
Abstract
Introduction:
Laparoscopic access for robot-assisted radical prostatectomy (RARP) is often initiated in the periumbilical location. Palmer's point, located in the left upper quadrant, has been reported as an alternative access site for pelvic laparoscopy to reduce morbidity, but not widely reported among urologists. To better understand surgeons' preferences for access and its associated morbidity during RARP, we surveyed surgeons from two urologic organizations.
Methods:
An anonymous online questionnaire (SurveyMonkey) consisting of 17 questions that assessed training, experience, and preferences for RARP was emailed in December 2014 and collected until February 2015 to members performing RARP of the Endourology Society (ES) and the Michigan Urological Society Improvement Collaborative (MUSIC). Surgeons were also asked to share their personal experience with a vascular, death or life-threatening event (DOLTE), or bowel injury during RARP.
Results:
Questionnaires were answered by 111 surgeons in total (ES, n = 71 and MUSIC, n = 40) with an estimated total response rate of 5.5%. In total, 77% reported prior experience with the Veress needle method before exposure to RARP and 71% of respondents primarily use the Veress needle for RARP, with 73% reporting access primarily at the periumbilical location. A personal experience with a vascular or a bowel injury during Veress needle insertion was reported in 18% and 9% of surgeons, respectively; furthermore, 26% of respondents were personally aware of at least 1 DOLTE among colleagues (5% reported 3 or more). The majority (56%) of respondents were unaware of Palmer's point, while among the minority aware of Palmer's point, only 33% reported ever using this location.
Conclusion:
In this survey, surgeons most commonly access the abdomen at the periumbilical location with a Veress needle for RARP with the majority not aware or utilizing Palmer's point. Nearly one in five surgeons reported a personal experience with a vascular injury during access for RARP. Palmer's point, located away from major vasculature, may reduce the morbidity of access for RARP and warrants further awareness and study.
Introduction
W
Gynecologic surgeons reported the first laparoscopic organ removal in 1981 (salpingectomy) and have since recorded the greatest number of laparoscopic and robotic pelvic surgeries of all specialties. 1 Within this surgical subspecialty, numerous publications have addressed vascular injuries during initial access/insufflation and have proposed Palmer's point, located in the left upper quadrant—3 cm below the left costal margin on the midclavicular line—as an alternative access location to minimize intra-abdominal injury 2 (Fig. 1). Within the urology literature, however, only one study has reported the use of Palmer's point access for robotic pelvic surgery 3 and there are no reports specifically examining the incidence of vascular injuries during access for RARP.

Palmer's point for RARP: Palmer's point is located 3 cm below the left costal margin on the midclavicular line. For RARP, this location avoids major vessels and, at 6–7 cm lateral to the midline and two finger breaths below costal margin, avoids epigastric vessels. RARP = robot-assisted radical prostatectomy.
The Michigan Urological Surgery Improvement Collaborative (MUSIC) is a consortium of 42 academic and community urology practices across the state of Michigan focused at improving prostate cancer care. Currently, MUSIC is assessing and establishing technical benchmarks for RARP, including the evaluation of surgeons performing this procedure. 4 In this context, surgeons from MUSIC sought to better understand preferences for access, associated morbidity, and awareness or utilization of Palmer's point for RARP. Furthermore, we wanted to assess these preferences in comparison to specialists performing this procedure outside of Michigan. For these reasons, we surveyed surgeons from MUSIC and the Endourology Society (ES)—a diverse specialty of minimally invasive urologists spanning the globe—on their experience surrounding laparoscopic access for RARP.
Methods
An anonymous online questionnaire consisting of 17 questions that assessed training, experience, and preferences for laparoscopic access for RARP was emailed in December 2014 and collected until February 2015 to all members of the ES and MUSIC (Appendix A1). The ES is a global society with interests in endourology and minimally invasive urology. MUSIC is a quality improvement consortium funded by the Blue Cross Blue Shield of Michigan consisting of 42 urology practices across Michigan, encompassing 90% of all practicing urologists in the state. 5 The ES is composed of ∼1850 members, while 150 urologists in MUSIC were contacted. The email asked for responses from surgeons performing RARP and all questions pertained to RARP. Responses were collected through the SurveyMonkey system over a 2-month period and respondents of both organizations were requested to complete only one survey. Questions polled respondents regarding their experience with RARP (i.e., number of cases performed, when they received the majority of their Veress needle training (residency, fellowship), and their preferred insufflation access location and technique (Veress, visual obturator, open Hasson, or other). Surgeons were also asked to share their personal experience with a vascular or bowel injury during initial laparoscopic access, as well as their awareness of a vascular death or life-threatening event (DOLTE) among colleagues (“none,” “1 injury,” “2 injuries,” “3 or more,” “would rather not comment”). Respondents were further questioned on their familiarity, frequency, and possible reasons for utilizing Palmer's point for access. Outcomes from the survey were analyzed using summary statistics, collectively for the two groups.
Results
Demographics
Questionnaires were answered by 111 surgeons in total (ES, n = 71 and MUSIC, n = 40) with an estimated total response rate of 5.5%. While data on the total number of ES members specifically practicing RARP are unknown, ∼100 members of MUSIC are known to be performing RARP, of which 40 responded to the survey (40% response rate). Table 1 summarizes and compares responses across the two groups. In the total cohort, 33% of respondents received training in laparoscopic access during residency and 41% reported completing fellowships with robotic training. Among the respondents, 30% reported 1 to 5 years of experience performing RARP while 63% reported greater than 5 years with this operation. In terms of specific case volume, 69% of respondents reported performing >100 RARPs, including 44% with >250 cases.
MUSIC = Michigan Urological Society Improvement Collaborative; RALP = robot-assisted laparoscopic prostatectomy; RARP = robot-assisted radical prostatectomy.
Experience with Veress needle technique
When questioned on access preference, 71% gained access primarily with a Veress needle and, less commonly, reported using the Hasson technique (20%), visual obturator technique (5%), or some combination of the above (4%) as their technical approach for insufflation (Fig. 2). Most surgeons (78%) reported gaining experience with Veress needle insertions before performing their first RARP, and the vast majority (69%) reported experience with a Veress needle during their residency and/or fellowship training.

Urologists' reported preferred technique for abdominal access and insufflation for RARP.
Complications
Respondents were also questioned on their personal experience or knowledge of major intraoperative complications associated with Veress needle access. Four percent of respondents elected to not respond to the questions regarding personal experience or knowledge of a DOLTE, of which, none of these provided a reason for choosing “would rather not comment.” Eighteen percent of surgeons reported a personal experience with a vascular injury and 9% reported a personal experience with a bowel injury. Twenty-six percent of respondents reported personal knowledge of colleagues who experienced a vascular injury resulting in a DOLTE; 5% of respondents reported knowledge of 3 or more DOLTEs (Fig. 3).
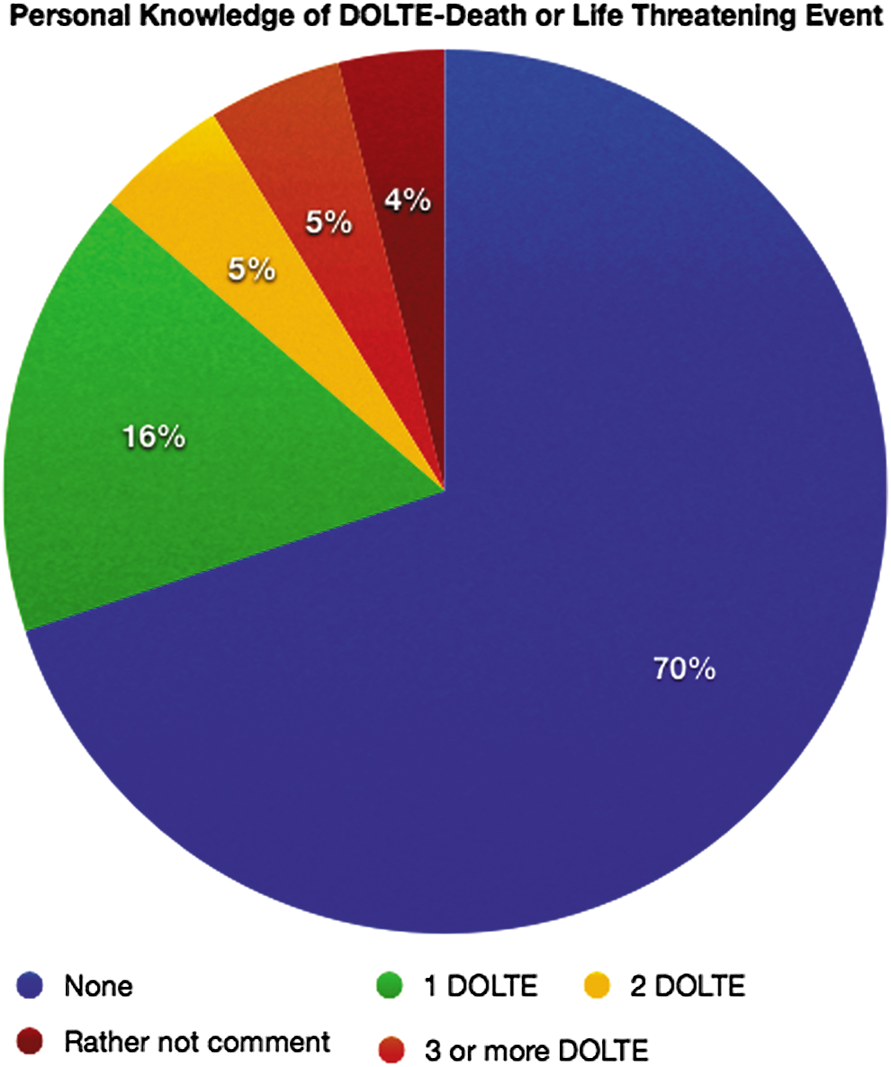
Respondents' reported personal knowledge of a death or life-threatening event (DOLTE) among colleagues.
Awareness of Palmer's point
Most surgeons (73%) gained access at the periumbilical area. The majority of respondents (57%) were unfamiliar with Palmer's point as a site for access during RARP, and of those aware of Palmer's point, 68% reported never accessing at this location. Only 8% used Palmer's point as their primary access site. Among the minority of surgeons familiar with Palmer's point, 36% chose Palmer's point as an alternative access site only when periumbilical scarring/adhesions are suspected from prior periumbilical entry.
Discussion
This survey highlights the collective responses from a global survey of an experienced cohort of robotic surgeons performing RARP. With no published articles specifically addressing vascular injuries during RARP access within the literature and with the initial findings of our survey aiming to raise awareness among the practicing robotic surgeons, the authors feel the article has important implications for the practicing urologist and for patient safety.
We found that most surgeons utilized the umbilical area for entry with Veress needle for laparoscopic access for RARP. Even among this experienced cohort, our survey revealed that 18% of practicing RARP surgeons have experienced at least one vascular injury during access, yet most surgeons were unaware of or not utilizing Palmer's point as an alternative access site.
The topic of laparoscopic access and morbidity for RARP has not been widely addressed, and studies specifically addressing this are limited. Tufek and colleagues, in the only published report on Palmer's point use in RARP, reported effective access with the first attempt in 93% of their 126 patients examined, with no vascular injuries or complications. 3 Multiple studies within the gynecologic literature have established the risk of vascular injury during access for laparoscopic pelvic surgeries at the periumbilical location and have proposed Palmer's point as an alternative access location to minimize intra-abdominal injury. 1,2 Furthermore, our survey may under-represent that seen in less experienced robotic environments with 41% of respondents in this survey having completed fellowship training in robotics and over 44% reporting experience in >250 cases.
While data on complications during access for urologic pelvic procedures are limited, studies from general surgery and gynecology inform us on the frequency of these events. A recently published study in the Cochrane Database found a rate of eight vascular injuries per 1000 laparoscopic cases (or one vascular event per 125 cases). 6 Saville and Woods reported four major vascular injuries in 3591 general laparoscopic procedures over a 3.5-year period, or approximately one injury per 1000 cases. 7 Jones and colleagues examining gynecologic surgeries reported vascular injuries in 1 out of 469 cases. 8 Despite these findings from gynecologic surgeons performing pelvic laparoscopy, urologists performing RARP have traditionally chosen the periumbilical location for laparoscopic access. As noted in our study, this may be due to the majority of surgeons gaining experience with Veress at the umbilicus for upper tract surgery before performing RARP.
This study does have some limitations. First, the survey was sent to electronic addresses available from two societies' database, however, the exact number of urologists who actually received this email, the number of functional/active/duplicate email accounts, and that the email requested only members performing RARP and all questions pertained to robotic prostatectomy must be taken into account and limit interpretation on response rates. The survey did not ask for country of origin, institution type, or location of the practice; the latter may have led to concerns with keeping the answer anonymous. Second, this study surveyed a robotic surgeon's personal experience with a vascular injury and his or her knowledge of a DOLTE among colleagues, with the latter opening the possibility of a single DOLTE being reported by more than one surgeon. Also, it is unclear if concerns such as fear of liability, denial, or suppression of a traumatic event led to the small proportion of surgeons who failed to answer the question on a DOLTE. Last, the survey asked for vascular injuries during access, but did not specify the vessel or organ injured or technique associated with the injury. Although higher response rates are always desired, current trends show that online response rates in recently published urology studies survey practice patterns report rates of 10%. 9 Furthermore, Table 1 shows the data from the ES and MUSIC, of which MUSIC had a 40% response rate, with similar survey outcomes to the ES.
These limitations not withstanding, our findings have significant implications for surgeons performing RARP by raising more awareness of the morbidity associated with access for RARP and offering a possible alternative technique, largely not practiced or known among urologists. Traditionally, techniques evolve over time and are often passed down through academic training and publications. Change to any techniques, however, may often be met with resistance as the status quo is familiar to the surgeon and an attitude that serious adverse events from access are rare. In our study, two-thirds of surgeons were unfamiliar with Palmer's point as a laparoscopic access site. The data from our survey, however, suggest that the incidence of a vascular injury is not uncommon with 18% of surgeons reporting a personal experience with a vascular injury at some point in their career. As surgeons, statistics can help us assess risk and guide change, but when we examine data that fail to reach statistical significance, we are satisfied we are performing at acceptable standards. When considering more serious events, however, our bull's eye should always be a numerator of zero, irrespective of the denominator.
Moving forward, our findings highlight the relative lack of knowledge of Palmer's point among practicing robotic surgeons. Palmer's point offers a primary access location or an alternative access site when periumbilical scarring is suspected after previous open or laparoscopic access. Moving the access away from the periumbilical region can help shift the line of fire away from the great vessels that traverses in the midline (Fig. 1). While the surgeon can direct periumbilical access caudally (potentially below the bifurcation), the aortic and inferior vena cava bifurcation is located at a mean of 0.8 and 2.5 cm below the umbilicus, respectively, but anatomic variation can vary this location both caudal and cranial. 10 Furthermore, needle deflection or misdirection could lead to inadvertent entry into a great vessel. Last, previous laparoscopic surgeries that have used periumbilical access, such as cholecystectomy, hernia (mesh), and appendectomy, can lead to scar tissue or bowel adhesions and lead to deflection or over penetration during abdominal access. As the first published study examining RARP vascular access injury, we agree that prospective studies are indicated and hope this article serves as the springboard for greater understanding and patient safety.
Conclusion
In this survey, nearly one in five surgeons reported a personal experience with a vascular injury during access for RARP. Most surgeons reported use of a Veress needle through a periumbilical location, but were unaware or not utilizing Palmer's point for access. Palmer's point, with its location away from the great vessels, may decrease vascular injury during access for RARP and warrants further study to increase awareness and evaluate whether use of Palmer's point can reduce morbidity for RARP.
Footnotes
Author Disclosure Statement
No competing financial interests exist.