011 to 2012 were identified from NSQIP, which is a multi-institutional database of comprehensive 30-day postoperative outcomes. Wound complication included superficial surgical site infections (SSIs), deep SSI, organ space infections, and dehiscence. Descriptive statistics and multiple logistic regression examined the relationship between obesity and wound complications in open and robotic radical prostatectomy.
Results:
Of the 12,454 radical prostatectomy cases reported in the study period, 9248 were robotic (74%), 2244 (18%) patients were normal weight (body mass index [BMI] <25), 5836 (47%) were overweight (BMI 25–30), and 4374 (35%) were obese (BMI >30). Wound complications occurred in 134 (4%) of open and 114 (1%) of robotic radical prostatectomies. After adjusting for age, history of smoking, history of diabetes, history of chronic steroid use, and operative time, it was determined that obese patients were at 71% increased odds of developing a wound complication after open prostatectomy (p = 0.034), while there was no difference in the odds of a wound complication after robotic radical prostatectomy (odds ratio 1.14, p = 0.665).
Conclusions:
Obese patients are at increased risk of developing wound complications when undergoing open vs robotic radical prostatectomy. Obese patients likely benefit from robotic radical prostatectomy whenever feasible.
Introduction
P
We sought to evaluate whether the use of the robotic technique mitigates the risk of postoperative wound complications in obese patients undergoing radical prostatectomy using a multi-institutional database. Additionally, we evaluated modifiable risk factors, including operative time, which may have impacted development of wound complications in both the open and minimally invasive groups. We hypothesized that robotic assistance would decrease the risk of postoperative wound complications in obese patients receiving extirpative surgery for localized prostate cancer.
Methods
Patients and database
Institutional Review Board exempt status was obtained for the conduct of the study. The National Surgical Quality Improvement Program (NSQIP) prospectively captures 30-day postoperative outcomes on randomly selected surgical patients at participating institutions. 8 Trained surgical clinical reviewers systematically collect and submit data using patient records and phone call follow-up. The program is a validated American College of Surgeons (ACS) endeavor initially used in Veterans Affairs hospitals, but expanded to nonfederal hospitals in 2004, with the primary aim of collecting and improving surgical quality indicators. Institutional and national NSQIP data are available to participating NSQIP institutions. All adult patients undergoing radical prostatectomy between 2011 and 2012 were identified from the NSQIP database. Radical prostatectomy cases were identified by Current Procedure Terminology (CPT) codes (open: 55812, 55815, 55821, 55831, 55840, 55842, 55845; robot-assisted: 55866). The study was limited to patients undergoing prostatectomy for prostate cancer, which was identified by the International Classification of Disease Version 9 (ICD-9) code 185.
Outcomes and variables
The primary outcome of the study was the development of a wound complication. Wound complications were defined as superficial surgical site infections (SSIs), deep SSI, organ space infections, and wound dehiscence. The primary comparison was drawn between normal weight, overweight, and obese patients, which was defined by body mass index (BMI) of less than 25, 25 to 30, and greater than 30, respectively. Further comparison was drawn between open and robot-assisted radical prostatectomy techniques.
Variables evaluated in the study were demographic, perioperative, and postoperative. Demographic and hospital variables included age, race, and patient comorbidities. Perioperative variables included operative time and length of stay. Postoperative complications included wound complications, urinary tract infection (UTI), venous thromboembolism, septic shock, pneumonia, and reintubation. We initially intended to examine cardiac, renal, and neurologic complications, including myocardial infarction, cardiac arrest, acute renal failure, stroke, and delirium; however, these complications each occurred in less than 20 patients. Therefore, it was decided that they were too rare to be included in the analysis. Pathologic variables and estimated blood loss are not available from NSQIP. All variable definitions are available from NSQIP.
8
Clavien grading is not available in NSQIP; however, an attempt at application of Clavien grading was performed and the results are available as a Supplementary Table S1 (Supplementary Data are available online at
Statistical analyses
Descriptive analysis of the data was performed using Pearson's chi-squared test for categorical variables and Student's t-test and the Mann–Whitney test for continuous variables as appropriate. Multiple logistic regression was performed examining the impact of BMI on wound complications in open and robotic radical prostatectomy. Variables included in the model were chosen due to clinical relevance in wound healing: age, history of smoking, history of diabetes, recent steroid use, and operative time in 30-minute increments. We chose to perform logistic regression among robotic cases and open cases to compare the impact of obesity on wound complications in these cohorts of patients. A model that includes operative modality and all other variables is included as a Supplementary Table S2. From the multiple logistic regression models, an adjusted prediction model for probability of developing a wound infection based on operative time, procedure type, and BMI was generated. A priori p < 0.05 was chosen as the level of significance. All statistical analyses were performed using Stata version 12.1 (Statacorp, College Station, TX).
Results
In the study period, 12,454 prostatectomies were reported to NSQIP. Of these, 3206 (26%) were performed using an open technique, while 9248 (74%) were robotic. Seventy-eight percent of patients were overweight or obese. As shown in Table 1, there was no difference in smoking history, diabetes, and steroid use between the open and robotic patients. Two hundred forty-eight patients developed wound complications within 30 postoperative days. Of these, 40 were normal weight, 96 were overweight, and 112 were obese. Among open radical prostatectomy patients, 4% of normal weight (n = 24/616), 3% of overweight (n = 44/1542), and 6% of obese (n = 66/1048) patients developed wound complications (p < 0.001). In the robotic radical prostatectomy cohort, 1% of patients, regardless of BMI, developed wound complications (n = 16/1628 normal weight, n = 52/4294 overweight, n = 46/3326 obese; p = 0.480). Urinary tract infections were more common among the open cohort (n = 114/3206 open, n = 138/9248 robotic, p < 0.001). Fifty-two (1.6%) of the open patients required reoperation compared with 112 (1.2%) of robotic patients (p = 0.079) in the 30 days of postradical prostatectomy.
In the setting of less than 10 patients in a group, Fisher's exact test was performed.
BMI = body mass index; DVT = deep vein thrombosis; IQR = interquartile range; LOS = length of stay; PE = pulmonary embolus; SSI = surgical site infection; VTE = venous thromboembolism.
On multiple logistic regression examining the impact of BMI on wound complications among open radical prostatectomy patients (Table 2), obese patients were at 1.71 times increased odds of a wound complication compared with normal weight patients (p = 0.034). Additionally, open radical prostatectomy patients with a history of smoking had nearly twice the odds of developing a wound complication, and each 30-minute increase in operative time was associated with a 16% increase in the odds of an SSI. When performing the multiple logistic regression examining the impact of BMI on wound complications among robotic radical prostatectomy patients, only a history of steroids and increasing operative time demonstrated a positive association. As shown in Figure 1, with increasing operative time, there is an increased risk of developing wound infections. This was most pronounced among patients undergoing open radical prostatectomy regardless of BMI. The impact of BMI was significantly less in the robot-assisted prostatectomy patients. Supplementary Figure S1 shows that with increasing BMI, the risk of SSI is more pronounced among open compared with robot-assisted procedures.
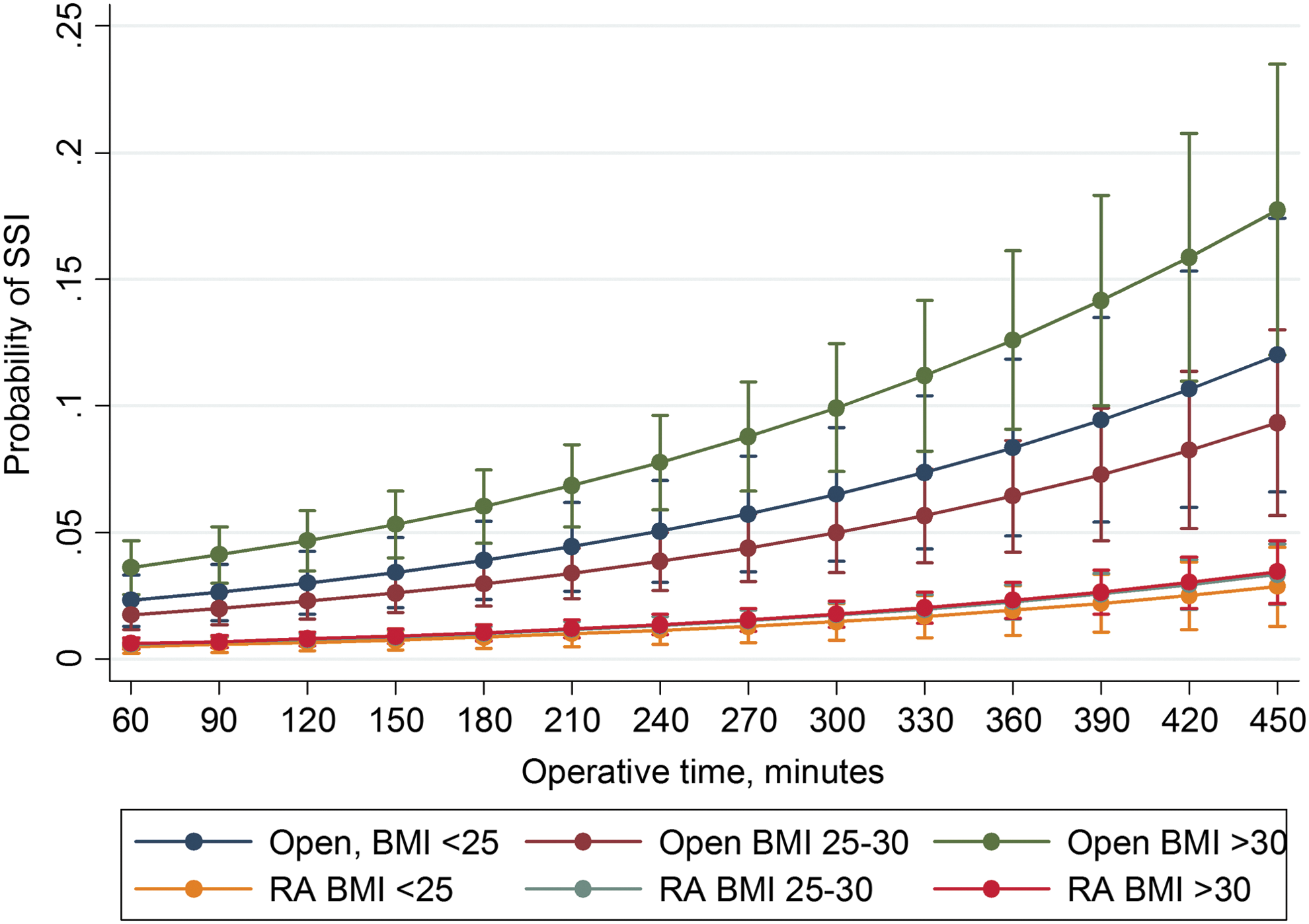
Probability of developing an SSI as a function of operative time, comparing technique, and BMI. Model controls for age, smoking, diabetes, and steroid use. Patients undergoing open radical prostatectomy are at increased risk of developing SSIs. This risk increases based on BMI category. BMI = body mass index; RA = robot-assisted; SSI = surgical site infection.
Discussion
The economic impact of wound complications in an era of pay-for-performance penalizations is a significant consideration when planning an operation. Additionally, obesity itself has well-established impacts on healthcare costs, and surgery for obese patients can pose additional hazards not otherwise considered. 7,9 Recent recommendations from the U.S. Preventative Task Force (USPTF) regarding prostate specific antigen screening are already impacting both diagnosis and treatment of prostate cancer across all ages and demographics. 10 As the pendulum continues to swing toward more selective treatment regimens for men with localized prostate cancer, understanding the impact of surgical technique and other modifiers on wound complications, especially in higher risk men, is critical.
Postoperative wound complications result in significant costs to the healthcare system. In colorectal surgery patients, Wick and colleagues previously reported that patients with an SSI incurred a $17,000 increase in charges to primary payers. 11 Although radical prostatectomy patients have lower SSI rates compared with patients undergoing bowel operations, the economic impact of an SSI in the prostatectomy population remains substantial. Pay-for-performance programs have threatened decreased reimbursement for cases with complications, including postoperative wound infections. 11,12 Beyond the immediate impact of a wound complication, there is likely a larger societal impact associated with delayed return to productivity. 13 Fixed variables, including obesity and other comorbidities, are often nonmodifiable by the surgeon. Identifying techniques to mitigate the increased risk imposed by obesity is critical for surgeons, particularly in light of pay-for-performance programs.
Multiple studies have evaluated the impact of obesity on radical prostatectomy outcomes. Van Roermund and colleagues evaluated a cohort of 252 men undergoing open retropubic radical prostatectomy and reported that 16% of obese patients developed wound complications compared with 4% of nonobese patients. 5 In the current study, we reported that 6% of obese patients undergoing open radical prostatectomy developed wound complications, which was significantly higher than the incidence of wound complications among nonobese patients. Similarly, Bae and colleagues reported that in open prostatectomy, obese patients were subjected to higher complication rates and increased blood loss compared with nonobese patients. Similar associations were not demonstrated in robot-assisted prostatectomy. 4 Although we were unable to examine blood loss, we did find that there was no difference in wound complications based on BMI among patients undergoing robot-assisted radical prostatectomy. This finding has been validated across multiple single-institution studies examining only robot-assisted or laparoscopic prostatectomy cohorts and reporting no difference in wound complications based on obesity alone. 14 –16 The impact of obesity on surgical wound healing is likely multifaceted. Studies have suggested that poor nutritional status, lack of mobility, immune impairment, and increased tension on suture lines impact wound healing among overweight and obese patients. 9,17,18 Minimally invasive techniques facilitate earlier ambulation and yield smaller incisions, both of which likely contribute to improved wound healing in obese patients.
In addition to the well-established advantages of minimally invasive surgery, including decreased blood loss, reduced narcotic use, and improved convalescence, 19 robotic surgery may have its highest potential benefit in the management of the obese patient. A recent study additionally noted that robotic compared with open radical prostatectomy was associated with decreased risk of readmission. 20 Despite the aforementioned advantages of robotic surgery for this higher risk cohort, it should be mentioned that unique technical challenges—including port placement modification, increased role of the bedside assistant to maintain surgical exposure, and working in a limited space with or without minimized pneumoperitoneum (for ventilation purposes)—may often be encountered. 21 Additionally, anesthesia-related challenges secondary to increased intraoperative airway pressures as well as longer procedure times also exist. 22 While many of these nuances can be overcome by surgeon experience and comfort levels of the entire operating room team, robot-assisted prostatectomy in the obese male is a more difficult operation compared with the identical operation in a nonobese patient and careful risk/benefit consideration should be made.
The potential benefit of robotic surgery in the obese patient population has been explored in other urologic procedures. Isac and colleagues reported on 250 patients undergoing partial nephrectomy and reported that there was no difference in postoperative complications among obese and nonobese patients. 23 Similar findings have been reported in partial nephrectomy and radical nephrectomy cohorts. 24 –26 However, in line with the findings of the current study, Musch et al. and Sung et al. reported decreased postoperative complications following robot-assisted radical cystectomy. 27 Identifying factors that mitigate postoperative risks in high-risk populations aids in determining which procedures should be considered the standard of care. Robotic assistance should be used preferentially in obese men undergoing radical prostatectomy to reduce the risk of postoperative complications.
We report that patients with use of chronic steroids were at four times increased risk of SSIs in the robotic cohort. This was an unexpected finding as the authors expected that chronic steroid use would impact wound healing in the open cohort more than the robot-assisted patients. We hypothesize that this may be related to the closure of the primary extraction site, where the small incision can actually challenge appropriate visualization of fascial edges. This may be additionally difficult in the obese patient and less forgiving in a patient on chronic steroids. It would be interesting to further investigate the impact of chronic steroid use on long-term hernia formation in the open and robotic radical prostatectomy cohorts.
Operative time has previously been shown to negatively impact postoperative length of stay and wound complication rates. 28 –30 Procter and colleagues examined the impact of operative time on general surgical procedures and reported that the risk of postoperative complications, defined as wound infections, UTIs, sepsis, or pneumonia, increased significantly for each additional 30 minutes of operative time. 28 Similarly, Monn et al. reported that operative time and surgical approach, independent of in-hospital complications, were associated with significantly longer hospital stays among patients undergoing urologic procedures with both open and minimally invasive techniques. 30 In the current study, we report that operative time was a significant independent predictor of postoperative wound complications among both open and robot-assisted radical prostatectomy cases. Furthermore, as shown in Figure 1, we demonstrated that the impact of operative time on wound infections in overweight and obese patients compared with normal weight patients was mitigated by utilizing the robot-assisted approach.
There are several limitations of this study. Foremost, we were unable to evaluate pathology using the NSQIP database. Therefore, surgical challenges associated with higher grade and/or more advanced disease could not be identified. Additionally, data regarding blood loss and long-term complications are not available. We intended to include cardiac, renal, and neurologic complications in the study; however, given the rarity following radical prostatectomy, these were unable to be included. Finally, additional factors—such as surgeon experience, patient selection for either open or robotic surgery, and preoperative antibiotics—cannot be characterized using the NSQIP database and may have impacted outcomes. As NSQIP is provided as a paid service to hospitals, there is a chance that large, tertiary care centers represent a disproportionate number of cases in the database, which may create a selection bias in the cases included. Additionally, the current study is retrospective in nature, and true rates of wound complications may be higher than what was captured by NSQIP. Regardless of these limitations, the study represents the largest current analysis evaluating wound infection and radical prostatectomy and the direct impact of surgical technique.
Conclusions
Surgical management of obese men with localized prostate cancer is challenging. Utilizing robot-assisted techniques whenever feasible appears to mitigate the impact of obesity on wound complications following radical prostatectomy, independent of patient's history of smoking, diabetes, and steroid use. Surgical efficiency, while important for both open and minimally invasive approaches, has a larger impact on minimizing wound complications in the open cohort. Particularly in the setting of increased pay-for-performance programs, identifying techniques that decrease complication risk among patients with unmodifiable comorbidities is becoming of the utmost importance. Careful consideration of all options in obese men with prostate cancer, including the surgical approach, timing of surgery (weight loss with delayed treatment), or consideration of nonsurgical management, is warranted and requires further research evaluation to determine the ideal management strategy for these men.
Footnotes
Acknowledgments
The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.