
Abstract
Objective:
To investigate the impact of three-dimensional (3D) printed pelvicaliceal system models on residents' understanding of pelvicaliceal system anatomy before percutaneous nephrolithotripsy (PCNL).
Materials and Methods:
Patients with unilateral complex renal stones indicating PCNL were selected. Usable data of patients were obtained from CT-scans in Digital Imaging and Communications in Medicine (DICOM) format. Mimics software version 16.0 (Materialise, Belgium) was used for segmentation and extraction of pelvicaliceal systems (PCSs). All DICOM-formatted files were converted to the stereolithography file format. Finally, fused deposition modeling was used to create plasticine 3D models of PCSs. A questionnaire was designed so that residents could assess the 3D models' effects on their understanding of the anatomy of the pelvicaliceal system before PCNL (Fig. 3).
Results:
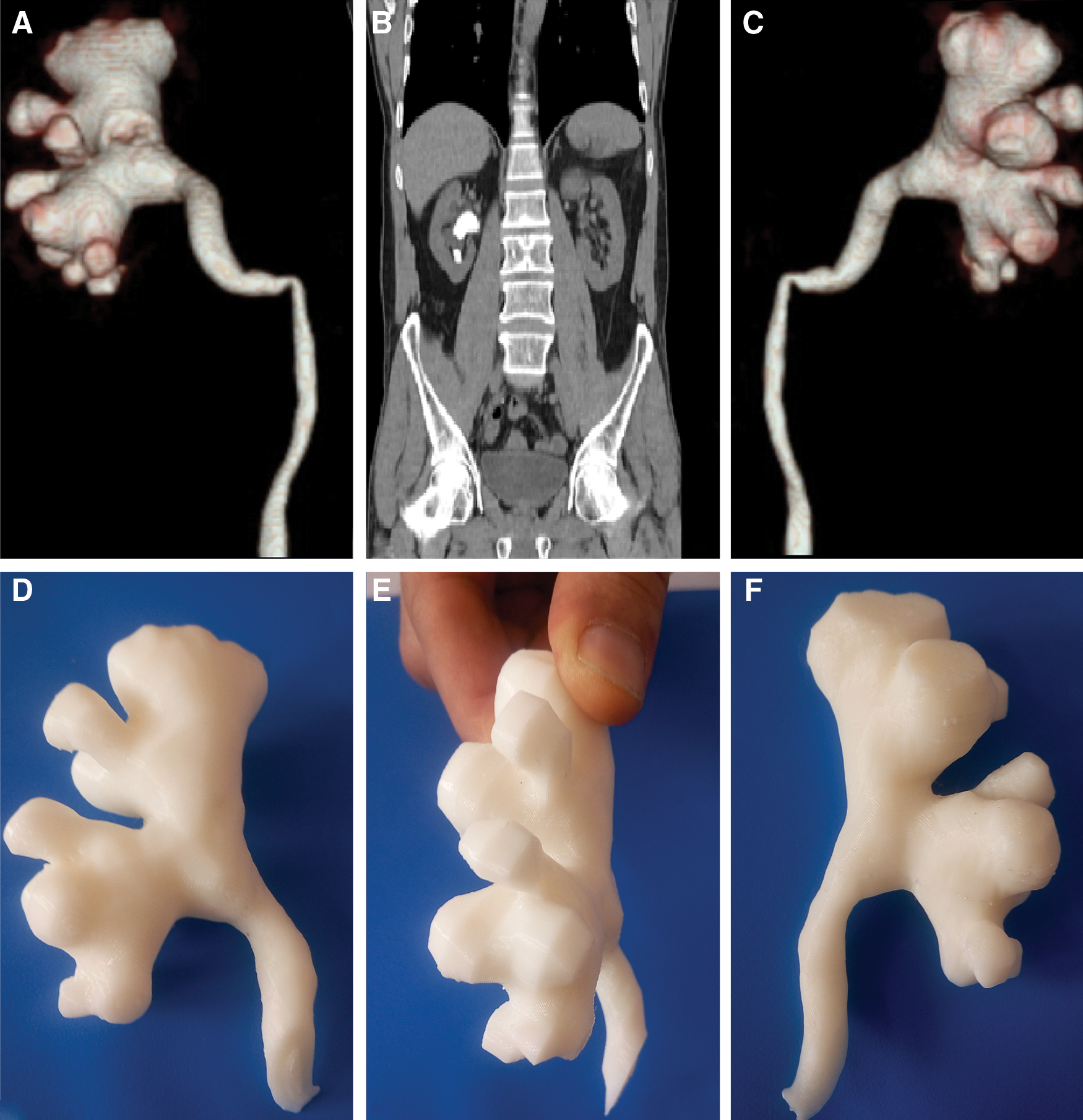
Five patients' anatomically accurate models of the human renal collecting system were effectively generated (Figs. 1 and 2). After presentation of the 3D models, residents were 86% and 88% better at determining the number of anterior and posterior calices, respectively, 60% better at understanding stone location, and 64% better at determining optimal entry calix into the collecting system (Fig. 5).
Conclusion:
Generating kidney models of PCSs using 3D printing technology is feasible, and the models were accepted by residents as aids in surgical planning and understanding of pelvicaliceal system anatomy before PCNL.
Introduction
T
Percutaneous nephrolithotripsy (PCNL) is a standard, safe, and efficient method for treating renal stones larger than 2 cm. 4 Access through an appropriate calix and knowledge of the complex 3D internal anatomy are essential for an effective PCNL. Adequate preoperative planning is mandatory, especially in learning the PCNL procedure. Computed tomography (CT) with or without contrast enhancement is the first choice for renal stone surgery. 5 With advances in CT technology (e.g., rapid spiral acquisition and reconstruction software), it is now possible to provide accurately reconstructed 3D images of the pelvicaliceal system (PCS) 6 that can be used to facilitate effective PCNLs. 7,8 Turney effectively constructed an accurate human renal collecting system using 3D printing technology and utilized their model as an educational tool for residents and patients undergoing PCNL. 9 The ability to generate 3D models from patient data is allowing physicians to create custom prosthetics and implants, to better view complicated pathologies, and to teach trainees in ways never seen before. 10
In this study, our aim was to assess whether 3D printed models of PCSs can improve resident understanding of the PCS anatomy before PCNLs.
Materials and Methods
Creating 3D printed models from medical imaging
Creating 3D models from medical imaging data is a multistep process. First, usable data must be obtained from CT scans, magnetic resonance images, or ultrasound images. In our hospital (Okmeydani Teaching and Research Hospital), we used CT (Toshiba Alexion™ multislice CT) scan data from five patients.
Second, segmentation or extraction and isolation of data from the area of interest must be performed. We sent our Digital Imaging and Communications in Medicine (DICOM)-formatted data to a bioengineer (Biotechnica Engineering Co. Ltd., Istanbul) for segmentation. Numerous software programs are available for use with DICOM datasets. In our case, Mimics software version 16.0 (Materialise, Belgium) was used.
Finally, data must be saved in a file format recognized by the 3D printed software. The most commonly used format is the stereolithography (.stl) file format.
3D printing
Recent advances in 3D printing technology have produced new processes that allow the use of a variety of materials' factors. Acrylonitrile butadiene styrene (ABS) has been used for creating 3D models of PCSs. The most important mechanical properties of ABS are impact resistance, toughness, high radiodensity, and low cost. We used fused deposition modeling, an inexpensive technology popular with consumers. These printers use a polymer filament that is heated to a liquid state in a printer head and deposited in predefined locations corresponding to the model shape (Stratasys, Inc.) 11
From June 2015 to January 2016, five patients with unilateral staghorn renal stones and clinical indications for PCNL were selected. Our first aim was to effectively create 3D models of the PCSs. After two attempts, we effectively generated anatomically accurate models of the human renal collecting system that were of the correct size and shape using fused deposition modeling. Overall, collecting systems were clear virtual reconstructions (Figs. 1 and 2). The cost of consumables to produce these models was around $100 for each model, primarily the rental cost of the 3D printer. Print time was approximately 2 hours each.

Patient 1
Patient 2
Evolution of models from residents
To assess the educational utility of our models, a questionnaire was designed for residents (Fig. 3). Ten residents evaluated the 5 patients using traditional CT-scans and intravenous urography images. Each then completed the questionnaire to prospectively assess their ability to estimate the number of posterior and anterior calices and to demonstrate their understanding of stone locations. In addition, their assessments of the optimal entry calix into the collecting system were determined. For each correct answer, five points were given, but for each incorrect answer and for overestimating the number of calices, one point was deducted. In addition, five points were given for correct selections of the optimal entry calices, which were selected by an experienced urologist who had performed more than 100 PCNLs. No points were given if other options were chosen. The 3D models were then presented to the residents, and they completed the questionnaire again for each of the five patients. Results of the two questionnaires were compared.
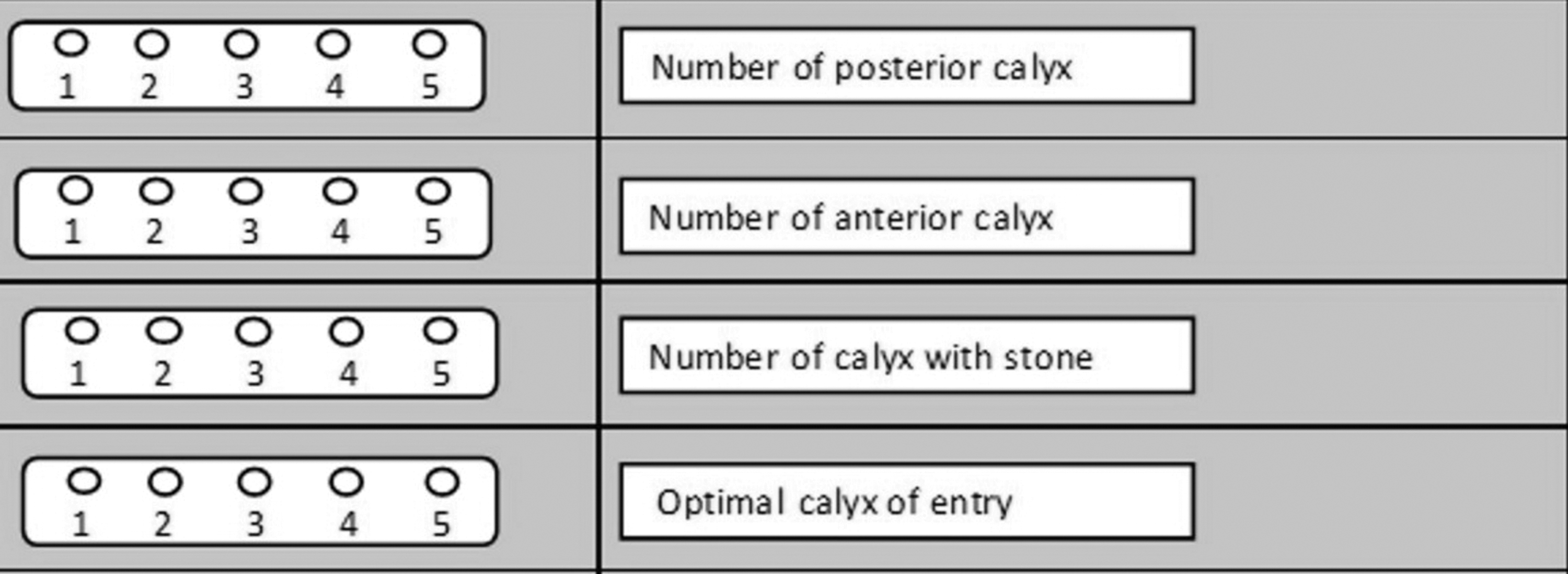
Resident questionnaire.
Statistics
In each iteration, a total of 40 questions were presented to residents. Median total scores were calculated for each section, and questionnaires completed before and after 3D printed model presentation were compared using the Wilcoxon signed rank test. Statistical analyses were performed using SPSS Statistics version 21.0 (IBM Corporation, Armonk, NY).
Results
Results of the resident questionnaires are shown in Figure 4, revealing that the models could be more useful than conventional imaging for surgical planning. Average overall scores for questions Q1, Q2, Q3, and Q4 were 120, 60, 130, and 90, respectively, of 200 possible points each. After examining the models, these scores were increased to 250, 250, 200, and 250, respectively. Residents tended to be more familiar with the positions of the PCSs and stones. After using the renal models, all residents reported that a 3D printed model could be a useful tool in planning PCNLs. Total percentage scores for residents before and after presentation of 3D models are shown in Figure 5. After model presentation, determining the number of anterior and posterior calices improved 52% (p = 0.018) and 76% (p = 0.009), respectively, understanding stone location improved 28% (p = 0.035), and the ability to determine the optimal entry calix into the collecting system improved 64% (p = 0.020). All residents agreed that the models could benefit surgical planning and supported their use as potential training aids in demanding procedures when combined with two-dimensional (2D) data.

Total scores for residents before and after presentation of 3D models. Q1: Number of posterior calix. Q2: Number of anterior calix. Q3: Number of calix with stones. Q4: Ability to select optimal calix of entry.

Total percentage score for residents before and after presentation of 3D models. Scores for Q1, Q2, Q3, and Q4 improved 52%, 76%, 28%, and 64%, respectively.
Discussion
Surgeons have shifted to a preference for minimal invasiveness. Use of 2D images limits surgeons' abilities to view intraoperative scenarios. 12 Therefore, 3D imaging modalities have been developed for various surgical fields. 13,14 In urology, PCNL is an effective treatment, but various factors have negative impacts on success rates and complications of PCNLs. Several studies have revealed that as stone burdens and numbers of tracks increase, stone-free rates decrease and bleeding increases. 15,16 Staghorn stones require multiple tracks to achieve stone-free status. The ultimate goal is complete stone clearance with no complications, ideally after a single procedure with a single access track.
In this study, we created five physical, patient-specific, and anatomically correct models based on CT-scan data of the human renal collecting system before operative intervention for unilateral staghorn renal stones. These models of the PCSs can provide not only necessary images but also the ability to plan collecting system access for PCNL surgery in complex staghorn renal stone treatment. Posterior and anterior calices are well described in the printed models, and their orientation to the renal pelvis can be observed when planning access.
Models have been used for preoperative planning of complex orthopedic and craniofacial procedures and of neurosurgical treatments. 17,18 Few reports of biomodeling for planning endourologic procedures are found in the literature. 19,20 While creating a 3D model, the most important steps for the urologist are to collaborate with a radiologist and a bioengineer. Slice thickness in CT-scans must be 5 to 3 mm because low-resolution images can result in discrepancies between the generated model and the patient's actual anatomy. 21 The greater dose of radiation delivered to the patient when generating CT-scans thinner than 5 mm is a cause for concern. The dose could increase 75% relative to that delivered with low-dose CT. 22,23 Segmentation and mesh generation are key steps in 3D modeling, necessitating collaboration with a bioengineer informed about kidney anatomy before segmentation. We experienced problems with the DICOM data and segmentation in our first try (Fig. 6).

Segmentation problem in our first try.
Generating 3D models anatomically identical to the patient's renal collecting system allows surgeons, trainees, and patients to interact with the renal unit in a tangible way rather than using conventional imagery. In this study, we have shown that interaction with models is an effective learning experience for trainees, resulting in improvements over interactions with conventional imaging. Using 3D models, residents were better able to understand the renal anatomy and determine the access calix and the number of calices than when using only CT-scans and intravenous urography images. In addition, resident self-confidence during surgery was boosted. In particular, the value of using 3D models as educational tools is greater for trainees with less experience and knowledge of interpreting cross-sectional images.
Several models for PCNL training have been developed over the years. 24,25 The main advantage of the model described in this study is that it is clean and relatively low in cost. The anatomic accuracy seen on fluoroscopy makes it particularly useful for practicing triangulation techniques. Anatomically accurate models such as those described in this study may be cheaper and more representative alternatives when developing new technologies to facilitate caliceal targeting. This anatomically accurate model can be adapted and developed for training in flexible ureteroscopy and surgical planning for nerve-sparing radical prostatectomy.
Conclusion
Generating kidney models of PCSs using 3D printing technology is feasible, and the models were accepted by residents as aids in surgical planning and understanding of pelvicaliceal system anatomy before PCNL.
Footnotes
Author Disclosure Statement
No competing financial interests exist.