
Abstract
Objective:
To compare the efficacy between motorized articulating instruments (AI) and rigid conventional laparoscopic instruments (CI) in chancing visualizing systems, respectively two-dimension (2D) and three-dimension (3D).
Methods:
Sixty physicians were divided into three groups according to their previous experience as medical students (Group 1), residents (Group 2), and expert surgeons (Group 3). Four experimental sets were created, respectively CI-2D visualizing system (CI-2D), CI-3D visualizing system (CI-3D), AI-2D visualizing system (AI-2D), and AI-3D visualizing system (AI-3D) platforms. European training in basic laparoscopic urological skills (E-BLUS) and anastomosis tasks (ın total five tasks) was used. All participants were randomly required to perform tasks in each one of the technical platforms, except anastomosis exercises that were performed as the last exercises. Duration of tasks were measured, and predefined errors were counted. All these were recorded, and completion quality samples were evaluated. Significant p was p < 0.05.
Results:
Significant time reduction and improvement in quality of tasks were observed in favor of Group 3, in all sets for all tasks (p < 0.001). Quality of the tasks was significantly improved in AI-3D in Group 1 and Group 2 for all tasks. Task 5 was the most difficult one and needed more experience to be completed with quality. Even, Group 3 was the experienced group; AI with 3D display enabled Group 3 to improve performance with increased quality without statistical significance.
Conclusion:
The AI-3D visualizing system can provide more successful completion in E-BLUS tasks than CI-2D, AI-2D, and CI-3D visualizing systems for the beginners in urologic laparoscopy, not for experts. Besides, AI with 3D display enable surgeons to improve their performance with increased quality of tasks, in anastomosis.
Introduction
T
However, development of the robot that has fully articulating instruments (AI) with three-dimension (3D) display makes operations easier when compared with conventional instruments (CI) in traditional laparoscopy. 3 We previously published benefits of the 3D visualizing system during laparoscopic radical prostatectomy in terms of reduced operative time, blood loss, and higher early continence rates in comparison with the two-dimension (2D) display system. 4 Besides, we used CI in that study. 4 The fully articulating arms of the robotic system are the distinctive superiorities of the robotic platform. Some reports on articulating devices in laparoscopy pointed out their usefulness. 5
Nevertheless, the robotic-driven motorized handled articulating instruments are new and the only study that was conducted with them was on laparoscopic suturing skills. 6 Their use in laparoscopic surgery is logical. There has not been a study for their benefits on fully laparoscopic validated skills in published literature. These devices may do and rotate as possible as like in robotic surgery. 6
In view of all these, laparoscopic operation via using a 3D visualizing system together with motorized fully articulating devices seems like to make laparoscopic operations familiar and easy to apply. According to our best knowledge, there has not been any published report on the effectivity and availability of these robotic-driven handled instruments with the 3D visualizing system compared with traditional laparoscopic devices and the 2D visualizing system, in validated laparoscopic skills.
Our hypothesis is that articulating devices can make surgeons perform surgical procedures easily with the 3D visualizing system. Having overcome this issue, we used European Training in Basic Laparoscopic Urological Skills (E-BLUS) platforms in training boxes and additional anastomosis task. 7 This is the first and unique study in the literature that compared conventional and motorized articulated devices in laparoscopic training boxes.
Methods
Twenty medical students “without a single independent operative laparoscopy experience,” 20 residents from the department of urology, the department of general surgery, and the department of gynecology with “limited laparoscopy experience,” and 20 expert surgeons with “at least 100 laparoscopic operation experience” were enrolled in the present study. All of them were divided into three groups according to the limit of their laparoscopic experience. Group 1 (n = 20) consisted of medical students, Group 2 (n = 20) consisted of residents, and Group 3 (n = 20) consisted of expert laparoscopic surgeons. The study was approved by our institutes. All participants signed an informed consent form.
The 3DHD Vision System® (Viking Systems, La Jolla, CA) with 30° optic, and the 2D Full-HD Endoscopy System® (Karl Storz, Tuttlingen, Germany) with 30° optic were used. Participants used passive, polarized glasses for display in the 3D system. We used conventional laparoscopic hand devices (Karl Storz, Tuttlingen, Germany) and robotic-driven handheld instruments Kymerax (Terumo, Tokyo, Japan) (Fig. 1). The Kymerax system has six degrees of freedom. Figure 1A shows the device. Movements (six degrees of freedom) of the devices are shown in Figure 1B. In addition, articulation of the devices is presented during operation in Figure 1C, D.
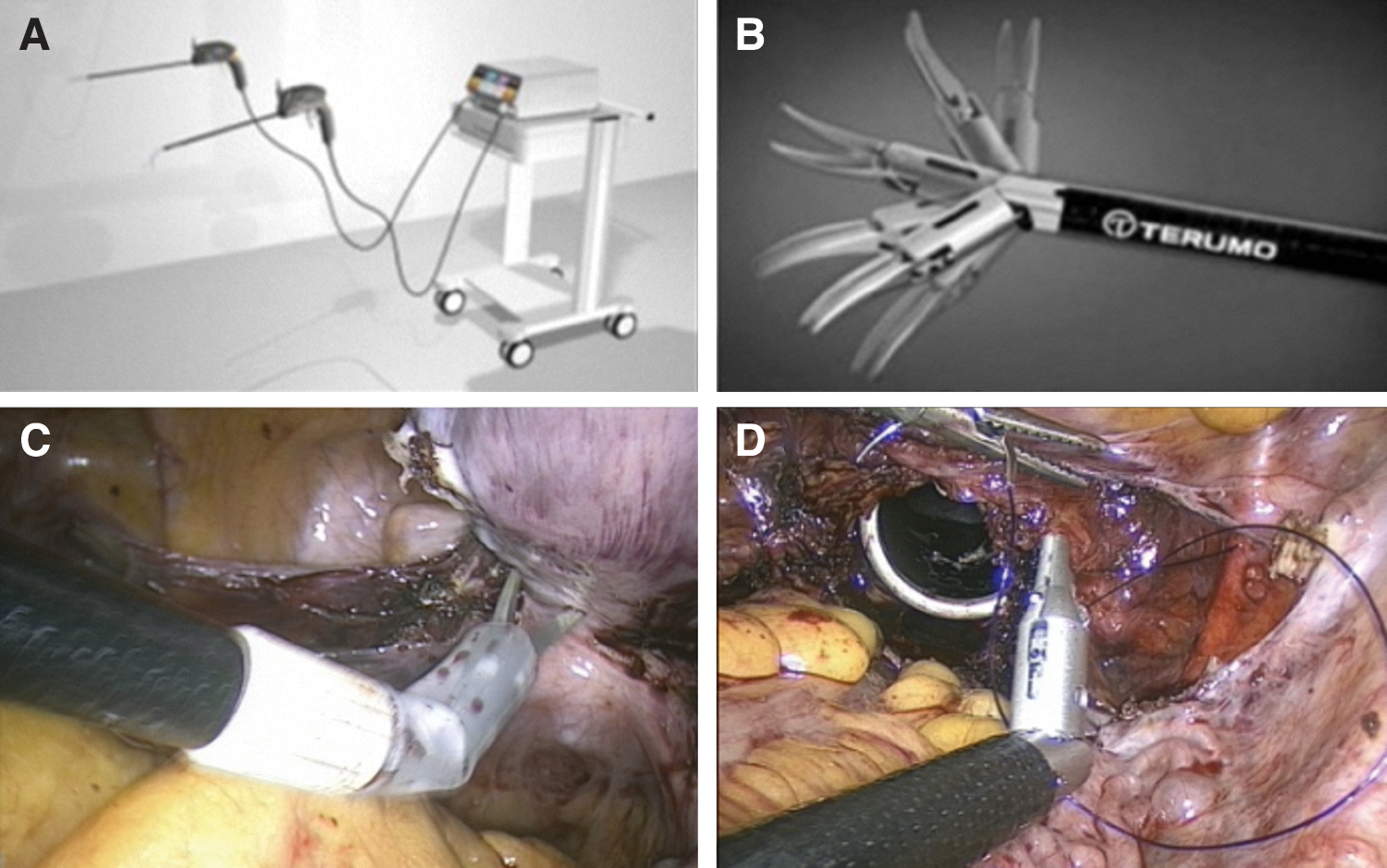
The Kymerax System comprised a console, handles, and interchangeable instruments. These instruments are fully articulated.
Technical platforms were set in the same training boxes as four experimental setups according to E-BLUS (Table 1 and Fig. 2). 7 Briefly, these exercises included peg transfer, cutting between circles, needle guidance, and laparoscopic suturing, respectively. We added the fifth exercise as a vesicourethral anastomosis model (Table 1 and Fig. 2) similar to nonanimal material that was used by Nadu and colleagues. 8
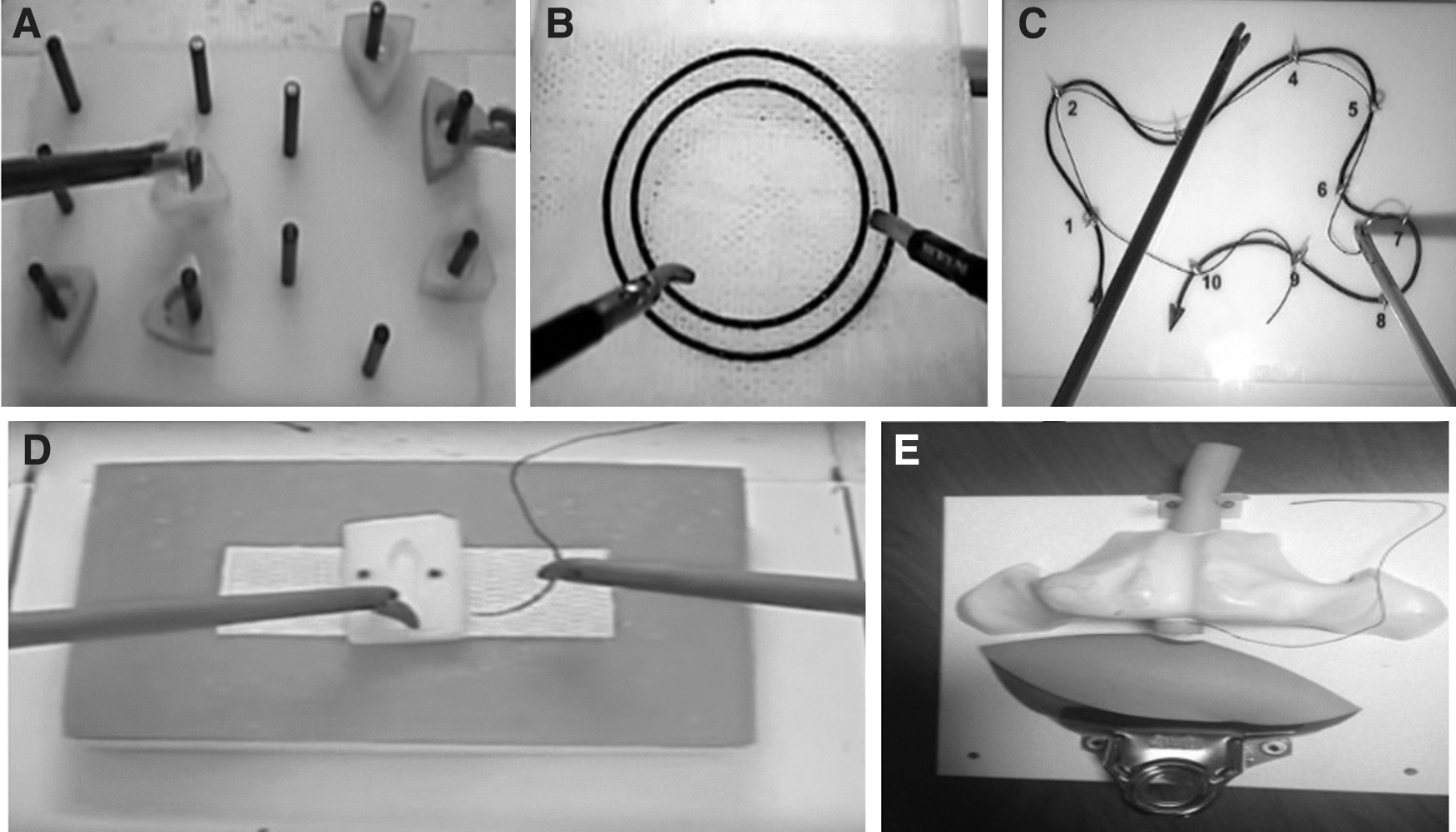
The first 4 tasks were adopted from European training in basic laparoscopic urological skills, and the anastomosis tasks were added.
We set 4 tasks using alterations of the display system and laparoscopic devices as CI with 2D display system (CI-2D), CI with 3D display system (CI-3D), AI with 2D display system (AI-2D), and AI with 3D display system (AI-3D) platforms. All participants were required to perform five different skills in each one of the technical platforms.
After adjustment of light intensity and white balancing for both optical systems, all tasks were performed. The participants were randomly assigned to start with the different technical platform setups except the anastomosis model. They performed anastomosis as the last exercise. They performed the tasks of each technical condition on separate days or after 30 minutes' intervals.
We measured completion time and quality of the finished skills. Procedure finishing times were recorded and compared. All tasks were monitored and recorded to evaluate the quality of participants' manipulations by the responsible expert surgeon (S.A.) of the study by giving points between 1 and 5 for the tasks. The quality standards of tasks 1–4 were described earlier. 7 Quality of anastomosis was assessed as considering intervals between sutures and tightness of the knot.
The SPSS v16.0 were used for statistical analyses. Mean values in groups were compared by using one-way-ANOVA tests. Paired t tests were used for independent variables. Significant p was p < 0.05.
Results
In total, there were 60 participants in three groups and they completed all the tasks. We measured completion time and quality scores for all the tasks. Table 2 presented the comparison of the groups in task 1 (peg transfer). Group 3 was the best in all sets for task 1 (p < 0.001). Interestingly, AI with 3D display enabled all groups to complete the task earlier with higher quality. The higher delta in parameters was observed in Group 1.
Statistical significant p-value.
One-way ANOVA test was used.
CI = conventional instruments; 2D = two dimension; AI = articulating instruments; 3D = three dimension.
Table 3 showed a comparison of groups for task 2 (cutting between circles). The best time to complete is in favor of Group 3 in all sets (p < 0.001). However, time to complete and quality of performed task were significantly improved for Groups 1 and 2 with AI and 3D display.
Statistical significant p-value.
One-way ANOVA test was used.
Table 4 represented a comparison of the groups for task 3 (needle guidance). Similar statistical significant results were obtained in Table 3, in favor of Group 3. However, significant improvement was observed for Groups 1 and 2 in AI with 3D display.
Statistical significant p-value.
One-way ANOVA test was used.
Table 5 showed a comparison of the groups in challenging sets for task 4 (knot tying). Similar results were gained from a comparison in favor of Group 3. The mean time to complete the task results of Group 1 and Group 2 was closed with the results of Group 3 with AI and 3D display.
Statistical significant p-value.
One-way ANOVA test was used.
Table 6 summarized a comparison of groups in different sets of laparoscopic instruments with display systems. Similar significant results were gained for analyses. However, this was the most difficult exercise. The completion time and quality of the task were improved with AI and 3D display set. Besides, all results were in favor of Group 3.
Statistical significant p-value.
One-way ANOVA test was used.
Figure 3 presents the impact of different display systems with chancing laparoscopic devices on outcomes of performed tasks. The mean finishing time was seen. Articulating devices with a 3D display system provided for finishing all tasks earlier than other settings in all groups (Fig. 3A). In addition, the mean quality of performing tasks increased with AI and the 3D set (Fig. 3B).
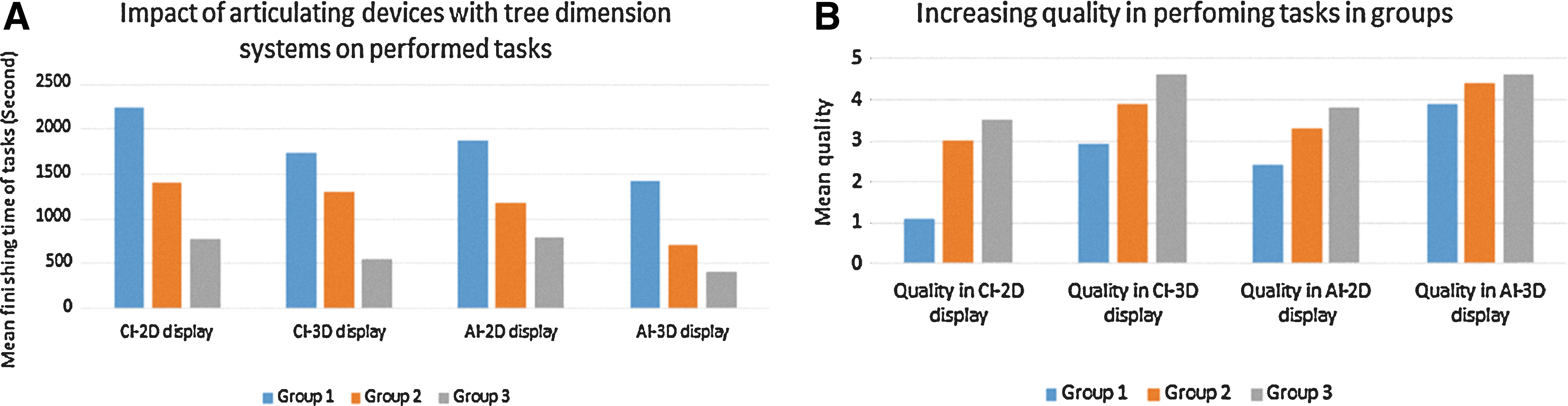
Impact of different display systems with chancing laparoscopic devices on outcomes of performed tasks.
Discussion
We found that laparoscopic skills were easily performed with AI and 3D for beginners and novices. On the other hand, these sets did not affect the performance of experts in laparoscopy. According to the best of our knowledge, these results are unique in that validated laparoscopic skills were examined in AI with the 3D set, in published literature.
In the present study, we preferred to use a validated skill pattern in the training box. Brinkman and colleagues previously published results of E-BLUS, and, thus, we used E-BLUS training skill in our trainings. 9 The E-BLUS is used to teach and learn basic laparoscopic skills worldwide. 7 The first skill was peg transfer, and its aim is ambidexterity. Group 1 was the worst of the table with CI and 2D display. However, the completion time and quality of the skill were improved with AI and 3D display.
Corker and colleagues pointed out to improved skills with articulating devices in peg transfer. 10 Our findings were similar to these. In our previous study, we showed benefits of the 3D display system on outcomes of laparoscopic radical prostatectomy operations. 4 As in task 1, all groups could develop their skills with 3D display when compared with 2D. However, they had great improvement with AI. Expert surgeons improved their skills and they reached the best quality in AI and 3D. However, the quality level was same for them in CI and 3D display, in chancing tasks. These may relate to their experience, and participants in Group 3 are used to perform operations with CI. According to our performed task results, 3D made novices learn laparoscopic skills easier and these did not affect experts. Özsoy and colleagues concluded that laparoscopy with the 3D display system seemed to facilitate the learning for novice surgeons. 11 Our results were in line with them. Interestingly, the quality of the skill with CI with 2D display was similar to AI with the 3D display in Group 3, in E-BLUS tasks, except task 5. The task 5 was the difficult one, including mimic of vesicourethral anastomosis. Performing intracorporeal suturing is annoying during laparoscopic surgery, notably for beginners. In our set, all groups improved completion time and quality of the tasks for task 5 with AI and 3D display.
Klein and colleagues reported importance of the stepwise technique for learning anastomosis in laparoscopy. 12 Pérez-Duarte and colleagues reported their own anastomosis skills. 13 As shown earlier, even novices improved their task quality with 3D display but they had great improvement with AI and the 3D set like experts.
We know our limitations in this study. The low numbers of the participants in groups constitute the first. Of course, there are a lot of tasks in the laparoscopic surgeries but we focused on validated and transferable tasks. Thus, we used E-BLUS with anastomosis skills. We could not show the learning curve of using Kymerax, which can be the subject of a future study. We discussed an optimum device and display system set with the emergence of the robot. The robotic-handled AI and 3D display systems are currently expensive. We believe that when the set of 3D display and AI will spread, the prices will decrease.
We emphasize that Kymerax devices have six degrees of freedom. Thus, this feature can only be optimal in combination with 3D-videotechology. Advanced hand-eye coordination is needed during laparoscopic operations. Because of adaptation probably being difficult, Kymerax devices should be used in dominant hand and traditional laparoscopic devices should be used in nondominant hand at the beginning.
The advantages of the Kymerax can be moved up a step with 3D display systems. Finally, Kymerax devices are not manufactured nowadays. However, we strongly think that six degrees of freedom in laparoscopic hand devices will become very important in the future.
Our results show that beginners can take advantage of the 3D and AI set to make basic laparoscopic skills easier. Experts can also get benefits of these sets in advanced skills such as anastomosis. This is the first article in the published literature that AI with 3D display was evaluated. More randomized controlled trials are needed on this issue.
Conclusion
There is a significant benefit in a simulated setting of AI with 3D display in terms of improving quality scores and completion time of the tasks for beginners and novices in laparoscopy. This operation set may help experts perform difficult skills such as laparoscopic anastomosis. In addition, expert laparoscopic surgeons can reduce time to perform skills. These may be proof that AI and 3D display systems can make surgeons complete surgical tasks fast with better skills. All of these should be checked in validated surgical laparoscopic skills with high numbers of participants.
Footnotes
Author Disclosure Statement
The authors of this study report no conflict of interest.