
Abstract
Background:
Percutaneous needle access is a critical step of performing percutaneous nephrolithotomy. Development of a synthetic model that accurately represents the forces encountered while gaining percutaneous renal access, allows for high ease of use and prevention of negative skill transfer. The objectives of this study were to define the needle insertion forces used during percutaneous renal access and to develop a multilayer synthetic physical simulator model based on human tissue data that is compatible with the SimPORTAL fluoro-less C-arm trainer (CAT) camera system.
Materials and Methods:
Needle insertion data were collected using in situ fresh human cadaveric tissue within 72 hours of death. Ultrasound guidance was used to place percutaneous reference needles into the kidney, and axial force vs displacement data was collected using a custom-built force measurement device. A novel multilayer model that includes several types of synthetic materials for simulation of distinct tissue layers was developed based on the human tissue reference data. The multilayer prototype model and an existing single material model were subsequently tested using the same needle insertion protocol and the results were compared with human tissue data.
Results:
Average maximum forces for needle puncture into skin ranged from 2.75 to 2.80 N for human tissue and from 4.53 to 4.19 N for simulated human tissue. The overall slope for all force vs displacement data was 0.35 to 0.59 N/cm for human tissue. The overall slope was comparatively lower for the multilayer model (0.17 N/cm) and was highest in the existing single material model (5.08–9.79 N/cm).
Conclusions:
We have defined the forces for percutaneous renal access using fresh human cadaveric tissue and designed a multilayer synthetic simulator model that can be utilized for training percutaneous needle access to the renal collecting system using the CAT camera system.
Introduction
P
The skill necessary to obtain needle access to the collecting system is well suited for the simulation environment. As the minimally invasive approach of the PCNL procedure evolved in the 1980s, a porcine model was created for training and hands-on courses. This effectively demonstrated the importance of simulation at the time the procedure was first gaining acceptance among endourologists. 5 Since that time, many simulators have been designed for training percutaneous renal access. Animal models using chicken and/or porcine tissue and virtual reality simulators have been reported in the literature. 6 –9 The University of Minnesota SimPORTAL C-arm trainer (CAT) was designed for training the concept of parallax for obtaining access during PCNL. 10,11 The camera system used for this device allows for a simulated X-ray visualization without the need for fluoroscopy, eliminating any radiation exposure while training. Synthetic model materials used in this system need to be transparent to allow for visualization of the renal pelvis and calices that are filled with dye during the simulation. Preliminary models used for the CAT were produced using a single semisolid silicone material, which was not benchmarked against the multiple layers of the human flank.
To increase model fidelity, increase ease of use, and decrease the likelihood of negative skill transfer, accurate representation of needle insertion forces encountered when interacting with human tissue is preferred. In addition to assistance from intraoperative imaging, percutaneous procedures require recognition of force feedback when tissue planes are cut. As the needle passes through distinct layers with significantly different tissue properties, such as a tissue plane, organ border, or other structure (e.g., blood vessel, kidney calices), there is a rapid rise and subsequent drop in force, which can be described as a major puncture event. Before puncture of a plane, the tissue is deforming at the same rate as the needle tip, with tissue cutting absent until the force decreases. 12 Accurate representation of these forces in a simulator model is valuable for instructors when training these skills and for learners to develop motor skills that are applicable within a clinical context.
Needle insertion into soft tissue and synthetic materials has been extensively studied in the fields of engineering and medicine, and many investigations of needle–tissue interaction experiments, modeling, simulators, and needle insertion assist devices have been reviewed by others. 13 Previous investigations of needle insertion forces include insertion through layers of skin, fat, and muscle, 14 puncture of an ex vivo porcine kidney encased in agar gel submerged in water, 15 and in vivo 16 or ex vivo 17,18 direct insertion into the kidney.
The first objective of this study was to characterize needle insertion forces during percutaneous renal access using fresh in situ human cadaveric tissue. The second objective was to develop a physical simulator model based on the reference data that more accurately replicates needle insertion forces and is compatible with the SimPORTAL CAT camera system.
Materials and Methods
Force measurement device
A portable device for measurement of needle insertion forces was built using a 12-inch 0.025 inch/rev translational stage with stepper motor (XSlide; Velmex, Inc., Bloomfield, NY) that was mounted on a vertical 15-inch manually adjustable translational stage (BiSlide; Velmex, Inc.) using a 3D printed 360° manually rotatable lockable mounting plate. The vertical stage was attached to a 360° manually rotatable lockable base plate. The rotatable mounting and base plate connector pieces allowed for adjustment of needle trajectory, positioning of insertion point, and angle of insertion. The needle was attached to the 12-inch translational stage and load cell using a custom 3D printed needle holder. A graphical user interface was developed in MATLAB (MathWorks, Natick, MA) to control the needle displacement path by the user. Force data were acquired using a 10-kg load cell and LoadVUE software (iLoad Mini; Loadstar Sensors, Fremont, CA). The entire device was able to be transported to the site of data collection and be positioned at the appropriate height and angle.
Needle insertion data on human cadaveric tissue
Two fresh cadaveric donors (donors 1 and 2) were obtained through the University of Minnesota Anatomy Bequest Program. Negative serology (hepatitis B/C, HIV) was confirmed before data collection. Data were collected within 72 hours of death.
Donors were placed in the supine position, and water was injected in a retrograde manner through a Foley catheter and stents to distend the renal collecting system. Donors were then moved into the prone position, and two reference needles were placed percutaneously into the renal collecting system bilaterally using ultrasound guidance (Fig. 1a).

Once the reference needles were placed, the force measurement device was brought alongside the donor (Fig. 1b). The placement of the reference needles was used to determine the position, angle, and depth of the test needles that were subsequently inserted using the force measurement device (Fig. 1c). An 18-gauge, 20-cm, 2-piece percutaneous access needle (Boston Scientific, Marlborough, MA) with triangular pyramid tip was inserted at a constant rate of 0.16 cm/second for donor 1 and 0.48 cm/second for donor 2. These rates were selected based on those previously presented in the literature 15 and observation of rates seen clinically, although these are variable. No skin incision was made before needle insertion. The needles passed through all tissue layers from the skin to renal pelvis to obtain axial (along insertion axis) force vs displacement data. There were 24 total trials completed (5 right and 5 left for donor 1, 7 right and 7 left for donor 2). Following each trial, either the needle or wire remained in place to mark the needle insertion path to prevent overlap with subsequent needle insertions.
Synthetic physical simulator model development
The three synthetic materials chosen for use in the simulator model were translucent room temperature vulcanizing (RTV) silicone, a low durometer opaque silicone, and polyacrylamide hydrogel cubes. The polyacrylamide cubes are commercially available as small cubes that expand in water to become transparent blocks when fully saturated. The materials were cast to create a model with four major layers. The innermost layer was a translucent silicone “kidney” (Fig. 2a) cast on a 3D printed patient-specific anatomically accurate mold created from MRI/CT data (Fig. 2b). The simulated kidney layer was surrounded by water-saturated polyacrylamide cubes. These represented the connective tissue, muscle, and adipose layers collectively. A translucent silicone shell surrounded the two inner layers and represented the contour of the right flank (Fig. 2c). An additional opaque low durometer silicone layer was added to the outer surface of the model as the final layer. The transparent nature of the hydrogel blocks and RTV silicone with the outer opaque silicone layer allowed for compatibility with the preexisting fluoro-less CAT camera system. The fully assembled prototype model is shown in Figure 3a.


Next, the prototype was subjectively evaluated for compatibility with the current SimPORTAL fluoro-less CAT. Rib and skin overlays were added, and the model was placed on the mini C-arm. Visualization of the calices was achieved using the existing CAT camera system following injection of dye into the collecting system using a Foley catheter inserted into the simulated ureter.
Needle insertion data on synthetic materials
The needle insertion force data collection protocol using the force measurement device was repeated on the multilayer prototype model (Fig. 3b) and the existing single-material SimPORTAL training model. The existing version of the model comprised a single type of semisolid translucent RTV silicone. The needle was inserted through all simulated tissue layers and axial force vs displacement data was collected.
Results
Needle insertion forces
Figure 4 demonstrates needle insertion force as a function of displacement for human cadaveric tissue, the multilayer prototype model, and the single-material model at a needle insertion rate of 0.16 cm/second (Fig. 4a) and 0.48 cm/second (Fig. 4b).
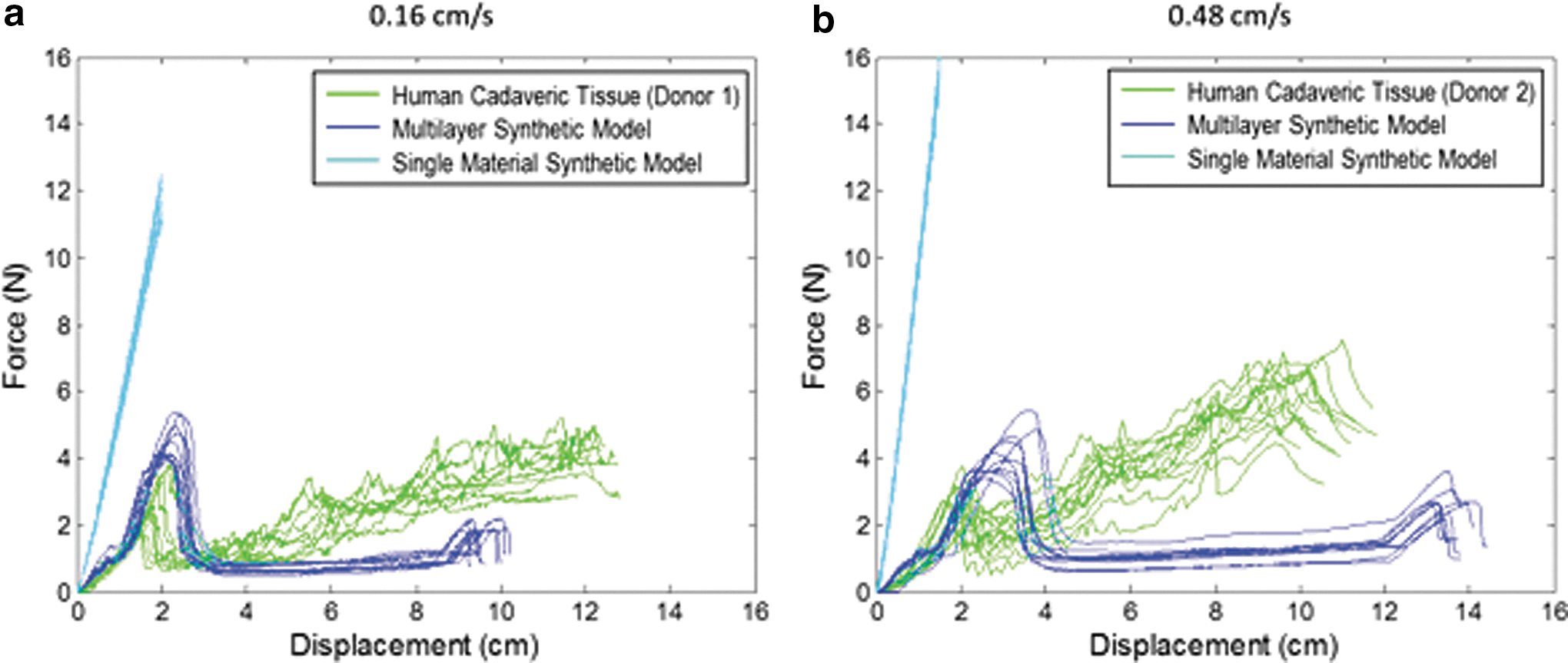
Comparison of needle insertion force vs needle tip displacement at
The cadaveric and multilayer model data were analyzed for maximum force required for skin (or simulated skin) puncture, as depicted by point A for a single-example trial at 0.16 cm/second in Figure 5. The average maximum force was larger in the multilayer model compared with human tissue (p < 0.001). All force data are shown in Table 1.

Single-needle insertion trial for
Coefficients a 1 and a 2 for the second-degree polynomial as shown in Equation (1). p-Values compare each model type (multilayer or single material) to cadaveric human tissue.
SD = standard deviation.
The magnitude of force decrease after skin (or simulated skin) puncture (segment B) and the magnitude of force increase before puncture of simulated kidney (segment C) are labeled in Figure 5, and average values are shown in Table 1. The average magnitude of segment B was larger in the multilayer model compared with human tissue (p < 0.001).
Linear regression was also completed for the human cadaveric tissue, multilayer model, and single-material model. The average slope for regression over all data is shown in Table 1 and labeled as line D for a single trial for human tissue and multilayer model in Figure 5. The average slope for the single-material model was larger compared with human tissue (p < 0.001), and the average slope for the multilayer model was smaller compared with human tissue (p < 0.001).
To characterize the deformation of tissue and synthetic material before skin (or simulated skin) puncture, a second-degree polynomial [Eq. (1)] was used assuming
In comparing coefficients between human and simulated skin tissue, there was a statistically significant difference for a1 and a2 (p < 0.001), except for a1 at 0.16 cm/second (p = 0.08).
Compatibility of prototype model with CAT
Overall, the prototype model was compatible with the existing CAT platform. Addition of dye through Foley catheter allowed for simulation of contrast under fluoroscopy to be visualized on the monitor (Fig. 6). Flow of dye into the renal pelvis and calices simulated the image that would be seen while using fluoroscopic techniques.
Visualization of filling of the collecting system seen on a monitor using the CAT camera system. CAT, C-arm trainer.
Discussion
The development of training models that accurately simulate properties of human tissue is important for facilitating skill transfer and increasing ease of use. Human tissue property data provide benchmark values for reference during the simulator design process and allow for defining gold standards, on which model fidelity can be partially based. This study demonstrates the effective application of human tissue properties as reference data for the development of an improved multilayer synthetic simulator model. The prototype developed allows for training of the needle insertion step of PCNL and is compatible with the existing CAT system.
The constant velocity and straight needle path used during data acquisition do not fully characterize the needle movements seen clinically during PCNL, including velocity changes and steering. However, the use of the force measurement device, compared with a device placed in the surgeon's hand to measure needle force, is advantageous for this application as constant velocity and displacement allows for tissue and model comparison as well as repeatability between trials. The same needle type was used throughout, and therefore, these data do not necessarily apply to other needle types of differing length, diameter, or tip type.
The experiments were performed on tissues in situ without alteration of surrounding tissue. This allowed for tissue planes to remain intact without alteration of natural tissue relationships and tension. The fresh cadaveric tissue used for this study has the disadvantage of not being perfused at the time of testing and may have undergone degradation at that point.
Reference needles were used to determine test needle trajectory and depth. Therefore, apart from skin perforation, there is no definitive evidence for which tissue layers correspond to which major puncture events as no imaging was used during data collection. For this data set, we chose to fit a simple linear regression line to characterize the trend in force accumulation for the internal tissue layers.
The new prototype model has multiple layers allowing for more accurate simulation of force variations seen in human tissue data. These variations in force were achieved as the needle moved between the silicone and polyacrylamide cube layers. This allows for learners to be trained to recognize forces felt when the needle passes through tissue layers that are clinically relevant to the PCNL procedure. This is an improvement on the existing version of the single-material synthetic model, which was shown to have higher forces than those seen in the human tissue reference data. This has the potential to lead to negative skill transfer due to excessive force used to insert needles to a clinically relevant depth.
Although improvements have been made, there remains a statistically significant difference in force measurements between the prototype model and human tissue. The needle insertion data show that the cadaveric tissue has higher variability in forces for internal puncture events when moving through the adipose, muscle, and connective tissue compared with the needle moving through the simulated bulk structures (polyacrylamide blocks). In addition, the accumulation of force per displacement is higher in the cadaveric tissue compared with the polyacrylamide blocks.
An advantage of using the polyacrylamide cubes is that the needle tracks from previous insertions cannot be seen, which increases the number of iterations that the model can be used, adding to cost-effectiveness and ease of use. The low durometer outer layer on the prototype model was able to reseal following needle insertion and removal, preventing water leakage and increasing the longevity of the model.
Overall, future directions should address several limitations of the current prototype and study design. First, additional adjustments in material formulations should be made to better approximate the overall slope of the human tissue data as shown in line D. Second, the amount of tissue degradation in the fresh cadaveric tissue is unknown compared with perfused tissues, and therefore, in vivo testing may be useful to address this.
Despite these limitations, this research demonstrates using objective data to define the fidelity of a simulator model. This provides a standard against which subsequent prototype models can be compared. The overall approach demonstrated in this study can be used to validate or contradict claims of model realism and ability to represent tissue properties in addition to traditional validity studies.
Conclusions
Accurately representing human tissue properties in simulators used to train surgical skills is a challenging process. We have effectively measured the forces applied to the needle during percutaneous needle insertion into the kidney using fresh human cadaveric flanks and have designed a multilayer synthetic simulator model that can be utilized for training percutaneous needle access to the kidney collecting system. In addition, the model is compatible with the existing SimPORTAL fluoro-less CAT, which is already being used in AUA sanctioned training courses. This study provides an example of using objective human tissue properties as a reference during the simulator design process to provide evidence for model fidelity.
Footnotes
Acknowledgments
The authors thank Gretchen Floan, Jason Speich, and Troy Reihsen for their contributions.
Author Disclosure Statement
No competing financial interests exist.