
Abstract
Background:
Robot-assisted partial nephrectomy (RAPN) is increasingly being used for the surgical management of renal masses. The comparison of RAPN with open partial nephrectomy (OPN) has not yet led to a unified conclusion with regard to perioperative outcomes.
Purpose:
To conduct a systematic review and meta-analysis of the literature on the perioperative outcomes of RAPN compared with OPN.
Methods:
We searched PubMed and EMBASE through January 31, 2016, to identify randomized controlled trials (RCTs) and observational comparative studies assessing the comparison of the two approaches (RAPN vs OPN). Primary outcomes were intraoperative complication rate and postoperative complication rate (including minor and major). Secondary outcomes were perioperative transfusion rate, positive surgical margin (PSM) rate, operative time (OT), warm ischemia time (WIT), estimated blood loss (EBL), length of hospital stay (LOS), and estimated glomerular filtration rate (eGFR) change.
Results:
A total of 19 cohort studies with at least 3551 patients (RAPN, 1216; OPN, 2335) were included. Compared with OPN, RAPN had the advantages of (a) lower rates of postoperative complication (risk ratio [RR] = 0.60, 95% confidence interval [CI] = 0.46, 0.78, p = 0.0002), postoperative minor complication (RR = 0.73, 95% CI = 0.56, 0.96, p = 0.02), and postoperative major complication (RR = 0.50, 95% CI = 0.30, 0.84, p = 0.01); (b) lower need for transfusion (RR = 0.64, 95% CI = 0.41, 0.98, p = 0.04); (c) less EBL (weighted mean difference [WMD] = −98.82, 95% CI = −125.64, −72.01, p < 0.00001); and (d) shorter LOS (WMD = −2.64, 95% CI = −3.27, −2.00, p < 0.00001). Sensitivity analyses excluding studies with obvious selection bias based on tumor complexity confirmed all these advantages. RAPN had longer OT (WMD = 18.56, 95% CI = 2.13, 35.00, p = 0.03) and WIT (WMD = 3.65, 95% CI = 0.75, 6.56, p = 0.01) in the primary analyses. Sensitivity analyses, however, showed no differences between RAPN and OPN regarding OT and WIT. Intraoperative complication rate (RR = 0.61, 95% CI = 0.29, 1.27, p = 0.19), PSM rate (RR = 0.87, 95% CI = 0.56, 1.34, p = 0.52), and short-term eGFR change, including absolute eGFR change (WMD = −1.56, 95% CI = −3.41, 0.28, p = 0.10) and percentage eGFR change (WMD = 0.99, 95% CI = −0.52, 2.50), did not differ between the two approaches.
Conclusions:
Compared with OPN, RAPN appears to have lower morbidity and achieves similar short-term functional outcomes. However, evidence is limited regarding the long-term oncologic outcomes even though the PSM rate is similar between the two groups. Well-designed RCTs with large sample sizes and long-term follow-up are needed to confirm and update the findings of our study.
Introduction
P
Previous large comparative studies and meta-analyses have already confirmed the significant advantages of RAPN over LPN. 9,10,12 So, as Mottrie et al. 11 have suggested, the real gold standard reference for RAPN outcome comparisons should be open partial nephrectomy (OPN), not LPN. For the past several years, a number of studies comparing perioperative outcomes between RAPN and OPN have been published with various results. 13 –31 With this in mind, we conducted a meta-analysis and systematically review the perioperative outcomes of RAPN vs OPN.
Methods
Search strategy
This systematic review and meta-analysis were conducted and reported in adherence to Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement (Supplementary Table S1; Supplementary Data are available online at
Selection criteria
Inclusion criteria were as follows: (a) studies comparing RAPN with OPN; (b) studies focusing on adult populations; (c) randomized controlled trials (RCTs) or observational cohort studies; (d) having, at least, one of the outcomes of interest. When two or more studies were reported by the same institutions and/or authors, or when two or more studies clearly had the duplicate patient population, the study with the largest sample size was included. However, if multiple studies with the same patient population had different outcomes of interest, they can be included for analysis separately.
Exclusion criteria were as follows: (a) RAPN/OPN only for benign tumors or bilateral tumors; (b) RAPN/OPN only in patients with solitary kidney; (c) single-port RAPN; (d) entirely zero-ischemia RAPN; (e) review articles, editorials, comments, letters to the editor, case reports, and conference abstracts; and (f) population-based studies.
Data extraction
Data extraction was performed by two reviewers and discrepancies were resolved by discussion. The following information was extracted from each study: authors; publication year; region; time period of RAPN/OPN; institutions; number of surgeons; number of patients; surgical approach; clamping method; study design; age; gender; body mass index (BMI); tumor size; tumor side; tumor location (upper/interpolar/lower); tumor depth (exophytic/mesophytic/endophytic); number of solitary kidney; number of malignant tumor; R.E.N.A.L score, preoperative aspects and dimensions used for an anatomical (PADUA) score, and outcomes of interest.
Total events, means, and standard deviations (SDs) were extracted from each study. Zero event studies were included. For studies presenting continuous data as median and/or range and/or interquartile range, the means and SDs were calculated using the methodology described by mathematicians and in the Cochrane handbook. 33 –35
Outcomes of interest
The primary outcomes were the intraoperative complication rate, overall postoperative complication rate, postoperative minor (Clavien–Dindo grades 1–2) complication rate, and postoperative major (Clavien–Dindo grades 3–4) complication rate. We defined major complication as Clavien–Dindo grades 3–4 since the perioperative mortality rate (Clavien–Dindo grade 5) of RAPN/OPN is rare.
The secondary outcomes were perioperative transfusion rate, positive surgical margin (PSM) rate, operative time (OT), warm ischemia time (WIT), estimated blood loss (EBL), length of hospital stay (LOS), and estimated glomerular filtration rate (eGFR) change.
Quality assessment
Quality assessment was performed by two reviewers and discrepancies were resolved by discussion. Cochrane risk of bias tool was used to assess the risk of bias for RCTs. 33 Observational studies were evaluated using the Newcastle–Ottawa Scale (NOS). 36 The NOS evaluates the quality of studies by examining three aspects of the study design: patient selection, comparability of the study groups, and assessment of outcomes. A score of 0–9 may be given to individual studies. Observational studies achieving a score of 6 or more indicate a high quality.
Statistical analysis
Meta-analysis
To be more conservative, the weighted mean difference (WMD) and risk ratio (RR) were used to compare continuous and dichotomous variables, respectively. The Mantel–Haenszel method with random-effects model was used to calculate pooled RRs and 95% confidence intervals (CIs). The inverse variance method with random-effects model was used to calculate pooled WMDs and 95% CIs. p < 0.05 was considered statistically significant.
Statistical heterogeneity
Statistical heterogeneity between studies was assessed using the chi-square (χ 2) test with significance set at p < 0.10. Heterogeneity was also quantified using the I 2 statistic. I 2, which is ranging from 0% to 100%, measures the degree of inconsistency across studies in a meta-analysis. 37 I 2 values of 25%, 50%, and 75% were deemed as low, moderate, and high heterogeneity. 37 Usually, I 2 value greater than 50% suggests significant heterogeneity in the reported effect sizes. 38
Sensitivity analysis
Due to the fact that RAPNs were usually performed for less complex tumors compared with OPN, we excluded the studies in which obvious selection bias existed for the sensitivity analysis. The R.E.N.A.L score and PADUA score are two commonly used tools classifying tumor complexity. 39,40 Obvious selection bias was defined as having unmatched R.E.N.A.L score or PADUA score between RAPN and OPN groups. If neither the R.E.N.A.L score nor PADUA score was reported, obvious selection bias was defined as having unmatched tumor size between RAPN and OPN groups. Remaining studies were included for sensitivity analysis.
Subgroup analyses
We chose postoperative complication rate for subgroup analyses since it has a decent number of included studies and has relatively more clinical significance. Subgroup analyses were conducted according to study design (prospective vs retrospective), setting (single center vs multicenter), sample size (≥200 vs <200), and region (Asia vs Europe vs the United States).
Publication bias
Publication bias was assessed by visually inspecting a funnel plot in which the logRRs or WMDs were plotted against their standard errors. The presence of publication bias was also evaluated by Begg's and Egger's tests. p < 0.05 was considered statistically significant.
Software
Excel 2013 (Microsoft Corporation), Review Manager 5.3 (Cochrane Collaboration), and STATA 14.0 (StataCorp LP).
Results
Literature search
The PRISMA flow diagram is shown in Figure 1. A total of 1491 studies were identified from the initial database search. Five hundred thirty-eight were excluded for duplication. The remaining 953 records were screened based on titles and abstracts. After exclusion of 903 studies from screening, 43 potentially eligible studies were reviewed based on full-text. In this process, another 24 studies were excluded for not meeting our inclusion criteria or falling into exclusion criteria. Finally, 19 studies were included in the meta-analysis. 13 –31

Flow diagram of studies identified, included, and excluded. RAPN = robot-assisted partial nephrectomy; LPN = laparoscopic partial nephrectomy.
Study characteristics
The main characteristics of the included studies are shown in Table 1. These studies were published between 2011 and 2015. The sample size ranged from 31 to 501. Two studies 15,18 and another two studies 24,27 shared some duplicate patient populations and had different outcomes of interest. After excluding the potential maximum overlapping patients, the total patient number was 3551 (RAPN group, 1216; OPN group, 2335). All studies were observational cohort studies, eight of them were prospective and 11 were retrospective. Five studies were multicenter studies. Among the 19 studies, eight of them were conducted in the United States, six in Europe, five in Asia. Some of the outcomes in the study of Simhan and colleagues 28 had to be pooled into two separate groups because the comparisons in the original study were stratified by a moderately and highly complex group (labeled as Simhan M and Simhan C, respectively) based on the R.E.N.A.L score.
RAPN = robot-assisted partial nephrectomy; OPN = open partial nephrectomy; / = not available.
Based on the Newcastle–Ottawa Scale (details in Supplementary Table S2).
Patient and tumor characteristics of the included studies are shown in Table 2. Mean/median patient age of the RAPN group ranged from 52.5 to 63.3 years old (OPN, 52–65 years old). Mean/median patient BMI of the RAPN group ranged from 24.8 to 31.4 kg/m2 (OPN, 24.4–30.1 kg/m2). Mean/median tumor size of the RAPN group ranged from 20 to 50 mm (OPN, 23–54 mm).
Continuous variables were reported as mean or median.
Match factors (details in Supplementary Table S3): 1 = age; 2 = gender; 3 = BMI; 4 = American Society of Anesthesiology (ASA) score; 5 = Charlson Comorbidity Index (CCI); 6 = tumor size; 7 = tumor laterality (left/right); 8 = tumor location (upper/interpolar/lower pole); 9 = tumor depth (exophytic/mesophytic/endophytic); 10 = R.E.N.A.L score; 11 = PADUA score; 12 = clamping method; 13 = solitary kidney; 14 = previous abdominal surgery; 15 = preoperative estimated glomerular filtration rate (eGFR); 16 = preoperative creatinine.
BMI = body mass index; PADUA = preoperative aspects and dimensions used for an anatomical; / = not available.
Quality assessment
Quality assessments of included studies are shown in Table 1 and Supplementary Table S2. Based on the NOS to assess the risk of bias of the cohort studies, one study was rated as a total score of 6, two studies as a score of 7, five studies as a score of 8, and 11 studies as a score of 9. So, all observational studies had a score of ≥6 and were considered high quality.
Primary outcomes
Meta-analyses of primary outcomes are shown in Table 3 and Figure 2.

Forest plots of primary and secondary outcomes:
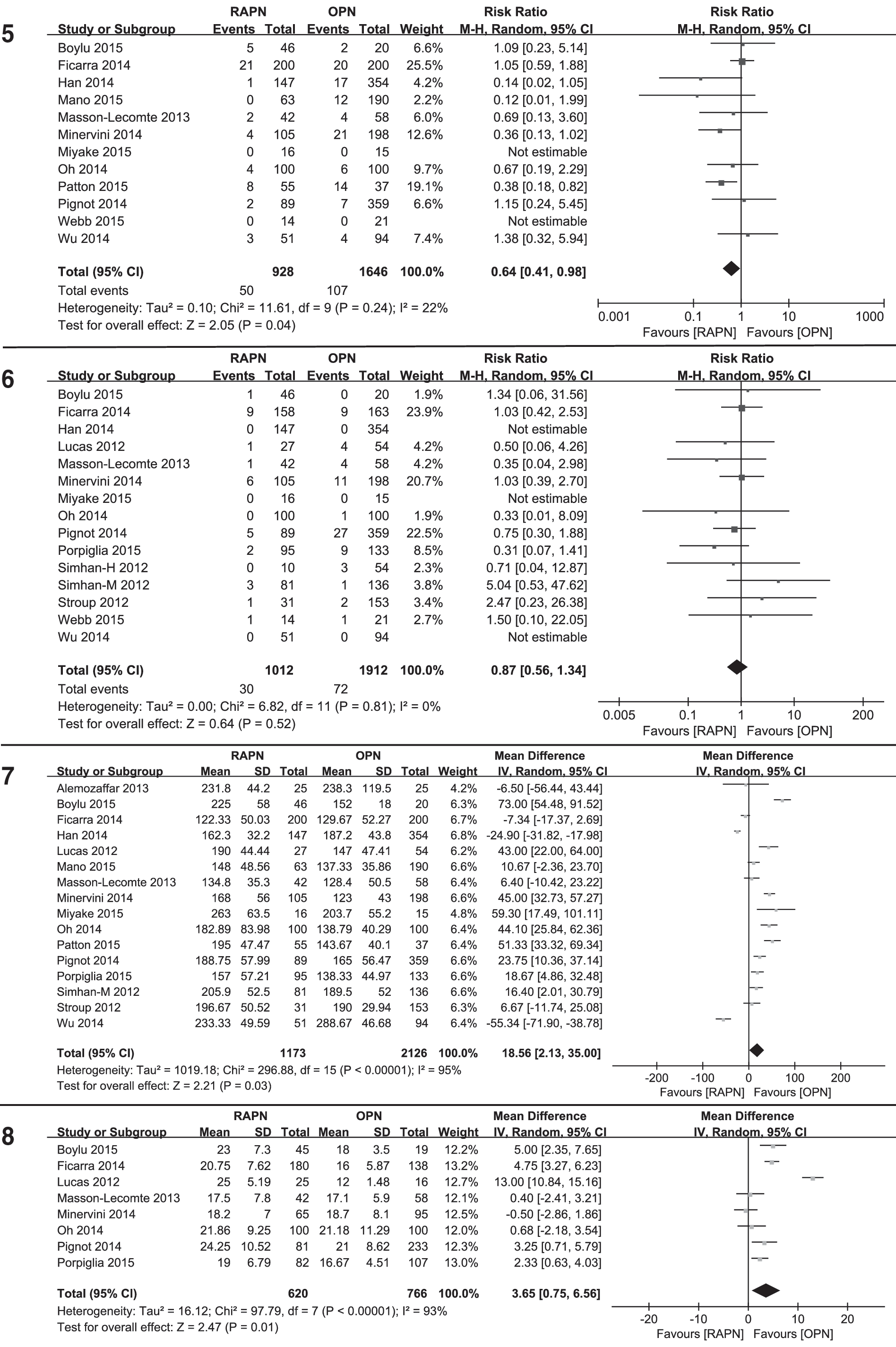
WMD.
Statistically significant results are shown in bold.
RR = risk ratio; WMD = weighted mean difference; CI = confidence interval; minor = Clavien–Dindo grades 1–2; major = Clavien–Dindo grades 3–4; eGFR = estimated glomerular filtration rate.
Intraoperative complications
Pooling data from nine studies 14,15,19,22 –24,27,30,31 that assessed intraoperative complications in 1489 patients showed no significant difference between the RAPN and OPN groups (RR [95% CI]: 0.61 [0.29, 1.27], p = 0.19).
Postoperative complications
A total of 13 studies 15,16,18 –23,25,27,29 –31 provided the data of overall postoperative complication, but the time frame of the postoperative complications varied. Three studies 20,26,29 defined it as complications that happened within 30 days of the date of surgery, one 15 as within 90 days of the date of surgery, and another one 31 as during hospital stay. Eight studies 16,18,19,21,22,25,27 did not specify the time frame of the postoperative complication. Pooling data from the 13 studies 15,16,18 –23,25,27,29 –31 that assessed postoperative complications in 2656 patients showed a significantly lower rate of postoperative complication in the RAPN vs OPN groups (RR [95% CI]: 0.60 [0.46, 0.78], p = 0.0002).
Overall postoperative complications were further divided into minor and major complications in the original 13 studies. 15,16,18 –23,25,27,29 –31 There was a significantly lower minor complication rate (RR [95% CI]: 0.73 [0.56, 0.96], p = 0.02) and a significantly lower major complication rate (RR [95% CI]: 0.50 [0.30, 0.84], p = 0.01) in the RAPN vs OPN groups.
Secondary outcomes
Meta-analyses of secondary outcomes are shown in Table 3 and Figure 2.
Perioperative transfusion
Pooling data from 12 studies 14 –16,20 –26,30,31 that assessed perioperative transfusions in 2574 patients showed a significantly lower rate of perioperative transfusion in the RAPN vs OPN groups (RR [95% CI]: 0.64 [0.41, 0.98], p = 0.04).
Positive surgical margin
Pooling data from 15 studies 14 –16,19,21 –24,26 –31 that assessed PSMs in 2924 patients showed no significant difference between the RAPN and OPN groups (RR [95% CI]: 0.87 [0.56, 1.34], p = 0.52).
Operative time
Pooling data from 16 studies 13 –16,19 –29,31 that assessed OTs in 3299 patients showed significantly longer OT in the RAPN vs OPN groups (WMD [95% CI]: 18.56 [2.13, 35.00], p = 0.03).
Warm ischemia time
For WIT, patients who underwent cold ischemia and/or off-clamp techniques in the RAPN and OPN groups were excluded. Studies in which cold ischemia was used in the OPN group were excluded. Pooling data from eight studies 14,15,19,21,22,24,26,27 that assessed WITs in 1386 patients showed significantly longer WIT in the RAPN vs OPN groups (WMD [95% CI]: 3.65 [0.75, 6.56], p = 0.01).
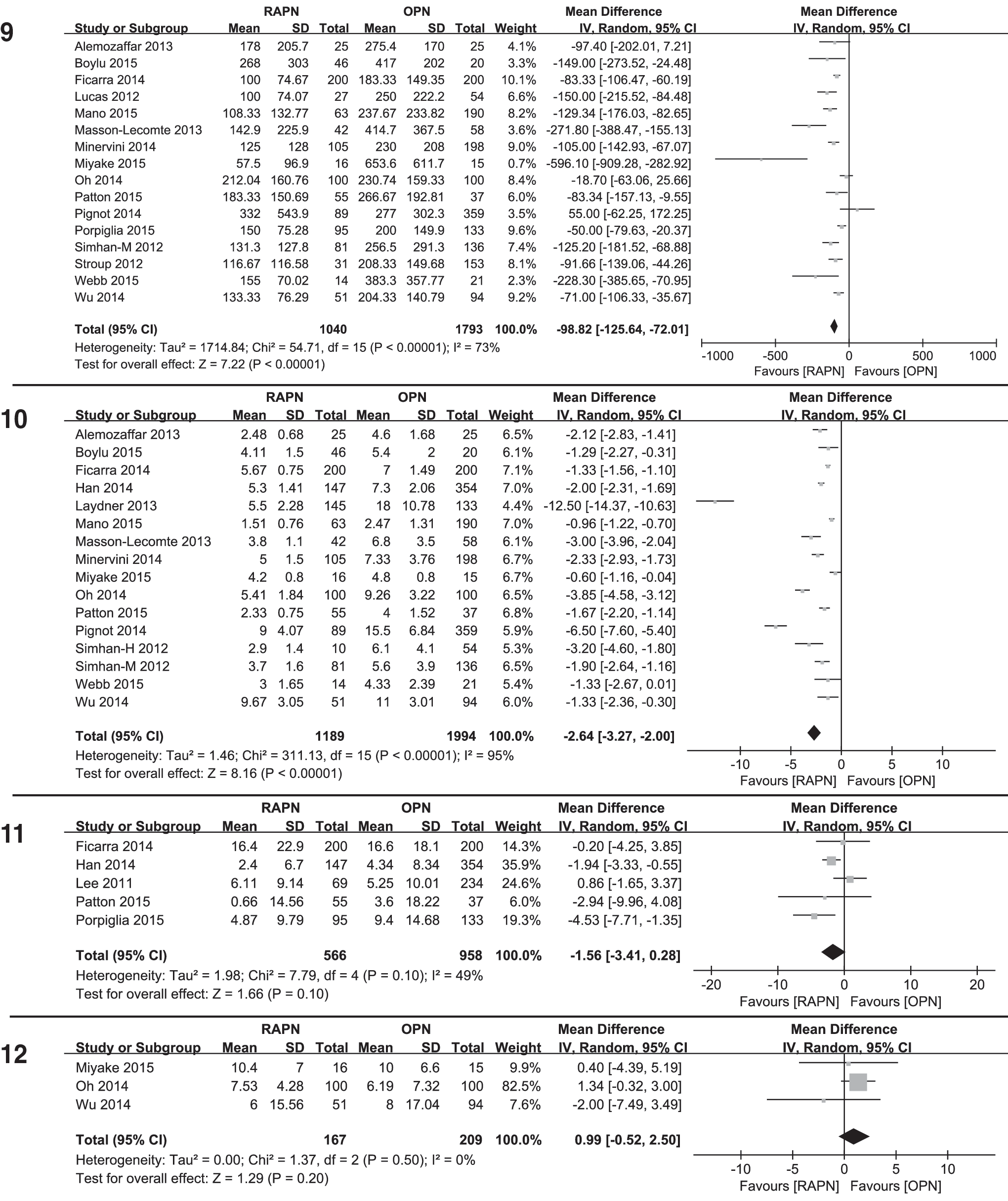
Estimated blood loss
Pooling data from 16 studies 13 –15,19 –31 that assessed EBL in 2833 patients showed a significantly lower EBL in the RAPN vs OPN groups (WMD [95% CI]: −98.82 [−125.64, −72.01], p < 0.00001).
Length of hospital stay
Pooling data from 16 studies 13 –17,20 –26,28,30,31 that assessed LOSs in 2783 patients showed significantly shorter LOS in the RAPN vs OPN groups (WMD [95% CI]: −2.64 [−3.27, −2.00], p < 0.00001).
eGFR change
Five studies 15,16,18,25,27 reported postoperative absolute eGFR decline and another three studies 23,24,31 reported percentage eGFR decline with extractable data. The postoperative eGFRs were assessed at postoperative 1 month in three studies, 18,23,27 3 months in two studies, 15,31 and 6 months in one study. 24 In another two studies, 16,25 assessment time of postoperative eGFRs was not clear.
Pooling data from five studies 15,16,18,25,27 that assessed absolute eGFR decline showed no significant difference between the RAPN and OPN groups (WMD [95% CI]: −1.56 [−3.41, 0.28], p = 0.10).
Pooling data from three studies 23,24,31 that assessed percentage eGFR decline showed no significant difference between the RAPN and OPN groups (WMD [95% CI]: 0.99 [−0.52, 2.50], p = 0.20).
Sensitivity analyses
Sensitivity analyses of all the primary and secondary outcomes are shown in Table 4 and Supplementary Figure S1. Sensitivity analyses included 13 studies 13,15,16,18 –20,22 –25,27,30,31 after excluding studies 14,17,21,26,28,29 with obvious selection bias. Of the excluded studies, three of them 14,21,29 had unmatched R.E.N.A.L score and another three 17,26,28 had unmatched tumor size between the RAPN and OPN groups. p-Value of OT changed from 0.03 to 0.15 (compared with primary meta-analysis), which indicated no significant difference between the RAPN and OPN groups. p-Value of WIT changed from 0.01 to 0.06 (compared with primary meta-analysis), which indicated no significant difference between the RAPN and OPN groups. p-Values of other outcomes of interest remain significant (<0.05) or nonsignificant (≥0.05) after sensitivity analyses.
WMD.
Statistically significant results are shown in bold.
Minor = Clavien–Dindo grades 1–2; major = Clavien–Dindo grades 3–4.
Subgroup analyses
Subgroup analyses of overall postoperative complication rate are shown in Table 5 and Supplementary Figure S2. The findings of lower postoperative complication rate were consistent in all subgroup analyses except for the single-center, sample size <200, Asian, and US subgroups. Subgroup differences were found in study design and sample size.
Statistically significant results are shown in bold.
Publication bias
All the funnel plots are shown in Figure 3. All the Begg's and Egger's tests are shown in Tables 3 and 4. The funnel plots and Begg's and Egger's tests showed no evidence of significant publication bias for intraoperative complication, postoperative complication, minor postoperative complication, major postoperative complication, transfusion, PSM, WIT, absolute eGFR decline, and percentage eGFR decline. Potential publication biases were seen in OT, EBL, and LOS.
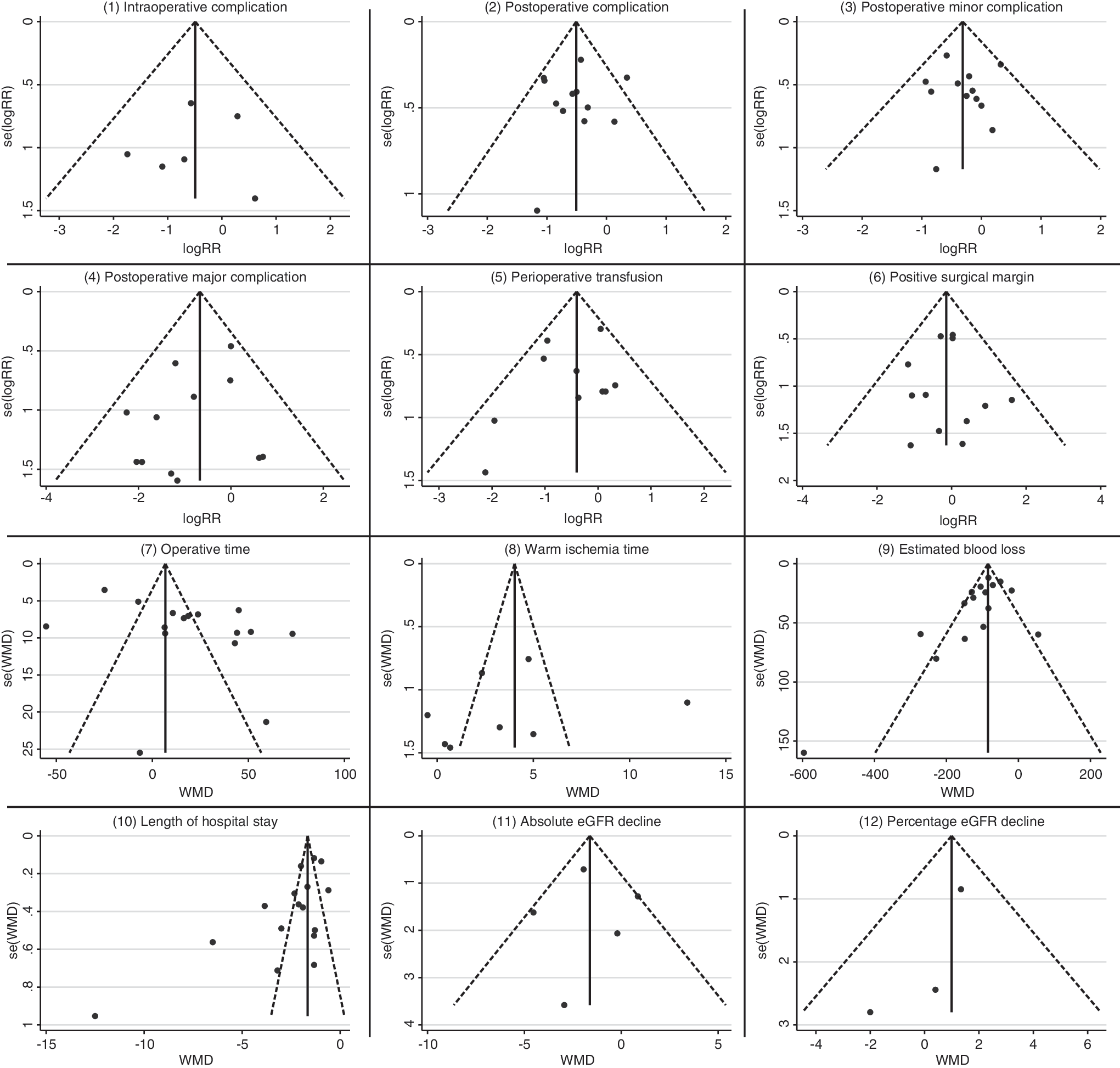
Funnel plots of primary and secondary outcomes:
Discussion
Main findings
The present systematic review and meta-analysis identified 19 studies comparing RAPN with OPN in terms of perioperative outcomes. The primary meta-analyses (Table 3; Fig. 2) showed that compared with OPN, RAPN had the following advantages: (a) lower rates of intraoperative complication, overall postoperative complication, postoperative minor and major complication; (b) lower transfusion rate; (c) less EBL; and (d) shorter LOS. However, the OPN group had a significantly shorter OT and WIT. No significant difference was found regarding PSM and eGFR decline between the two groups. After excluding studies with obvious selection bias based on tumor complexity, sensitivity analyses showed the same results for all the outcomes of interest except OT and WIT, both of which became nonsignificant (Table 4).
Comparison with one previous systematic review and meta-analysis
One previous meta-analysis on this topic, which included eight studies with a total of 3418 patients, was published in 2014. 41 There was one major flaw in their meta-analysis even though the sample size was almost the same as ours. 41 It is noticeable that more than half of their patient sample came from one population-based study (2022 patients). 41,42 In contrast, included in our meta-analysis were entirely single-center or multicenter studies. We excluded the population-based study because single-center or multicenter studies can provide more precise or detailed clinical information. Also, population-based studies themselves can be considered as heterogeneous factors, which can affect the results. 43,44 After the publication of the previous meta-analysis, several high-quality observational studies comparing RAPN with OPN were published. 15,24 –27,31 Therefore, our meta-analysis can provide the most updated and comprehensive evidence on this topic.
Implications for clinical practice
Although there were more studies comparing RAPN with LPN than RAPN with OPN, using OPN as the reference of RAPN might have more clinical significance. 11 Like Mottrie et al. 11 commented, traditional laparoscopy might not be the real competitor of RAPN. Large comparative studies and meta-analyses have demonstrated that compared with LPN, RAPN had the advantages of lower complication rate, less EBL, and shorter WIT. 9,10,12,45 Therefore, except for the cosmetic advantage, whether RAPN has other benefits over OPN is a topic worth clarifying.
Two facts need to be addressed before interpreting the clinical significance of our study. First, most of the outcomes of interest were procedure related, which can only provide early safety and efficacy evaluations. Second, match factors were reported in our results (Table 2 and Supplementary Table S3) and it was clear that selection bias existed. Although we excluded the obvious selection bias in the sensitivity analysis (Table 4), it was not possible to entirely eliminate the effects of selection bias considering all included studies were observational.
Optimal PN has three objectives: (a) minimalizing perioperative complications; (b) completely removing the tumor; and (c) maximally preserving remaining renal function. Previously proposed “trifecta,” “MIC,” or other combined outcomes were all based on these three objectives. 46 –50 Although we did not have enough studies to directly compare the “trifecta” or “MIC” achievements between RAPN and OPN, most of the individual outcomes were reported in our meta-analysis. In our meta-analysis, safety outcome was reported as intraoperative complication, postoperative complication, transfusion, and EBL; cancer control outcome was reported as PSM; and renal function outcome was reported as WIT and eGFR decline. Although PSM and WIT cannot truly reflect the cancer control and renal function preservation, respectively, they are generally used as the surrogates and long-term follow-up data are still not available. So, we believe our meta-analyses have enough outcomes of interest to assess the performance difference between RAPN and OPN.
Fewer postoperative complications were seen in the RAPN group than OPN group. Furthermore, both postoperative minor and major complications were more frequently seen in the OPN group. However, there was no difference regarding intraoperative complication between the two groups. The possible reason is that intraoperative complication was much rarer than postoperative complication and the absolute difference might be diluted. Compared with OPN, RAPN also had the advantages of less EBL and fewer transfusions. Based on the current evidence, it appears that RAPN offers more than not just cosmetic benefits but also lower morbidity.
As for cancer control, no direct comparison of RAPN vs OPN in terms of long-term outcomes (overall survival, cancer-specific survival, and recurrence) has been reported in the literature to date. Our meta-analysis only showed a similar PSM rate between RAPN and OPN groups. Although the impact of PSM on the long-term oncologic outcomes of patients with kidney cancer remains debatable, complete removal of the tumor and achieving a negative margin is undoubtedly one critical goal of PN. 51 –53 Andrade and colleagues 54 recently reported the longest follow-up data on RAPN and the 5-year overall survival, cancer-free survival, and cancer-specific survival were 91.1%, 97.8%, and 97.8%, respectively. Another two studies with intermediate-term follow-up also showed that recurrence and survival outcomes of RAPN were similar to those reported for OPN and LPN. 55,56 Also, one previous meta-analysis revealed that there was no significant difference in survival outcome between LPN and OPN for the treatment of localized kidney cancer. 57 RAPN is nothing but more advanced LPN, so based on all these studies combined with our results, it is safe to say that RAPN, at least, has noninferior oncologic outcomes compared with OPN.
Our primary analysis showed that OPN had the shorter WIT compared with RAPN. However, the sensitivity analysis showed no significant difference. Furthermore, there was no difference between the two groups regarding postoperative eGFR decline. Although WIT is an important predictor of postoperative renal function, it certainly is not the only factor. 58 –61 In fact, one major advantage of RAPN compared with LPN is WIT according to previous studies. 10,62 –64 The WIT of RAPN is generally brief because of the improved ability to suture with RAPN compared with LPN. In experienced hands and appropriate patient selection, the WIT of RAPN can be controlled to less than 20 minutes. 9,15,21,27,48 So, the marginal difference of WIT between RAPN and OPN may not have much clinical significance for patients with adequate renal reserve. Also, off-clamp or selective artery clamp RAPN can be applied to limit the renal function loss for patients with compromised renal function even though the benefit from those techniques is still controversial. 65 –68 However, in patients with marginal renal function or where a complex renal reconstruction may be anticipated, OPN may still remain the procedure of choice. For all comers, however, functional outcomes are generally comparable between the RAPN and OPN groups.
In our primary meta-analysis, OT was longer in the RAPN group, which is understandable considering the docking time was included in most of the studies. The different result demonstrated by the sensitivity analysis could simply be explained by the fact that heterogeneity between studies was large. The shorter LOS in our results can be considered as another benefit of RAPN, which could be possibly explained by the less invasive approach and lower postoperative complication rate. Also, the shorter LOS of LPN has already been reported in the comparison of OPN. 7,69 The shorter LOS has the potential to lower cost of hospitalization, which may offset the higher operating room costs of RAPN. 13,17,20 In other words, the advantages of RAPN may enable cost equivalence between RAPN and OPN. 13,17
One hidden point from our meta-analysis and included studies is that robotic technology has expanded the indications of minimally invasive PN. 23,25,27 –29 More complex renal masses are being managed with RAPN instead of OPN and the robot platform can help narrow the gap that has long existed between PN and RN. 25,70,71 Furthermore, even for complex renal masses, RAPN can still offer significant lower morbidity and simultaneously achieve oncologic and functional outcomes comparable to OPN. 23,25,27,28
Strengths and limitations
Major strengths of our meta-analysis included the compliance with the PRISMA guideline, extended search, critical assessment, substantial analyses, including sensitivity analyses accounting for the tumor complexity, all of which made it the most comprehensive evidence regarding RAPN vs OPN to date. Since there are still no RCTs comparing RAPN and OPN, our meta-analysis might contribute to the literature in a meaningful way.
However, there are several limitations in the current meta-analysis that must be acknowledged. First, the protocol for this meta-analysis was not registered before. Second, selection biases were inevitable considering all included studies were observational and only 8 of them were claimed prospective. We conducted a sensitivity analysis to limit the bias from tumor complexity, but other selection biases were not explored. Third, the learning curve of the surgeons, especially in RAPN, was not accounted for before conducting the analyses, which could further skew our results. Worth mentioning, most of the studies did declare that the surgeons in their series were beyond the learning curve. Fourth, heterogeneities among the studies for OT, WIT, EBL, and LOS were relatively high (Table 3). The possible explanation is that all of them are continuous variables and it is also relatively harder to document them in a unified method. On the contrary, categorical variables tend to have low heterogeneities.
Conclusions
This meta-analysis indicates that compared with OPN, RAPN appears to be associated with fewer postoperative complications (including both minor and major complications), lower need for transfusion, less EBL, and shorter LOS. Although OPN has shorter WIT, short-term postoperative GFR decline is comparable between RAPN and OPN. There is no difference between the RAPN and OPN in terms of PSM. Well-designed RCTs with large sample size and long-term follow-up are still needed to confirm and update the findings of our study.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.